

Abstract
Idiopathic demyelinating optic neuritis (ON) most commonly presents as acute unilateral vision loss and eye pain and is frequently associated with multiple sclerosis. Although emphasis is often placed on the good recovery of high-contrast visual acuity, persistent deficits are frequently observed in other aspects of vision, including contrast sensitivity, visual field testing, color vision, motion perception, and vision-related quality of life. Persistent and profound structural and functional changes are often revealed by imaging and electrophysiologic techniques, including optical coherence tomography, visual-evoked potentials, and nonconventional MRI. These abnormalities can impair patients' abilities to perform daily activities (e.g., driving, working) so they have important implications for patients' quality of life. In this article, we review the sequelae from ON, including clinical, structural, and functional changes and their interrelationships. The unmet needs in each of these areas are considered and the progress made toward meeting those needs is examined. Finally, we provide an overview of past and present investigational approaches for disease modification in ON.
Although idiopathic demyelinating optic neuritis (ON) broadly describes the vision loss associated with any inflammation of the CNS white matter tract referred to as the optic nerve, the term is most commonly associated with the unilateral visual loss that occurs in multiple sclerosis (MS). Atypical ON may be associated with neuromyelitis optica, infections, or systemic etiologies, but this article will focus predominantly on the typical demyelinating ON syndrome associated with MS. Typical ON is characterized by a loss of vision that develops over days and is associated with dyschromatopsia, visual field loss, and pain that is often exacerbated by eye movements.1 Usually there are no retinal exudates or severe disc swelling and vision is better than no light perception.
Significant knowledge about the clinical course of ON derives from the Optic Neuritis Treatment Trial (ONTT). First published in 1992, the ONTT established that high-dose IV corticosteroid treatment slightly accelerated the rate of recovery but had no effect on long-term visual outcomes.2 Visual fields and contrast sensitivity were the primary measures of efficacy and showed a slight advantage of high-dose IV corticosteroids over placebo at 6 months. Nevertheless, vision for most patients in all treatment groups at 6 months was characterized as “normal” based on high-contrast visual acuity, a secondary outcome measured using Snellen charts, which was 20/50 or better for >90% of patients regardless of treatment assignment. This created the impression that most patients make an excellent recovery following acute ON. However, a follow-up study 5–8 years later found abnormalities in affected eyes vs fellow eyes for the primary endpoints of contrast sensitivity (58% vs 17%) and visual field (33% vs 12%), as well as the secondary endpoints of high-contrast visual acuity (39% vs 16%) and color vision (37% vs 18%).3 Furthermore, as described in the sections that follow, advances in imaging and electrophysiologic techniques over the past 2 decades have revealed that persistent structural and functional damage is detectable following episodes of acute ON and that the associated visual deficits may have considerable impact on quality of life (QOL) measures. Given the development of therapies with the potential to prevent neuroaxonal loss and facilitate remyelination following acute ON, it is time to reassess the extent of spontaneous recovery in ON and the approaches to determining outcomes so that unmet needs may be identified and addressed.
In this article, we review the evidence for persistent functional and structural abnormalities in ON and their impact on visual function and vision-related QOL. We also provide an overview of investigational approaches to treat the underlying pathology in ON.
CLINICAL COURSE AND ASSESSMENT OF VISUAL FUNCTION
Typical ON develops over a 7- to 10-day period and begins to resolve within 2–3 weeks.4,5 Initial rapid improvement in visual function within the first month begins to slow in an asymptotic fashion over succeeding months,4 and improvements have been observed up to 2 years later.6 Numerous studies have found evidence of persistent retinal thinning, optic nerve atrophy, and reduced amplitude and increased latency of visual-evoked potentials (VEPs), consistent with chronic demyelination and neuroaxonal loss as sequelae of acute ON (see next sections). The extent of latency recovery appears to be more complete in younger patients vs older patients, females vs males, and patients with less severe attacks vs more severe attacks.7 Moreover, recovery of different aspects of visual function may proceed at different rates, with different sensitivities among tests, and to a different extent (figure 1). Recovery of different aspects of visual function may also involve distinct mechanisms, as patients who achieve partial recovery of static visual functions (e.g., high- and low-contrast visual acuity) after 1 month may recover those functions completely, whereas dynamic visual function (motion perception) appears to recover at a slower constant rate irrespective of the severity of the initial deficit.8
Figure 1. Evolution of visual function after acute optic neuritis.
