Abstract
OBJECTIVE:
To perform a review of studies of food consumption and nutritional adaptation in Brazilian infants pointing the main findings and limitations of these studies.
DATA SOURCE:
The articles were selected from Literatura Latino-Americana e do Caribe em Ciências da Saúde (Lilacs) (Latin-American and Caribbean Literature in Health Sciences), Scientific Electronic Library Online (SciELO) and Science Direct in Portuguese and in English. The descriptors were: ''food consumption'', ''nutritional requirements'', ''infant nutrition'' and ''child''. The articles selected were read by two evaluators that decided upon their inclusion. The following were excluded: studies about children with pathologies; studies that approached only food practices or those adaptation of the food groups or the food offert; and studies that did not utilize the Dietary Reference Intakes (DRI).
DATA SYNTHESIS:
Were selected 16 studies published between 2003 and 2013. In the evaluation of the energy consumption, four studies presented energetic consumption above the individual necessities. The prevalence of micronutrients inadequacy ranged from 0.4% to 65% for iron, from 20% to 59.5% for vitamin A, from 20% to 99.4% for zinc, from 12.6% to 48.9% for calcium and from 9.6% 96.6% for vitamin C.
CONCLUSIONS:
The food consumption of Brazilian infants is characterized by high frequencies of inadequacy of micronutrients consumption, mainly iron, vitamin A and zinc. These inadequacies do not exist only as deficiencies, but also as excesses, as noted for energetic consumption.
Keywords: Food consumption, Nutritional requirements, Infant nutrition, Child nutrition
Introduction
Children represent a group of highly vulnerable individuals, due to their rapid growth, physiological and immunological immaturity.1 , 2 Adequate nutrition in the early years of life is essential for healthy growth and development.3 Inadequate nutrient consumption can impair the nutritional status, leading to the development of nutritional deficiencies or excesses.4
Deficiency diseases increase children's susceptibility to diarrhea and infection and can compromise the maturation of the nervous, visual, mental and intellectual systems.5 In Brazil, iron and vitamin A deficiencies are the most often observed micronutrient deficiencies, representing a public health problem.6 , 7 Data from the National Demographic and Health Survey (PNDS), carried out in 2006, show a prevalence of anemia of 20.9% and inadequate levels of vitamin A in 17.4% of children younger than five years.8
With the nutritional transition, obesity and overweight, which reflect excessive energy consumption and / or insufficient energy expenditure, have shown a high prevalence in the Brazilian pediatric population. The Household Budget Survey (2008-2009) demonstrated the evolution of anthropometric indicators of Brazilian children aged five to nine years, showing an increase of overweight of 10.9% in 1974-1975 to 34.8% in 2008-2009 in boys and from 8.6% to 32% in girls, in the same period.9
Infant feeding practices should be able to provide enough food, with nutritional and sanitary quality, to meet the nutritional needs of children and ensure the development of their full potential.10 Proper nutrition in childhood contributes to the establishment of healthy eating habits, which will have an impact not only in the short term, but also in adulthood.3 Children with inadequate food intake since childhood tend to the early development of overweight and obesity, as well as other associated chronic diseases.11 On the other hand, children submitted to optimal feeding practices reach their normal development and become healthier adults, with greater intellectual and productive capacity.12
Considering the importance of adequate dietary intake in childhood to reach the nutritional needs, this article aims to perform a systematic review of studies on food consumption and nutritional adequacy in Brazilian children, pointing out the main findings and limitations of these studies.
Method
This is a systematic review of the literature based on the analysis of studies related to food consumption and nutritional adequacy of Brazilian children. Articles were selected by searching the Latin American and Caribbean Literature on Health Sciences (LILACS), Scientific Electronic Library Online (SciELO) and Science Direct databases in December 2013. The descriptors used in the search for articles were chosen after consulting the "Descriptors in Health Sciences (DeCS)". The following descriptors and their combinations in Portuguese and English were used: "Food Consumption" ("Consumo Alimentar"), "nutritional requirements", ("Necessidades nutricionais"), "Infant nutrition" ("Nutrição do lactente") and Child (Criança).
This review included articles published in Portuguese and English, carried out with Brazilian children aged 0 to 10 years that addressed the subject of food consumption in childhood and nutritional adequacy in quantitative terms. There was no limitation regarding the year of publication of the articles. Studies with children with any type of pathology; those that addressed inadequate feeding practices without quantitatively expressing the inadequacies in nutrient intake; the ones that assessed the adequacy of food groups only, but not of nutrients; the ones that analyzed the food offered to children without verifying consumption; and manuscripts that did not use the Dietary Reference Intakes (DRI) to verify nutritional adequacy were excluded.
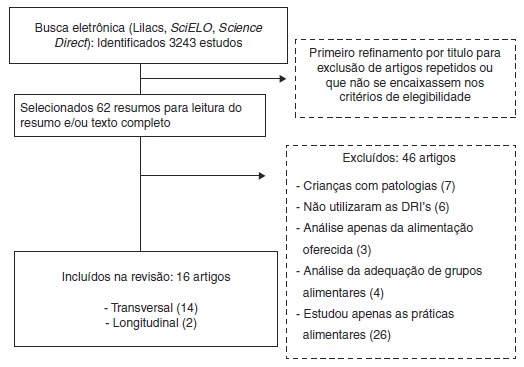
A total of 3,234 studies were identified in the database search. Subsequently, we performed an analysis by title to exclude repeated articles or articles that did not meet the predefined criteria, which resulted in 62 articles. After this phase, summaries or full texts were read in their entirety to verify the inclusion and exclusion criteria. The selected articles were read by two examiners who decided on their inclusion based on the eligibility criteria. Each examiner independently decided by "inclusion" or "exclusion" and discrepant results were reassessed by the examiners.
A total of 16 studies were selected for this review: 14 cross-sectional and two longitudinal studies, published between 2003 and 2013, which quantitatively evaluated dietary intake of Brazilian children (Fig. 1).
Figure 1. Flowchart of article search.

Results
Table 1 shows the methodological aspects concerning the site and types of studies, the dietary survey used to assess dietary intake, sample group and objectives of the assessed studies.