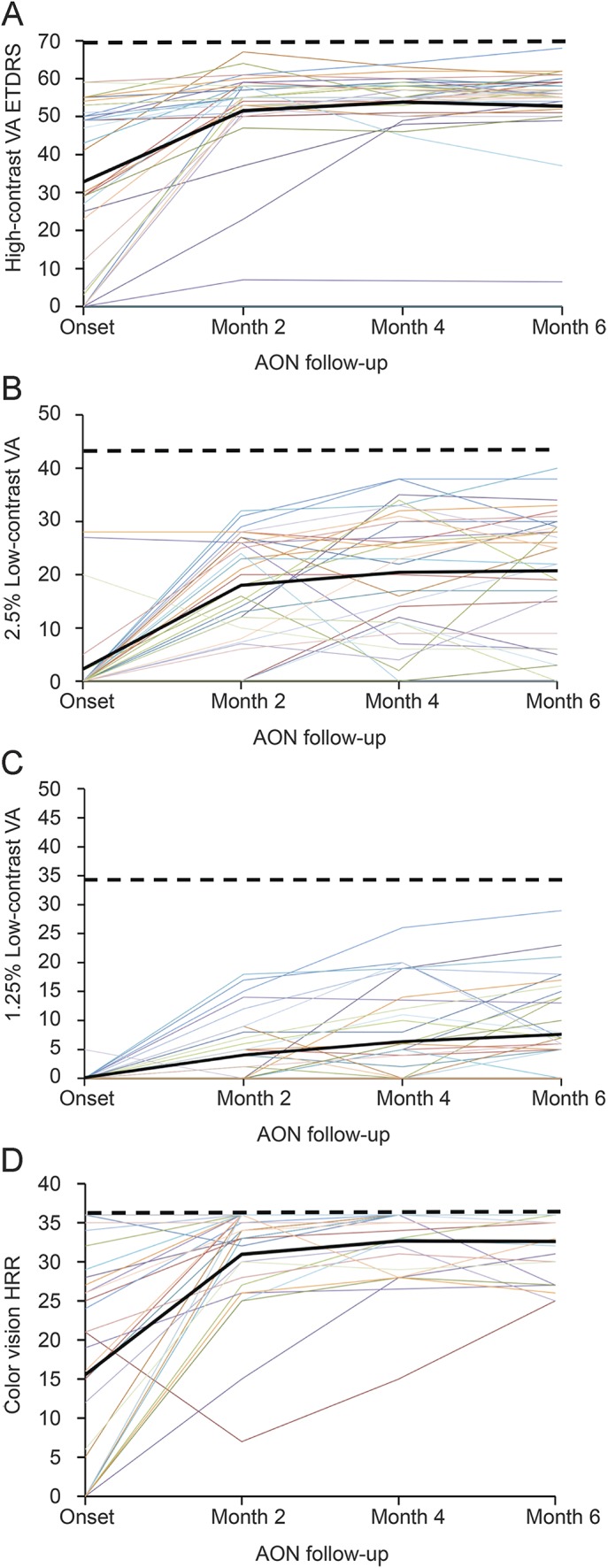
Figure shows the measurement of high-contrast visual acuity (VA) using the Early Treatment Diabetic Retinopathy Study (ETDRS) charts (A), the 2.5% and 1.25% low-contrast VA using Sloan charts (B, C), and color vision using the Hardy-Rand-Rittler (HRR) pseudoisochromatic plates (D) in a cohort of 37 patients with acute optic neuritis (AON) and visual assessment at baseline (presentation) and months 2, 4, and 6 after onset (data from Gabilondo, I et al. 201516). Each colored line is data from an individual patient, the solid black line represents the mean from all patients, and the dashed black line shows the normal values for healthy individuals for binocular testing (ETDRS = 70; 2.5% low-contrast VA = 43; 1.25% low-contrast VA = 34; HRR = 36). Reprinted with permission from Elena H. Martinez-Lapiscina.
Although patients with ON frequently regain visual acuity to a large extent as measured by full-contrast letter charts (e.g., Snellen charts), low-contrast acuity/sensitivity reveals permanent deficits and is a better predictor of impairment for daily activities that require vision, such as reading, facial recognition, and driving.9 Persistent deficits in low-contrast letter acuity characteristic of ON are better measured using Sloan charts (Sloan low-contrast letter acuity [SLCLA]) that include versions with 2.5% and 1.25% contrast levels to better stratify deficits. The pattern of visual field defects may help distinguish ON from other neuropathies. In ON, a central scotoma is common and Humphrey central visual field perimetry frequently shows diffuse loss, whereas peripheral, altitudinal, or other defects may occasionally be evident on formal perimetry. Color vision is commonly affected in ON, but there is no consistent pattern of dyschromatopsia.10 More complex visual functions, such as motion perception, are also frequently affected by ON.11 Binocular summation (improved vision with binocular viewing) has also been shown to be reduced, and in some instances patients demonstrate binocular inhibition (worse vision with binocular viewing), perhaps reflecting concomitant disease activity in postgeniculate pathways in some patients.12 Thus, evaluation of visual function after ON requires multiple tests to ensure comprehensive assessment of the potential deficits.
APPROACHES TO ASSESSMENT OF ON
Optical coherence tomography.
Assessment of structural changes in the course of ON has been revolutionized over the past 2 decades by advances in optical coherence tomography (OCT), a technique that uses interferometry of reflected light to obtain images of the retinal layers13 (figure 2). Most OCT studies of patients with ON have used time-domain OCT (TD-OCT), which provides cross-sectional images from different tissue levels. Since the peripapillary retinal nerve fiber layer (RNFL) is composed of unmyelinated optic nerve axons, RNFL thinning detected by OCT is directly interpretable as neuroaxonal degeneration. More modern systems using spectral-domain OCT (SD-OCT) provide considerably improved resolution and speed and can be used to generate 3-dimensional images for measurements of thickness of neuronal layers.
Figure 2. Optical coherence tomography of the human retina.

A) Detailed retinal segmentation sample on spectral-domain optical coherence tomography (OCT) image. Six intraretinal layer borders can be automatically segmented. (B) Correlation of anatomy with OCT for the human retina. On the left is a hematoxylin & eosin stain of the human retina, in the center is a schematic representation of the cell composition of the human retina, and on the right is a magnification of the image obtained with spectral-domain OCT (bottom), with indications of the retina layers identified. Figure 2B reprinted with permission from Santiago Ortiz-Perez. BM = Bruch membrane; CC = choriocapillaris layer; GCL = ganglion cell layer; ILM = inner limiting membrane; INL = inner nuclear layer; IPL = inner plexiform layer; OLM = outer limiting membrane; ONL = outer nuclear layer; OPL = outer plexiform layer; PL = photoreceptor layer; RNFL = retinal nerve fiber layer; RPE = retinal pigment epithelium.
Acute ON often results in inflammatory swelling of the RNFL of the affected eye. The inflammatory swelling generally resolves within 3 months14 and is accompanied by a period of RNFL thinning that continues for up to 7–12 months but is most prominent in the first 6 months after acute ON onset.5,15 The initial period of swelling prevents examination of the timing of axonal loss in the RNFL with TD-OCT. In contrast, the thickness of the retinal ganglion cell layer (RGCL) appears to be less affected by edema,16,17 so the more detailed resolution with SD-OCT may allow for a better assessment of the timing of thinning in reference to acute ON. Recent studies suggest that thinning of the RGCL starts within several weeks after an episode of ON and may precede RNFL thinning.16,17 Ultimately, RNFL thinning in affected eyes correlates with visual acuity, low-contrast letter acuity, visual field, color vision, and VEPs (see also below),18,19 thereby supporting its functional relevance, and RNFL thickness <75 μm has been shown to predict reduced visual field function.5,20 Although it is not yet clear whether preventing RNFL thickness from crossing that threshold can reduce the extent of associated visual deficits, it is worth noting that it is also near the lower limit of RNFL thickness, when virtually all retinal ganglion cell (RGC) axons have been lost (20–40 μm).21
Thinning of the RNFL following an episode of ON is thought to result from axonal loss subsequent to axonal injury during the inflammatory demyelinating lesion of the affected optic nerve. However, it is noteworthy that detectable RNFL thinning and associated visual deficits are also observed in unaffected eyes of patients with MS in the absence of history of ON.15 One possibility is that some “mild” attacks are not reported or do not result in deficits that are immediately evident to patients. Thus, in nonacute ON eyes there is a component of RNFL thinning that may be attributable to other causes, such as subclinical optic nerve inflammation, neurodegeneration within normal-appearing white matter, or transsynaptic degeneration associated with lesions elsewhere in the visual pathway.22–24
The increased resolution of SD-OCT and the use of segmentation algorithms have allowed a more detailed analysis of the effects of ON and MS on retinal structure25 (figure 2). These studies found that RNFL thinning associated with MS with or without ON is not confined to the peripapillary region but also affects the macula. In addition, a similar pattern of thinning is observed for the ganglion cell layer/inner plexiform layers (GCL + IPL) in the peripapillary region and macula. A recent study in patients with ON found that decreases of ≥4.5 μm in GCL + IPL thickness after 1 month predicted low-contrast visual acuity dysfunction at 6 months, whereas decreases of ≥7 μm predicted visual field and color vision deficits.16 In another study in patients with MS with or without a history of ON, thinning of GCL + IPL was most closely associated with visual function and vision-specific QOL.26 Results of these studies suggest that degeneration associated with ON and MS is widespread in the RGCL.