Table 1. Methodological aspects and objective of the selected studies.
| Author/Year | Place and type of study | Food inquiry (N. of days it was applied) | Sample group | Objective |
|---|---|---|---|---|
| Spinelli et al., 2003 16 | São Paulo (SP) Cross-sectional |
Weighed food records (5 days) | Total: 106 children aged 6-18 months; | Verify children’s food intake and assess nutrient adequacy |
| Groups: 6-9; 9-12 months; 12-18 months | ||||
| Cavalcante et al., 2006 4 | Viçosa (MG) Cross-sectional | 24-hour recall (1 day); | Total: 174 children aged 12-35 months; | To assess dietary intake and nutritional status of children enrolled in public health care services |
| Food Frequency Questionnaire (once) | Groups: male and female | |||
| Barbosa et al., 2007 18 | Paquetá (RJ) Longitudinal |
Dietary history (once); Direct weighing of food (two days); Food diaries (two days) |
Total: 35 children aged 2 and 3 years; Groups: at enrollment (time 1) and after 6 months in daycare (time 2) |
Compare the adequacy of nutrient intake in children from a non-profit daycare |
| Fidelis; Osório, 2007 3 | Metropolitan Region of Recife, Urban countryside and Rural countryside (PE). Cross-sectional | 24-hour recall (1 day) | Total: 948 children aged < 5 years | Evaluate the dietary intake of macro and micronutrients of children |
| Groups: 0-6 and 7-11 months; 1-3 and 4-8 years | ||||
| Menezes; Osório, 2007 20 | Pernambuco Cross-sectional |
24-hour recall (1 day) | Total: 948 children aged <5 years; | Assess the intake of energy and protein and associate it with the nutritional status of children |
| Groups: 0-6; 7-11; 12-47 and 48-60 months | ||||
| Alves et al., 2008 21 | Umuarama (PR) | Weighed food records (1 day) | Total: 54 children aged 4-6 years | Perform anthropometric and dietary intake assessment of children in day care |
| Cross-sectional | ||||
| Antunes et al., 2010 13 | Duque de Caxias (RJ) | 24-hour recall (2 days) | Total: 384 children aged 6-30 months; | Describe the association between food insecurity and child food consumption |
| Cross-sectional | Groups: Food Security; Mild Food Insecurity; Moderate and Severe Food insecurity | |||
| Caetano et al., 2010 22 | Curitiba (PR), São Paulo (SP) and Recife (PE) Longitudinal |
Food diaries (7 consecutive days) | Total: 179 children aged 4-12 months; Groups: <6 and 6-12 months |
Evaluate practices and food consumption in healthy infants from three cities of Brazil |
| Gomes; Costa; Schmitz, 2010 17 | Brasília (DF) Cross-sectional |
Weighed food records (three days); 24-hour recall (3 days) |
Total: 678 children aged 4-82 months; Groups: 4-12 and 13-82 months |
To assess dietary intake of children from no-profit daycare centers |
| Martino et al., 2010 23 | Alfenas (MG) | Weighed food records (1 day); | Total: 186 children aged 12-72 months; |
Assess socioeconomic, nutritional status and dietary intake of preschoolers attended by Municipal Educational Centers (EMC) |
| Cross-sectional | ||||
| Silva et al., 2010 24 | Maceió (AL) | 24-hour recall (1 day) | Total: 272 children aged 1-8 years | To assess dietary intake of energy, macronutrients and micronutrients related to growth and development |
| Cross-sectional | ||||
| Bernardi et al., 2011 5 | Caxias do Sul (RS) | Individual weighed food record (1 day); Food diary (1 day) |
Total: 362 children aged 24-72 months | Assess the dietary intake of micronutrients in preschool children at home and in public and private kindergartens |
| Cross-sectional | ||||
| Costa et al., 2011 14 | Gameleira (PE) and São João do Tigre (PB) | 24-hour recall (1 day) | Total: 445 children aged 0-23 months: 238 in Gameleira and 207 in São João do Tigre | Evaluate the dietary intake of children |
| Cross-sectional | ||||
| Paiva-Bandeira et al., 2011 25 | João Pessoa (PB) Cross-sectional |
Quantitative Food Frequency Questionnaire (once) |
Total: 183 children aged 2-10 years | Analyze the association between income and food consumption of b-carotene, vitamin C and vitamin E in children |
| Tavares et al., 2012 15 | Manaus (AM) Cross-sectional |
Individual weighed food record (1 day); |
Total: 308 children aged 24-72 months: 217 from public daycare and 91 from private daycare centers | Verify the nutritional status and dietary intake of children in day care centers |
| Food diary (1 day) |
||||
| Bueno et al., 2013 19 | Brazil Cross-sectional |
Individual weighed food record (1 day); |
Total: 3058 children aged 2-6 years in public and private schools | Estimate the nutritional risk of children |
| Food diary (1 day) |
When assessing energy consumption in children, the studies by Cavalcante et al.,4 Antunes, Sichieri and Salles-Costa,13 Costa et al.14 and Tavares et al.15 were the ones that showed energy consumption above the individual needs calculated by the Estimated Energy Requirements (EER). The studies by Spinelli et al.,16 Fidelis and Osório3 and Gomes et al.17 highlight the protein intake above the recommended levels among the assessed children.
When assessing micronutrient intake, we observe that most studies demonstrate the inadequacy of iron, vitamin A and zinc levels. The prevalence of inadequacy ranged from 0.4% to 65% for iron, from 20.0% to 59.5% for vitamin A, from 20.0% to 99.4% for zinc, from 12.6% to 48.9% for calcium and from 9.6% to 96.6% for vitamin C. Table 2 shows the results of assessed studies.
Table 2. Summary of the main results of each study that assessed the adequacy of food consumption in children.