Together, these studies provide compelling evidence for structural damage from acute ON, and they also provide a powerful demonstration of the potential for SD-OCT as a tool to assess neurodegenerative changes in acute ON. However, both TD-OCT and SD-OCT appear to be less sensitive than VEPs for assessing the clinical and subclinical effects of ON,27,28 so interpretation of OCT may require complementary assessments using functional techniques. Furthermore, improvements are needed to standardize and reduce test-retest variability in SD-OCT systems.29 Given the rapid evolution of the technology, the technical expertise required, and differences between commercially available instruments,30 it is also important that criteria be established to ensure quality control for OCT as a validated outcome measure, a process that is under way.31
VEPs.
Standard VEPs elicited by visual stimuli and measured in the occipital cortex can be used to detect functional changes in the visual pathway, including the optic nerve.32 In multifocal VEPs (mfVEPs), visual stimuli are provided independently to localized regions of a wider visual field (48°) and responses to the stimuli are measured individually,33 allowing for a more detailed analysis of visual function covering a much larger area of the visual pathway than standard VEPs (figure 3).
Figure 3. Multifocal visual-evoked potentials in optic neuritis.

Figure shows the visual-evoked potentials (VEPs) in 52 sectors of the retina. (A, B) A case of acute optic neuritis with diffuse impairment of the VEPs in the affected eye (A) compared with the unaffected eye (B), with significant impairment of the latencies and amplitudes. (B, C) After recovery from the acute optic neuritis, the VEPs show a significant decrease of amplitude and latencies in most of the sectors of the affected eye (C) compared with the unaffected eye (D). Reprinted with permission from Ana Tercero.
The severity of an attack of ON and the extent of inflammation are correlated with an acute reduction in the amplitude of VEPs.34 Reduction in VEP amplitude is thought to reflect functional impairment of axonal conduction either transiently (e.g., due to acute inflammation or demyelination) or persistently (due to axonal loss). Within 3–4 months after the acute episode, the amplitude generally shows some recovery, reflecting resolution of edema, and the waveform of the VEP is well-preserved, but the latency is significantly increased. This residual latency delay is thought to result from demyelination of surviving axons, which interferes with saltatory conduction of the action potential along the optic nerve lesion. Some investigators have reported subsequent improvement in latency for up to 2 years,6 whereas others have reported no further recovery after 4 months.8 Prolongation of latency is most evident in the central visual field, perhaps indicating that the central (macular) region of the optic nerve is more susceptible to demyelination or resistant to remyelination.32 The central region of the optic nerve contains the greatest density of parvocellular fibers that convey static information (e.g., form and color), but VEP latency in patients with ON correlates more strongly with dynamic functions (e.g., motion detection) than with static functions. This may suggest more specific effects on magnocellular fibers or greater vulnerability of fibers required for accurate signal timing.8
Effects of ON on VEPs have also been shown to reflect structural changes in the RNFL. In a study of 21 patients following a first episode of unilateral ON, VEP latency prolongations and amplitude reductions of affected eyes at baseline and 3 months after onset were associated with RNFL thinning,19 suggesting a relationship between the initial structural loss and residual functional impairment. In a separate study of 25 patients with ON with incomplete recovery after 1 year, similar relationships between VEP latency/amplitude and RNFL thinning were still evident,18 further supporting the clinical relevance of this technique.
mfVEPs have been used in a growing number of small studies to examine the pathology of ON in greater detail.35–38 mfVEPs detect functional changes associated with onset and evolution of acute ON38 and may be particularly useful to assess treatment outcomes in clinical trials as it appears to be more reproducible than standard VEPs.39 One study of 25 patients with ON between 6 and 12 months after onset found an apparent discrepancy between structural and functional measures in these patients.35 As RNFL thinning progressed in the affected eyes over this time period, the mfVEP amplitude partially recovered, suggesting that functional recovery may be due in part to remyelination and/or neuronal plasticity.