| Author/Year | Results |
|---|---|
| Spinelli et al., 2003 16 | Adequacy of children aged 6 to 9 months, 9 to 12 months and 12 to 18 months |
| Energy (58.9%. 58.9% and 57.0%); | |
| PTN (145.9%. 158.3% and 189.6%); | |
| Vit A (92.2%. 98% and 95.1%); | |
| Vit C (118.1%. 114.0% and 111.8%); | |
| Iron (38.4%. 45.9% and 52.2%); | |
| Calcium (109.1%. 114.5% and 73.8%) | |
| Cavalcante et al., 2006 4 | Prevalence of inadequacy |
| Vit. C (96.6%) | |
| Vit. A (36.8%) | |
| Iron (13.2%) | |
| Zinc (99.4%) | |
| Barbosa et al., 2007 18 | Apparent intake adequacy |
| Moment 1: PTN (0.93%); Iron (0.63%); Vit C (0.59%); Calcium (0.57%); Fibers (0.10%); | |
| Moment 2: PTN (0.99%); Iron (0.86%); Vit C (0.91%); Calcium (0.70%);
Fibers (0.20%) | |
| Fidelis; Osório, 2007 3 | Prevalence of inadequacy |
| Energy: 49% (0 to 6 months); 41.4% (1 to 3 years); 55.2% (4 to 5 years); | |
| Vit. A: 44% (1 to 3 years); 59.5% (4 a 5 years); | |
| Iron: 65% (7 to 11 months); 23.7% (1 to 3 years); 22.4% (4 to 5 years); | |
| Zinc: 57.3% (7 to 11 months); 43.7% (1 to 3 years); 52.6% (4 to 5 years) | |
| Menezes; Osório, 2007 20 | Prevalence of Inadequacy |
| Energy: 49% (0 to 6 months); 26.5% (7 to 11 months); 41.4% (12 to 47 months); 55.2% (48 to 60 months); | |
| PTN: 6.0% (7 to 11 months); 4.4% (12 to 47 months); 6.9% (48 to 60 months) | |
| Alves et al., 2008 21 | Adequacy in relation to recommended amounts |
| Energy (47.9%); PTN (106.7%); LIP (56.7%); CHO (65.6%); Fibers (21.6%) | |
| Calcium (14.9%); Iron (36.4%); Sodium (167.6%) | |
| Antunes et al., 2010 13 | Prevalence of inadequacy in children on Food Security |
| Energy (28.3%); PTN (3.6%); CHO (24.4%); LIP (1.1%); Iron (33.6%) | |
| Prevalence of inadequacy in children on moderate and severe food
insecurity | |
| Energy (30.5%); PTN (8.9%); CHO (22.9%); LIP (7.0%); Iron (64.3%) | |
| Caetano et al., 2010 22 | Prevalence of inadequacy for children aged 6 to 12 months |
| Vit. B3 (53%); Vit E (47%); Vit A (38%); Zinc (75%); Iron (45%) | |
| Gomes; Costa; Schmitz, 2010 17 | Prevalence of inadequacy |
| Children aged 7 to 12 months → Iron (56.5%) | |
| Children aged ≤12 months → 100% higher consumption than AI for CHO. PTN. vitamins B1. B2. B12. B6 and zinc | |
| Children ≥12 months → Vit. E (53.2%) and Vit. B9 (90%) | |
| Martino et al., 2010 23 | Adequate energy intake: 78.4% (from 1 to 3 years); |
| Excess energy intake: 72.6 % and 74.1% (from 4 to 6 years); | |
| Adequacy from 1 to 3 years: Calcium (27.9%); Iron (150%); | |
| Adequacy from 4 to 6 years: Calcium (22.8%); Iron (146.3%) | |
| Silva et al., 2010 24 | Adequate energy intake: 84,4% (1 a 3 years); 95,2% (3 a 8 years); |
| Excess energy intake: 15.6% (1 to 3 years); 1.2% (3 to 8 years); | |
| Frequency of inadequacy (1 to 3 years) | |
| Vit A (>40%); Vit C (20%); Vit E (100%); Iron: (>40%); Zinc (>40%); | |
| Frequency of inadequacy(4 to 8 years) | |
| Vit A (>20%); Vit C (10%); Vit E (>30%); Iron (>40%); Zinc (>20%) | |
| Bernardi et al., 2011 5 | Prevalence of inadequacy Calcium: 33.7% and 32.2% (Public School and Private School) |
| Costa et al., 2011 14 | Prevalence of inadequacy from 7 to 11 months (Gameleira and São João
do Tigre) |
| Energy: 23.9% and 30.5%; | |
| PTN: 9.8% and 13.5%; | |
| Iron: 45.6% and 61.0%; | |
| Zinc: 31.3% and 36.3%; | |
| Prevalence of inadequacy from 12 to 23 months (Gameleira and São João do Tigre) | |
| Energy: 23.6% e 23.9%; | |
| Vit. C: 23.9% e 28.1%; | |
| Iron: 25.1% e 15.4%; | |
| Zinc: 23.3% e 25.8 | |
| Paiva-Bandeira et al., 2011 25 | Prevalence of inadequacy: |
| Vit C: 9.6% (4 to 8 years); 10% (9 to 10 years); | |
| Vit E: 41.7% (2 to 3 years); 59.6%(4 to 8 years); 75% (9 to 10 years) | |
| Tavares et al., 2012 15 | Prevalence of inadequacy |
| Energy: 40% > EER; Calcium: 27.6%; Vitamin D: 25.8% | |
| Vitamins A and C, zinc and sodium exceeded more than 70% UL | |
| Bueno et al., 2013 19 | Prevalence of inadequacy: |
| Public School: Iron (0.4%); Calcium (12.6%); Vit. D (93.6%) (2-3 years) | |
| Private School: Iron (<0.001%); Calcium (13.6%; Vit. D (92.3%) (2-3 years) | |
| Public School: Iron (<0.001%); Calcium (48.9%); Vit. D (90.9%) (4-6 years) | |
| Private School: Iron (<0.001%); Calcium (40.3%); Vit. D (94.1%) (4-6 years) |
Vit, vitamin; EER, Estimated Energy Requirement; EAR, Estimated Average Requirement; AI, Adequate Intake; CHO, carbohydrates; PTN, protein; LIP, lipid.
In this article, eight studies assessed the dietary intake of institutionalized children, especially in public and private day care centers. Six publications used only one 24-hour recall record. Among the eight studies that applied weighed food records, five did so on a single day.
The study by Barbosa et al.18 performed the calculation of the apparent adequacy in the analysis of food intake in 35 children in Paqueta-RJ. Among the other assessed studies, 15 used the Estimated Average Requirements (EAR) as the cutoff and only one used RDA (Recommended Dietary Allowance). Among the studies that estimated the prevalence of inadequate nutrient consumption based on EAR, only five made the adjustment for intra-individual variability.5 , 14 , 15 , 17 , 19
Discussion
Among the studies that assessed children's energy intake,3 - 5 , 14 - 24 four showed energy consumption above the individual requirements4 , 14 , 15 , 19 and three3 , 16 , 23 showed insufficient energy intake among the assessed children.