Functional data provided by VEPs and mfVEPs make an ideal counterpart to structural retinal assessments using OCT. However, as with OCT, criteria need to be established to ensure reproducibility and validity of VEP results. Furthermore, larger-scale studies are needed to confirm the results of current smaller studies.
MRI.
Nonconventional MRI techniques offer novel tools to examine the structure of CNS tissues in detail. For example, magnetization transfer (MT) imaging exploits the difference in resonance in free protons and protons associated with macromolecules (e.g., myelin), the ratio of which may provide a measure of myelin content.40 Diffusion tensor imaging (DTI) can be used to measure asymmetric radial diffusivity (RD), axial diffusivity (AD), or fractional anisotropy (FA) of water as a gauge of tissue in major nerve tracts (e.g., optic nerve and optic radiations).41
A small number of studies have provided support for use of these techniques to assess pathologic changes in ON. For example, in an MT study in 11 patients with ON, MT ratios of affected optic nerves closely followed the course of the disease: they were significantly higher at baseline (within 8 days of onset) but were reduced at months 3 and 6.42 In a separate study in 37 patients with ON, MT ratios of affected optic nerves were not found to be different from those of unaffected nerves until 3 months after onset.43 In that study, ON-associated alterations in MT ratios at 3 months correlated with high- and low-contrast visual deficits and with VEP latency at 6 months as well as with RNFL thinning at 12 months.
In a study of DTI performed within 30 days of onset and after 1 year in 12 patients with ON, FA of affected optic nerves (which is also considered a potential measure of myelination) was the only parameter correlated with vision at onset but did not correlate with the extent of recovery of visual acuity or contrast sensitivity at 1 or 3 months.44 The AD (considered a measure of axonal integrity) was the only parameter that was correlated with worse contrast sensitivity at 1 and 3 months. This was confirmed in a follow-up study in 25 patients, in which a lower baseline AD was also found to be correlated with the extent of RNFL thinning and with VEP amplitude and latency.45 These were small studies and should be interpreted with caution as eye motion makes imaging of the optic nerve by MT ratio and DTI challenging, but they do not seem to support a model in which the extent of neurodegeneration is determined solely by chronic demyelination. Rather, they suggest that the initial neuroaxonal effects of the acute inflammatory injury may be more important.
Although these “nonconventional” MRI techniques hold promise as a tool to investigate underlying processes and assess recovery in ON, there are substantial challenges to widespread use. For example, the acquisition times are frequently longer than is practical for routine human studies, and imaging is complicated by motion artifacts caused by moving the eye or head.46 In addition, there is no consensus on sequences and protocols for their application in ON. These factors have limited widespread adoption of these approaches and have likely contributed to the inconsistencies in findings. Thus, further technological improvements and standardization of techniques for imaging of ON lesions will be required before they can be considered as reliable measures of outcomes in clinical trials.
QOL
Visual deficits in patients with ON are likely to have a marked impact on daily activities and QOL. Patients frequently rate vision among the most important physical functions affected by MS.47 However, vision is poorly or insufficiently represented on standard objective measures of physical function, such as the Expanded Disability Status Scale, and functional assessment instruments, such as the Multiple Sclerosis Functional Composite (MSFC). Addition of SLCLA charts to the MSFC has been reported to better capture MS-related disability.48 One patient-reported outcome instrument, the 25-item National Eye Institute Visual Functioning Questionnaire (NEI-VFQ-25), has become a commonly used measurement of vision-specific health-related QOL. When administered to patients from the ONTT 5–8 years after the episode of acute ON, scores on the NEI-VFQ-25 were lower than for an older disease-free cohort.3 In patients with MS, correlations with NEI-VFQ-25 scores have been demonstrated for low-contrast visual acuity,49 binocular summation,12 motion perception,50 and loss of RGCs25 (figure 4). Moreover, a 10-item supplement has been developed to better capture aspects more relevant to neuro-ophthalmology, such as double vision and difficulties with viewing motion.51 A follow-up study has also reported its ability to distinguish patients with MS with a history of ON.52
Figure 4. Relationship of thickness of retinal layers to quality of life and low-contrast visual acuity.