Costa et al.14 observed mean energy and macronutrient consumption above the recommended amounts, with the exception of children aged 7-11 months, who had inadequate energy consumption. The diet of these children was characterized as dull, with high consumption of sugar and fat, and low in micronutrients. Tavares et al.15 emphasize that the high percentage of children with excess weight can be explained by the high energy intake observed in more than 40% of the children. As an effect of high energy consumption, there is a higher frequency of overweight and obesity, as well as micronutrient deficiencies due to poor diet quality.26 The high protein intake observed in some studies is a marker of the diet quality of these children, as it may be a protective factor against protein-energy malnutrition.20 In situations of unbalanced consumption of other macronutrients, protein can have its function diverted and used to supply energy.16
This review showed that micronutrient levels most often found to be inadequate in children were iron, vitamin A and zinc. Iron deficiency is associated with an increase in frequency and duration of infections, changes in growth and development, cognitive acquisition and intellectual performance impairment.27 Children are particularly at risk for this deficiency, mainly due to inadequate dietary habits during childhood. Some of the main ones are: delayed introduction of iron-rich foods (meats, for instance), weaning and early introduction of cow's milk.28
The low prevalence of exclusive breastfeeding up to six months of age in Brazil has been documented in the literature29 , 30 and represents an important risk factor for inadequate iron consumption. Breast milk is often replaced by cow's milk, which has lower iron bioavailability, in addition to causing intestinal microbleeds.28 In Brazil, the prevalence of iron deficiency is high, especially in children aged 6-24 months due to the increased need for this micronutrient in this phase.6 , 31 In order to fight this deficiency, the Brazilian government has created the National Iron Supplementation Program, which proposes preventive supplementation of this nutrient for children aged 6 to 18 months in the entire country. Although this supplementation has occurred since 2005, currently the prevalence of iron deficiency is still high.6 , 32 This demonstrates the complexity of the nutritional adequacy of this nutrient, which is not limited to supplementation, but requires a network of actions ranging from the increase in the population's level of schooling to the promotion of exclusive breastfeeding until six months of age.33
Vitamin A deficiency is the leading cause of preventable blindness worldwide and even in milder cases, it can lead to a compromised immune system and increased childhood morbidity and mortality.7 The study by Caetano et al.22 demonstrated inadequate feeding practices, such as the short duration of exclusive breastfeeding, use of whole cow's milk and the early introduction of processed foods rich in lipids, sugar and salt to children aged 4-12 months. As a consequence of this diet, we observed a high prevalence of inadequacy for several micronutrients, including vitamin A. Similarly to the strategy adopted for iron, Brazil also created the Vitamin A Supplementation Program to fight deficiency of this vitamin. However, the prevalence of vitamin A deficiency remains high in Brazil, indicating the need for further actions that encourage greater consumption of this nutrient by Brazilian children.5
From the sixth month, approximately 70% of the infant's iron and zinc requirements must be met through adequate complementary feeding.22 Imbalances in complementary feeding can cause damage to the adequacy of zinc in children. The study by Palmeira et al.2 observed a higher intake of dairy meals instead of other foods. This dietary practice may involve the lower consumption of meats and thus impair the consumption of zinc, as these are the main source of this nutrient in the child's diet.34
Analysis of institutionalized children's food intake was assessed in seven studies of this review. Martino et al.,23 when assessing children attending Municipal Educational Centers (EMC), found that the food consumption covered more than 70% of energy requirement and the distribution of macronutrients was adequate, although the intake of calcium and iron was inadequate. However, this study only evaluated the dietary intake of these children at the institution and not at home, where the intake can be supplemented and contribute to the achievement of these recommendations.35
Tavares et al.15 observed that food consumption did not differ between public and private day care centers. The authors of this study point out that the nutritional adequacy of children is more often related to the frequency of attendance at the daycare than to the type of day care (public or private). In the study by Bernardi et al.,5 although children attending private schools had better consumption than the ones in public schools, the latter showed no risk at the intake, as the recommendations were reached with the food received at home. Therefore, the analysis of total dietary intake of these children, considering the school and home, did not differ between the types of school.
The studies by Alves et al.21 and Gomes et al.17 demonstrated the need to adapt the diet consumed by children in the institutions. This indicates the need for greater caution regarding the proposed feeding recommendations at the institutional level. The National School Feeding Program (PNAE) is the oldest social program of the federal government and constitutes an important government strategy to ensure Food and Nutrition Security among the population.36 One aim of the program is to meet the nutritional needs of public school students during the period they are at school, in order to contribute to the adequate development and learning, as well as to improve school performance.37 In day care centers where children stay full-time, all the meals offered must provide at least 70% of the daily nutritional needs. It is supposed that the 30% complementation occurs at home, which can lead both to nutritional adequacy and excess, if there is no qualitative and quantitative balance.35
Children aged 7 months to 5 years that stay only part-time in the institution, must receive two meals that provide 30% of the daily nutritional needs. For schoolchildren aged 6 to 10 years, who usually stay at school part-time, 20% of the nutritional needs must be provided. The reach of these percentages in the meals offered in day-care centers and schools is an important action to contribute to the nutritional adequacy of Brazilian children attending the public education network.37
Studies carried out in institutions show very different results of nutritional adequacy depending on the type of school, but they seem to indicate that children that receive their meals at school are more protected from inadequacies in their total consumption. And as observed in the study by Barbosa et al., 18 attending day care seems to improve the children's dietary profile.
It is noteworthy that the different methods used to analyze food intake in several studies is a factor that may contribute to result variability. The most often used tools were the 24-hour recall and weighed food record. It is essential to choose the most adequate method to assess dietary intake for increased estimate reliability. As no method of assessing dietary intake is free of errors, the choice of the dietary survey should take into account the aims of the study, age, gender and the agreement of the methods regarding their application and accuracy.38 In this review, six studies associated more than one type of food intake assessment method. A combination of methods is commonly used in studies with children when they want to evaluate daily consumption in daycare and also at home.
The number of days of survey application is an important aspect to consider, as by increasing the number of days one can minimize the effects of intra-individual variability.39 In population studies, the application of 24-hour recalls for two nonconsecutive days seems to have similar results to applications for more days. To obtain the mean consumption by direct weighing, the application for 3 non-consecutive days is recommended.40 In this article, only two studies applied the 24-hour recalls for more than a day. It is noteworthy that the application of a single 24-hour recall or food record does not reflect the individual's usual intake and the use of repeated measures (repeating the survey with part of the sample) with correction of intra-individual variability is necessary to prevent under or overestimation of the results. The study by Verly-Jr et al.41 investigated the accuracy of estimates of usual intake using different replication rates in different sample sizes. It was observed that it was necessary to repeat the measurement at least in 40% of the sample, as the accuracy of usual intake estimates decreased when low replication rates used were.
The calculation of the apparent adequacy allows estimating the level of reliability at what the intake of a nutrient meets the individual's need, comparing the reported intake and that the EAR.42 Therefore, it is necessary to consider the intra-individual variability, as food consumption of the same individual varies from day to day, as well as the variability of needs, because even at the same stage of life, there are differences in the needs of each individual.39 Recently, Castro et al.43 estimated values of intraand interpersonal variance for children aged 1-6 years through multilevel analysis, in addition to calculating the rate of variation and the number of days of dietary assessment of energy and nutrients, according to age and body weight. However, there are no Brazilian studies for the other age groups of children that have evaluated the intra-and interpersonal variability and, therefore, American data are still used. It is worth mentioning that this type of analysis should only be used for the evaluation of individuals, being inadequate for population groups.