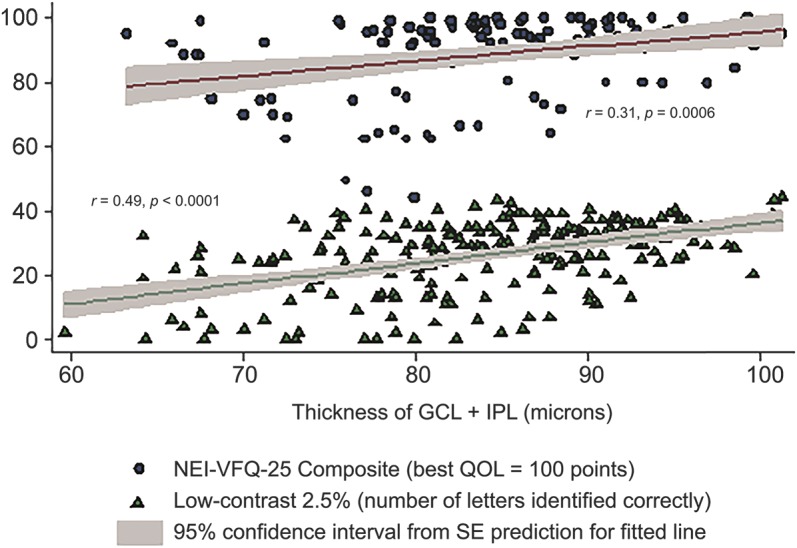
Scatter plot and fitted linear regression line showing relationships of ganglion cell layer plus inner plexiform layer (GCL + IPL) thickness to 25-item National Eye Institute Visual Functioning Questionnaire (NEI-VFQ-25) composite scores and low-contrast visual acuity at 2.5% level. The regression lines represent fitted values for mean GCL + IPL thickness for each value of NEI-VFQ-25 or low-contrast visual acuity; the gray shaded areas show the 95% confidence intervals from the SEs of the predictions for the fitted lines. Linear correlations were significant. QOL = quality of life. Reprinted from Ophthalmology 119(6), Walter SD et al., Ganglion cell loss in relation to visual disability in multiple sclerosis, 1250–1257, 2012, with permission from Elsevier.26
TREATMENTS
An important unmet need with respect to ON is the availability of effective treatments to prevent or reverse long-term visual dysfunction. Given the narrow window of time during which most recovery occurs, it seems reasonable to suggest that an effective treatment be initiated as soon as possible after ON onset, with the aim of promoting RGC survival and either extending the window for remyelination or accelerating the rate and extent to which it occurs. Data emerging from OCT studies suggest that RGC loss may begin within weeks of the event, thereby narrowing the time to initiate neuroprotective therapy.
Despite the lack of long-term benefits of high-dose corticosteroids, patients with acute ON are frequently provided these drugs as symptomatic treatment to speed resolution of acute inflammation. Patients are often assessed by MRI to determine their risk for MS, but it is not clear that disease-modifying therapies for relapsing forms of MS are effective to prevent neurodegeneration when ON occurs while receiving these treatments. For example, interferon β was not found to prevent RFNL thinning in patients with ON.53 Natalizumab has been shown to reduce loss of vision54 and improve VEPs55 in patients with relapsing-remitting MS, but there are no data to indicate treatment benefits specifically in patients with ON. A phase II study of fingolimod in acute demyelinating ON is complete, although it is not clear that enrollment goals were met. Another phase II/III study is under way but study results are not yet available (table).
Table.
Phase II and III studies in typical optic neuritis

Based on promising results from animal studies and small clinical studies, IV immunoglobulin was investigated in patients with one or more episodes of typical ON and irreversible loss of visual acuity but was terminated early due to negative results56 (table). Since that time, various investigational therapies have shown promise in early preclinical and clinical studies, and a number of phase II and III studies have been completed or are under way. For example, in a placebo-controlled study of IV erythropoietin for 3 days as an add-on to methylprednisone in patients with a first episode of ON within the previous 10 days, those treated with erythropoietin demonstrated reduced RNFL thinning, less decrease in optic nerve diameter, and shorter VEP latency.57 Although the mechanism by which erythropoietin may exert these effects is poorly understood, it may involve the neuroprotective effects of this hormone during acute inflammation. In another placebo-controlled study in patients with symptom duration of <4 weeks and reduced contrast sensitivity, simvastatin (a hypercholesterolemia medication) narrowly missed significance on the primary efficacy outcome (contrast sensitivity), but improvements were noted for VEP latency and amplitude.58 However, imbalances in randomization and technical issues may have contributed to the observed effects.59 A study in ON testing possible neuroprotective effects of phenytoin, an anticonvulsant, has recently completed, and another study testing effects of amiloride hydrochlorothiazide, a diuretic, is currently underway. Nevertheless, it is an open question whether a neuroprotective agent can do more than delay degeneration of axons if they remain chronically demyelinated. Finally, BIIB033, a fully-human antibody to LINGO-1, an inhibitor of myelination and neuroaxonal growth, has shown promise in preclinical and early clinical testing,60 and a phase II study in ON was recently completed.
CONCLUSIONS
It is now clear that recovery from ON is frequently incomplete, which adversely affects the QOL of patients. In addition, there remain considerable gaps with respect to understanding, assessing, and treating this disease to prevent long-term deficits. Nevertheless, ongoing work holds promise for all of these areas. The application of newer technologies continues to provide new insight into the underlying disease processes and increased appreciation of the injury that occurs following ON. The development of these new tools may increase the ability to detect meaningful changes in vision with therapeutic intervention and study results suggest that timing is critical. Development of guidelines to ensure consistency in their application should also improve interpretation of findings and thereby improve the quality of assessments. Finally, several therapies have shown promise in preclinical and early clinical testing. Therefore, there is reason to be optimistic that strategies may soon be identified to improve the prognosis for patients with ON. Given the relationship between ON and MS, it seems likely that any such developments for ON may have substantial implications for understanding, assessing, and treating MS as well.
ACKNOWLEDGMENT
The authors thank Dr. Elena H. Martinez-Lapiscina, Dr. Santiago Ortiz-Perez, and Dr. Ana Tercero from the Center of Neuroimmunology, Institute of Biomedical Research August Pi Sunyer/Hospital Clinic Barcelona, University of Barcelona for creating figures 1, 2B, and 3, respectively. Lauren Nagy of Excel Scientific Solutions copyedited and styled the manuscript per journal requirements, and this editorial support was funded by Biogen.
GLOSSARY
- AD
axial diffusivity
- DTI
diffusion tensor imaging
- FA
fractional anisotropy
- GCL
ganglion cell layer
- IPL
inner plexiform layer
- mfVEP
multifocal VEP
- MS
multiple sclerosis
- MSFC
Multiple Sclerosis Functional Composite
- MT
magnetization transfer
- NEI-VFQ-25
25-item National Eye Institute Visual Functioning Questionnaire
- OCT
optical coherence tomography
- ON
optic neuritis
- ONTT
Optic Neuritis Treatment Trial
- QOL
quality of life
- RD
radial diffusivity
- RGC
retinal ganglion cell
- RGCL
retinal ganglion cell layer
- RNFL
retinal nerve fiber layer
- SD-OCT
spectral-domain OCT
- SLCLA
Sloan low-contrast letter acuity
- TD-OCT
time-domain OCT
- VEP
visual-evoked potential
AUTHOR CONTRIBUTIONS
All authors participated in the conception of the article, interpretation of the data, and revision of the manuscript, and they approved the final version. Biogen provided funding for writing and editorial support in the development of this paper, and they reviewed and provided feedback on the paper to the authors. The authors had full editorial control of the paper and provided their final approval of all content.
STUDY FUNDING
Writing and editorial support was funded by Biogen.