One study was found22 that used RDA values as a cutoff to calculate the prevalence of inadequate dietary intake. This is an inadequate method to evaluate the prevalence of inadequacies, as the RDA values refer to consumption goals and not need estimates. Therefore, it is possible that the results of this study overestimated the prevalence of inadequacy.
EAR represents the value of a nutrient intake that meets the mean estimated needs according to the phase of life and gender.44 , 45 EAR, as a cutoff, is a simplified method of probabilistic approach, which allows the assessment of inadequate consumption of population groups.45 Among the studies that comprised this review, most used EAR as a cutoff to calculate the prevalence of micronutrient inadequacy. This is the correct approach for group analysis; however, it is necessary to perform control by intra-individual variability to obtain a better estimate. To calculate the prevalence of inadequate consumption, it is necessary to obtain the intrapersonal and interpersonal variances through the analysis of variance (ANOVA).38 For that purpose, we need at least two independent measurements of each individual's diet, i.e., assessment of food consumption for at least two days. To remove the intra-individual variability, the methods most often used are those of the National Research Council / Institute of Medicine, Iowa State University, Iowa State University Foods, Best-Power and National Cancer Institute. 46 , 47 After applying these methods, the adjusted distribution reflects only the interpersonal variability.42 Most studies3 , 4 , 13 , 16 , 18 , 20 - 25 did not perform the intra-individual variability control and, therefore, their results should be viewed with caution, as the prevalence of inadequacy may be overestimated. Statistical adjustments for food consumption analysis must be used to obtain more reliable results about the individuals' usual consumption. Failure to use these techniques is an important limitation of some of the analyzed studies.
The results of the studies compiled in this review can be considered representative of Brazilian children, as they include several age ranges, socioeconomic strata, regions of the country and urban and rural areas. The PNDS, carried out with a representative sample of children younger than five years in the five Brazilian macroregions, in urban and rural areas, found a high prevalence of anemia and inadequate levels of vitamin A, characterizing public health problems.8 The results of this study agree with those shown in the studies of this review; however, they did not cover all age ranges of childhood and evaluated only the micronutrients iron and vitamin A.
Conclusion
The dietary intake of Brazilian children shows high prevalence of inadequate consumption of micronutrients, especially iron, vitamin A and zinc. This inadequate consumption is not due only to deficiency, but also to excess, as observed for energy consumption in some studies of this review. This profile discloses the children's poor quality of the diet, which despite showing energy intake that is even higher than the recommended amounts, have significant nutritional deficiencies in terms of micronutrients.
The observed inadequacies are probably due to incorrect dietary practices in infancy, mainly represented by the early cessation of breastfeeding, inadequate introduction of complementary foods, excessive consumption of industrialized products that are rich in sugars, fat and salt.
Institutionalization seems to have a protective effect on children regarding the best nutritional adequacy, as they complement the meals provided at home. However, analysis of the studies does not allow us to conclude whether the type of school or daycare influences the nutritional adequacy.
Finally, it is noteworthy the difficulties comparing the studies due to the methodological differences between them, both in relation to the methods used in assessing the diet, as well as the result analysis.
Footnotes
Funding This study did not receive funding.
References
- 1.Lima DB, Fujimori E, Borges AL, Silva MM. Feeding in the two first years of life. Rev Esc Enferm USP. 2011;45:1705-9. [DOI] [PubMed]; Lima DB, Fujimori E, Borges AL, Silva MM. Feeding in the two first years of life. Rev Esc Enferm USP. 2011;45:1705–1709. doi: 10.1590/s0080-62342011000800012. [DOI] [PubMed] [Google Scholar]
- 2.Palmeira PA, Santos SM, Vianna RP. Feeding practice among children under 24 mouths in the semi-arid area of Paraíba, Brazil. Rev Nutr. 2011;24:553-63.; Palmeira PA, Santos SM, Vianna RP. Feeding practice among children under 24 mouths in the semi-arid area of Paraíba, Brazil. Rev Nutr. 2011;24:553–563. [Google Scholar]
- 3.Fidelis CM, Osório MM. Dietary intake of macro and micronutrients by children under five years of age in the State of Pernambuco, Brazil. Rev Bras Saude Mater Infant. 2007;7:63-74.; Fidelis CM, Osório MM. Dietary intake of macro and micronutrients by children under five years of age in the State of Pernambuco, Brazil. Rev Bras Saude Mater Infant. 2007;7:63–74. [Google Scholar]
- 4.Cavalcante AA, Tinôco AL, Cotta RM, Ribeiro RC, Pereira CA, Franceschini SC. Food consumption and nutritional profile of children seen in public health services of Viçosa, Minas Gerais, Brazil. Rev Nutr. 2006;19:321-30.; Cavalcante AA, Tinôco AL, Cotta RM, Ribeiro RC, Pereira CA, Franceschini SC. Food consumption and nutritional profile of children seen in public health services of Viçosa, Minas Gerais, Brazil. Rev Nutr. 2006;19:321–330. [Google Scholar]
- 5.Bernardi JR, Cezaro CD, Fisberg RM, Fisberg M, Rodrigues GP, Vitolo MR. Dietary micronutrient intake of preschool children at home and in kindergartens of the municipality of Caxias do Sul (RS), Brazil. Rev Nutr. 2011;24:253-61.; Bernardi JR, Cezaro CD, Fisberg RM, Fisberg M, Rodrigues GP, Vitolo MR. Dietary micronutrient intake of preschool children at home and in kindergartens of the municipality of Caxias do Sul (RS), Brazil. Rev Nutr. 2011;24:253–261. [Google Scholar]
- 6.Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. In: Programa Nacional de Suplementação de Ferro: manual de condutas gerais. Brasília: Ministério de Saúde; 2013.; Brasil . Programa Nacional de Suplementação de Ferro: manual de condutas gerais. Brasília: Ministério de Saúde; 2013. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. [Google Scholar]
- 7.Miglioli TC, Fonseca VM, Gomes Junior SC, Lira PI, Batista Filho M. Vitamin A deficiency in mothers and children in the state of Pernambuco. Cienc Saude Colet. 2013;18:1427-40. [PubMed]; Miglioli TC, Fonseca VM, Gomes SC, Junior, Lira PI, Batista M., Filho Vitamin A deficiency in mothers and children in the state of Pernambuco. Cienc Saude Colet. 2013;18:1427–1440. [PubMed] [Google Scholar]
- 8.Brasil. Ministério da Saúde. Centro Brasileiro de Análise e Planejamento. PNDS 2006: dimensões do processo reprodutivo e da saúde da criança Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/pndscriancamulher.pdf. Acessado em 20 mar 2014.; Brasil.Ministério da Saúde. Centro Brasileiro de Análise e Planejamento PNDS 2006: dimensões do processo reprodutivo e da saúde da criança. 2006. [20 mar 2014]. a Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/pndscriancamulher.pdf.
- 9.Brasil. Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares 2008-2009: antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil. Disponível em: http://ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/20082009encaa/pof20082009encaa.pdf. Acessado em 10 mar 2014.; Brasil.Instituto Brasileiro de Geografia e Estatística Pesquisa de Orçamentos Familiares 2008-2009: antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil. 2009. [10 mar 2014]. a Available from: http://ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/20082009encaa/pof20082009encaa.pdf.
- 10.Nejar FF, Segall-Corrêa AM, Rea MF, Vianna RP, Panigassi G. Breastfeeding patterns and ernergy adequacy. Cad Saude Publica. 2004;20:64-71. [DOI] [PubMed]; Nejar FF, Segall-Corrêa AM, Rea MF, Vianna RP, Panigassi G. Breastfeeding patterns and ernergy adequacy. Cad Saude Publica. 2004;20:64–71. doi: 10.1590/s0102-311x2004000100020. [DOI] [PubMed] [Google Scholar]
- 11.Oliveira S, Filha E, Araújo JS, Barbosa JS, Gaujac DP, Santos CF, Silva DG. Consumption of food groups among children attending the public health system of Aracaju, Northeast Brazil, in Sergipe. Rev Paul Pediatr. 2012;30:529-36.; Oliveira S, Filha E, Araújo JS, Barbosa JS, Gaujac DP, Santos CF, Silva DG. Consumption of food groups among children attending the public health system of Aracaju, Northeast Brazil, in Sergipe. Rev Paul Pediatr. 2012;30:529–536. [Google Scholar]
- 12.Penn H. Primeira infância: a visão do banco mundial. Cad Pesq. 2002;115:7-24.; Penn H. Primeira infância: a visão do banco mundial. Cad Pesq. 2002;115:7–24. [Google Scholar]
- 13.Antunes MM, Sichieri R, Salles-Costa R. Food intake among children under three years of age in area with high food insecurity. Cad Saude Publica. 2010;26:1642-50. [DOI] [PubMed]; Antunes MM, Sichieri R, Salles-Costa R. Food intake among children under three years of age in area with high food insecurity. Cad Saude Publica. 2010;26:1642–1650. doi: 10.1590/s0102-311x2010000800017. [DOI] [PubMed] [Google Scholar]
- 14.Costa EC, Silva SP, Lucena JR, Batista Filho M, Lira PI, Ribeiro MA, et al. Food consumption of children from cities with a low human development index in the Brazilian Northeast. Rev Nutr. 2011;24:395-405.; Costa EC, Silva SP, Lucena JR, Batista M, Filho, Lira PI, Ribeiro MA. Food consumption of children from cities with a low human development index in the Brazilian Northeast. Rev Nutr. 2011;24:395–405. [Google Scholar]
- 15.Tavares BM, Veiga GV, Yuyama LK, Bueno MB, Fisberg RM, Fisberg M. Nutritional status and energy and nutrients intakes of children attending day-care centers in the city of Manaus, Amazonas, Brazil: are there differences between public and private day-care centers. Rev Paul Pediatr. 2012;30:42-50.; Tavares BM, Veiga GV, Yuyama LK, Bueno MB, Fisberg RM, Fisberg M. Nutritional status and energy and nutrients intakes of children attending day-care centers in the city of Manaus, Amazonas, Brazil: are there differences between public and private day-care centers. Rev Paul Pediatr. 2012;30:42–50. [Google Scholar]
- 16.Spinelli MG, Goulart RM, Santos AL, Gumiero LD, Farhud CC, Freitas EB, et al. Consumo alimentar de crianças de 6 a 18 meses em creches. Rev Nutr. 2003;16:409-14.; Spinelli MG, Goulart RM, Santos AL, Gumiero LD, Farhud CC, Freitas EB. Consumo alimentar de crianças de 6 a 18 meses em creches. Rev Nutr. 2003;16:409–414. [Google Scholar]
- 17.Gomes RC, Costa TH, Schmitz BA. Dietary assessment of pre-school children from Federal District Brazil. ALAN. 2010;60:168-74. [PubMed]; Gomes RC, Costa TH, Schmitz BA. Dietary assessment of pre-school children from Federal District Brazil. ALAN. 2010;60:168–174. [PubMed] [Google Scholar]
- 18.Barbosa RM, Soares EA, Lanzillotti HS. Assessment of nutrients intake of children in a charity daycare center: application of dietary reference intake. Rev Bras Saude Mater Infant. 2007;7:159-66.; Barbosa RM, Soares EA, Lanzillotti HS. Assessment of nutrients intake of children in a charity daycare center: application of dietary reference intake. Rev Bras Saude Mater Infant. 2007;7:159–166. [Google Scholar]
- 19.Bueno MB, Fisberg RM, Maximino P, Rodrigues GP, Fisberg M. Nutritional risk among Brazilian children 2 to 6 years old: a multicenter study. Nutrition. 2013;29:405-10. [DOI] [PubMed]; Bueno MB, Fisberg RM, Maximino P, Rodrigues GP, Fisberg M. Nutritional risk among Brazilian children 2 to 6 years old: a multicenter study. Nutrition. 2013;29:405–410. doi: 10.1016/j.nut.2012.06.012. [DOI] [PubMed] [Google Scholar]
- 20.Menezes RC, Osório MM. Energy and protein intake and nutritional status of children under five years of age in Pernambuco state, Brazil. Rev Nutr. 2007;20:337-47.; Menezes RC, Osório MM. Energy and protein intake and nutritional status of children under five years of age in Pernambuco state, Brazil. Rev Nutr. 2007;20:337–347. [Google Scholar]
- 21.Alves G, Colauto EV, Fernandes JK, Zabine L, Nienow RC. Anthropometric and food intake assessment of preschoolers in day-care centers in Umuarama, Paraná. Arq Cienc Saude Unipar. 2008;12:119-26.; Alves G, Colauto EV, Fernandes JK, Zabine L, Nienow RC. Anthropometric and food intake assessment of preschoolers in day-care centers in Umuarama, Paraná. Arq Cienc Saude Unipar. 2008;12:119–126. [Google Scholar]
- 22.Caetano MC, Ortiz TT, Silva SG, Souza FI, Sarni RO. Complementary feeding: inappropriate practices in infants. J Pediatr (Rio J). 2010;86:196-201. [DOI] [PubMed]; Caetano MC, Ortiz TT, Silva SG, Souza FI, Sarni RO. Complementary feeding: inappropriate practices in infants. J Pediatr (Rio J) 2010;86:196–201. doi: 10.2223/JPED.1994. [DOI] [PubMed] [Google Scholar]
- 23.Martino HS, Ferreira AC, Pereira CN, Silva RR. Anthropometric evaluation and food intake of preschool children at municipal educational centers, in South of Minas Gerais State, Brazil. Cienc Saude Colet. 2010;15:551-8. [DOI] [PubMed]; Martino HS, Ferreira AC, Pereira CN, Silva RR. Anthropometric evaluation and food intake of preschool children at municipal educational centers, in South of Minas Gerais State, Brazil. Cienc Saude Colet. 2010;15:551–558. doi: 10.1590/S1413-81232010000200031. [DOI] [PubMed] [Google Scholar]
- 24.Silva JV, Timóteo AK, Santos CD, Fontes G, Rocha EM. Food consumption of children and adolescents living in an area of invasion in Maceio, Alagoas, Brazil. Rev Bras Epidemiol. 2010;13:83-93. [DOI] [PubMed]; Silva JV, Timóteo AK, Santos CD, Fontes G, Rocha EM. Food consumption of children and adolescents living in an area of invasion in Maceio, Alagoas, Brazil. Rev Bras Epidemiol. 2010;13:83–93. doi: 10.1590/s1415-790x2010000100008. [DOI] [PubMed] [Google Scholar]
- 25.Paiva-Bandeira GT, Rios-Asciutti LS, Riveira AA, RodriguesGonçalves C, Pordeus-de-Lima RC, Marinho-Albuquerque T, et al. The relationship between income and children's habitual consumption of ß-carotene, vitamin C and vitamin E in food. Rev Salud Publica. 2011;13:386-97. [PubMed]; Paiva-Bandeira GT, Rios-Asciutti LS, Riveira AA, RodriguesGonçalves C, Pordeus-de-Lima RC, Marinho-Albuquerque T. The relationship between income and children's habitual consumption of ß-carotene, vitamin C and vitamin E in food. Rev Salud Publica. 2011;13:386–397. [PubMed] [Google Scholar]
- 26.Leão AL, Santos LC. Micronutrient consumption and overweight: is there a relationship. Rev Bras Epidemiol. 2012;15:85-95. [DOI] [PubMed]; Leão AL, Santos LC. Micronutrient consumption and overweight: is there a relationship. Rev Bras Epidemiol. 2012;15:85–95. doi: 10.1590/s1415-790x2012000100008. [DOI] [PubMed] [Google Scholar]
- 27.Bortolini GA, Vitolo MR. The impact of systematic dietary counseling during the first year of life on prevalence rates of anemia and iron deficiency at 12-16 months. J Pediatr (Rio J). 2012;88:33-9. [DOI] [PubMed]; Bortolini GA, Vitolo MR. The impact of systematic dietary counseling during the first year of life on prevalence rates of anemia and iron deficiency at 12-16 months. J Pediatr (Rio J) 2012;88:33–39. doi: 10.2223/JPED.2156. [DOI] [PubMed] [Google Scholar]
- 28.Braga JA, Vitalle MS. Iron deficiency in infants and children. Rev Bras Hematol Hemoter. 2010;32 Suppl 2:38-44.; Braga JA, Vitalle MS. Iron deficiency in infants and children. Rev Bras Hematol Hemoter. 2010;32(2):38–44. [Google Scholar]
- 29.Carrascoza KC, Possobon RF, Ambrosano GM, Costa Júnior AL, Moraes AB. Determinants of the exclusive breastfeeding abandonment in children assisted by interdisciplinary program on breast feeding promotion. Cien Saude Colet. 2011;16:4139-46. [DOI] [PubMed]; Carrascoza KC, Possobon RF, Ambrosano GM, Costa AL, Júnior, Moraes AB. Determinants of the exclusive breastfeeding abandonment in children assisted by interdisciplinary program on breast feeding promotion. Cien Saude Colet. 2011;16:4139–4146. doi: 10.1590/s1413-81232011001100019. [DOI] [PubMed] [Google Scholar]
- 30.Kaufmann CC, Albernaz EP, Silveira RB, Silva MB, Mascarenhas ML. Feeding during the first three months of life for infants of a cohort in Pelotas, Rio Grande do Sul, Brazil. Rev Paul Pediatr. 2012;30:157-65.; Kaufmann CC, Albernaz EP, Silveira RB, Silva MB, Mascarenhas ML. Feeding during the first three months of life for infants of a cohort in Pelotas, Rio Grande do Sul, Brazil. Rev Paul Pediatr. 2012;30:157–165. [Google Scholar]
- 31.Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Careˆncias de micronutrientes. Cadernos de Atenção Básica. 20. Brasília. Ministério da Saúde. 2007. Disponível em: http://189.28.128.100/nutricao/docs/geral/abcad20.pdf; Brasil.Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica . Careˆncias de micronutrientes. Cadernos de Atenção Básica. 20. Brasília: Ministério da Saúde; 2007. http://189.28.128.100/nutricao/docs/geral/abcad20.pdf [Google Scholar]
- 32.Castro TG, Silva-Nunes M, Conde WL, Muniz PT, Cardoso MA. Anemia and iron deficiency among schoolchildren in the Western Brazilian Amazon: prevalence and associated factors. Cad Saude Publica. 2011;27:131-42. [DOI] [PubMed]; Castro TG, Silva-Nunes M, Conde WL, Muniz PT, Cardoso MA. Anemia and iron deficiency among schoolchildren in the Western Brazilian Amazon: prevalence and associated factors. Cad Saude Publica. 2011;27:131–142. doi: 10.1590/s0102-311x2011000100014. [DOI] [PubMed] [Google Scholar]
- 33.Bortolini GA, Vitolo MR. Low compliance with supplementary iron to infants attending public health services. Pediatria (São Paulo). 2007;29:176-82.; Bortolini GA, Vitolo MR. Low compliance with supplementary iron to infants attending public health services. Pediatria (São Paulo) 2007;29:176–182. [Google Scholar]
- 34.Cruz JB, Soares HF. Uma revisão sobre o zinco. Ensaios e C. 2011;15:207-22.; Cruz JB, Soares HF. Uma revisão sobre o zinco. Ensaios e C. 2011;15:207–222. [Google Scholar]
- 35.Longo-Silva G, Toloni MH, Goulart RM, Taddei JA. Evaluation of food consumption at public day care centers in São Paulo, Brazil. Rev Paul Pediatr. 2012;30:35-41.; Longo-Silva G, Toloni MH, Goulart RM, Taddei JA. Evaluation of food consumption at public day care centers in São Paulo, Brazil. Rev Paul Pediatr. 2012;30:35–41. [Google Scholar]
- 36.Villar BS, Schwartzman F, Januario BL, Ramos JF. Situation of the municipalities of São Paulo state in relation to the purchase of products directly from family farms for the National School Feeding Program (PNAE). Rev Bras Epidemiol. 2013;16:223-6. [PubMed]; Villar BS, Schwartzman F, Januario BL, Ramos JF. Situation of the municipalities of São Paulo state in relation to the purchase of products directly from family farms for the National School Feeding Program (PNAE) Rev Bras Epidemiol. 2013;16:223–226. [PubMed] [Google Scholar]
- 37.Brasil. Ministério da Educação. Fundação Nacional de Desenvolvimento da Educação. Coordenação Geral do Programa Nacional de Alimentação Escolar. Manual de orientação para a alimentação escolar na educação infantil, ensino fundamental, ensino médio e na educação de jovens e adultos. 2a ed. Brasília: Ministério da Saúde; 2012. Disponível em: http://www.fnde.gov.br/arquivos/category/110-alimentacao-e-nutricao?download=7669:manual-de-orientacao-sobre-alimentacao-escolar-nas-diferentes-etapas-de-ensino; Brasil.Ministério da Educação. Fundação Nacional de Desenvolvimento da Educação. Coordenação Geral do Programa Nacional de Alimentação Escolar . Manual de orientação para a alimentação escolar na educação infantil, ensino fundamental, ensino médio e na educação de jovens e adultos. 2a ed. Brasília: Ministério da Saúde; 2012. http://www.fnde.gov.br/arquivos/category/110-alimentacao-e-nutricao?download=7669:manual-de-orientacao-sobre-alimentacao-escolar-nas-diferentes-etapas-de-ensino [Google Scholar]
- 38.Fisberg RM, Slater B, Marchioni DM, Martini LA. Inquéritos alimentares: métodos e bases científicos. São Paulo: Manole; 2005.; Fisberg RM, Slater B, Marchioni DM, Martini LA. Inquéritos alimentares: métodos e bases científicos. São Paulo: Manole; 2005. [Google Scholar]
- 39.Verly Junior E, Cesar CL, Fisberg RM, Marchioni DM. Within-person variance of the energy and nutrient intake in adolescents: data adjustment in epidemiological studies. Rev Bras Epidemiol. 2013;16:170-7. [PubMed]; Verly E, Junior, Cesar CL, Fisberg RM, Marchioni DM. Within-person variance of the energy and nutrient intake in adolescents: data adjustment in epidemiological studies. Rev Bras Epidemiol. 2013;16:170–177. [PubMed] [Google Scholar]
- 40.Falcão-Gomes RC, Coelho AA, Schmitz BA. Characterization of dietary intake assessment studies in pre-school children. Rev Nutr. 2006;19:713-27.; Falcão-Gomes RC, Coelho AA, Schmitz BA. Characterization of dietary intake assessment studies in pre-school children. Rev Nutr. 2006;19:713–727. [Google Scholar]
- 41.Verly-Jr E, Castro MA, Fisberg RM, Marchioni DM. Precision of usual food intake estimates according to the percentage of individuals with a second dietary measurement. J Acad Nutr Diet. 2012;112:1015-20. [DOI] [PubMed]; Verly-Jr E, Castro MA, Fisberg RM, Marchioni DM. Precision of usual food intake estimates according to the percentage of individuals with a second dietary measurement. J Acad Nutr Diet. 2012;112:1015–1020. doi: 10.1016/j.jand.2012.03.028. [DOI] [PubMed] [Google Scholar]
- 42.Marchioni DM, Verly Junior E, Cesar CL, Fisberg RM. Assessment of nutrient intake adequacy in clinical practice. Rev Nutr. 2011;24:825-32.; Marchioni DM, Verly E, Junior, Cesar CL, Fisberg RM. Assessment of nutrient intake adequacy in clinical practice. Rev Nutr. 2011;24:825–832. [Google Scholar]
- 43.Castro MA, Verly-Jr E, Fisberg M, Fisberg RM. Children's nutrient intake variability is affected by age and body weight status according to results from a Brazilian multicenter study. Rev Nutr. 2014;34:74-84. [DOI] [PubMed]; Castro MA, Verly-Jr E, Fisberg M, Fisberg RM. Children's nutrient intake variability is affected by age and body weight status according to results from a Brazilian multicenter study. Rev Nutr. 2014;34:74–84. doi: 10.1016/j.nutres.2013.09.006. [DOI] [PubMed] [Google Scholar]
- 44.National Research Council. Dietary reference intakes: applications in dietary assessment. Washington: The National Academy Press; 2000.; National Research Council . Dietary reference intakes: applications in dietary assessment. Washington: The National Academy Press; 2000. [Google Scholar]
- 45.Slater B, Marchioni DL, Fisberg RM. Estimating prevalence of inadequate nutritent intake. Rev Saude Publica. 2004;38:599-605. [DOI] [PubMed]; Slater B, Marchioni DL, Fisberg RM. Estimating prevalence of inadequate nutritent intake. Rev Saude Publica. 2004;38:599–605. doi: 10.1590/s0034-89102004000400019. [DOI] [PubMed] [Google Scholar]
- 46.Dodd KW, Guenther PM, Freedman LS, Subar AF, Kipnis V, Midthune D, et al. Statistical methods for estimating usual intake of nutrients and foods: a review of the theory. J Am Diet Assoc. 2006;106:1640-50. [DOI] [PubMed]; Dodd KW, Guenther PM, Freedman LS, Subar AF, Kipnis V, Midthune D. Statistical methods for estimating usual intake of nutrients and foods: a review of the theory. J Am Diet Assoc. 2006;106:1640–1650. doi: 10.1016/j.jada.2006.07.011. [DOI] [PubMed] [Google Scholar]
- 47.Tooze JA, Kipnis V, Buckman DW, Carroll RJ, Freedman LS, Guenther PM, et al. A mixedeffects model approach for estimating the distribution of usual intake of nutrients: the NCI method. Stat Med. 2010;30:2857-68. [DOI] [PMC free article] [PubMed]; Tooze JA, Kipnis V, Buckman DW, Carroll RJ, Freedman LS, Guenther PM. A mixedeffects model approach for estimating the distribution of usual intake of nutrients: the NCI method. Stat Med. 2010;30:2857–2868. doi: 10.1002/sim.4063. [DOI] [PMC free article] [PubMed] [Google Scholar]