DISCLOSURE
S.L. Galetta has received consulting honoraria and travel funding/speaker honoraria from Genzyme and Biogen and is on the editorial board for Neurology and Journal of Neuro-Ophthalmology. P. Villoslada serves on advisory boards for Novartis, Roche, Neurotec Pharma, and Bionure Pharma; has consulted for Novartis, Roche, TFS, Heidelberg Engineering, MedImmune, Diagna Biotec, and Neurotec Pharma; is an academic editor for PLoSONE; is on the editorial board for Neurology & Therapy and Current Treatment Options in Neurology; has received research support from European Commission, Genzyme, Biogen, Instituto Salud Carlos III, Marato TV3, Novartis, and Roche; and holds patents and owns stocks/stock options with Bionure Pharma. N. Levin receives research support from National Multiple Sclerosis Foundation. K. Shindler received research support from the F.M. Kirby Foundation, Harbor Therapeutics, National Eye Institute, National Multiple Sclerosis Foundation, Research to Prevent Blindness, Sirtris Pharmaceuticals, ITMAT, and Stemnion, Inc.; has received speaker honoraria from Medical College of Wisconsin and Temple University; is an associate editor for Frontiers in Neurology: Neuro-Ophthalmology; receives publishing royalties from UpToDate and Oakstone Publishing; and has consulted for medical-legal cases. H. Ishikawa received research support from the NIH. E. Parr is a full-time employee of Excel Scientific Solutions, who were funded by Biogen to provide editorial and writing support for this paper. D. Cadavid is a full-time employee of Biogen, owns stock options in Biogen, and has patent applications pending related to the use of drugs that block LINGO-1 to treat demyelination in multiple sclerosis. L.J. Balcer received consulting fees from Acorda, Biogen, Genzyme, Novartis, Questcor, and Vaccinexe; serves on a clinical trial advisory board for Biogen; and serves on a scientific advisory board for Genzyme. Go to Neurology.org/nn for full disclosure forms.
REFERENCES
- 1.Toosy AT, Mason DF, Miller DH. Optic neuritis. Lancet Neurol 2014;13:83–99. [DOI] [PubMed] [Google Scholar]
- 2.Beck RW, Cleary PA, Anderson MM, Jr, et al. ; Optic Neuritis Study Group. A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. N Engl J Med 1992;326:581–588. [DOI] [PubMed] [Google Scholar]
- 3.Cole SR, Beck RW, Moke PS, Gal RL, Long DT; Optic Neuritis Study Group. The National Eye Institute Visual Function Questionnaire: experience of the ONTT. Invest Ophthalmol Vis Sci 2000;41:1017–1021. [PubMed] [Google Scholar]
- 4.Beck RW, Cleary PA, Backlund JC. The course of visual recovery after optic neuritis. Experience of the Optic Neuritis Treatment Trial. Ophthalmology 1994;101:1771–1778. [DOI] [PubMed] [Google Scholar]
- 5.Costello F, Hodge W, Pan YI, Eggenberger E, Coupland S, Kardon RH. Tracking retinal nerve fiber layer loss after optic neuritis: a prospective study using optical coherence tomography. Mult Scler 2008;14:893–905. [DOI] [PubMed] [Google Scholar]
- 6.Brusa A, Jones SJ, Plant GT. Long-term remyelination after optic neuritis: a 2-year visual evoked potential and psychophysical serial study. Brain 2001;124:468–479. [DOI] [PubMed] [Google Scholar]
- 7.Malik MT, Healy BC, Benson LA, et al. Factors associated with recovery from acute optic neuritis in patients with multiple sclerosis. Neurology 2014;82:2173–2179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Raz N, Dotan S, Chokron S, Ben-Hur T, Levin N. Demyelination affects temporal aspects of perception: an optic neuritis study. Ann Neurol 2012;71:531–538. [DOI] [PubMed] [Google Scholar]
- 9.Leat SJ, Legge GE, Bullimore MA. What is low vision? A re-evaluation of definitions. Optom Vis Sci 1999;76:198–211. [DOI] [PubMed] [Google Scholar]
- 10.Martínez-Lapiscina EH, Ortiz-Pérez S, Fraga-Pumar E, et al. Colour vision impairment is associated with disease severity in multiple sclerosis. Mult Scler 2014;20:1207–1216. [DOI] [PubMed] [Google Scholar]
- 11.Raz N, Dotan S, Benoliel T, Chokron S, Ben-Hur T, Levin N. Sustained motion perception deficit following optic neuritis: behavioral and cortical evidence. Neurology 2011;76:2103–2111. [DOI] [PubMed] [Google Scholar]
- 12.Pineles SL, Birch EE, Talman LS, et al. One eye or two: a comparison of binocular and monocular low-contrast acuity testing in multiple sclerosis. Am J Ophthalmol 2011;152:133–140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gabriele ML, Wollstein G, Ishikawa H, et al. Optical coherence tomography: history, current status, and laboratory work. Invest Ophthalmol Vis Sci 2011;52:2425–2436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Henderson AP, Altmann DR, Trip AS, et al. A serial study of retinal changes following optic neuritis with sample size estimates for acute neuroprotection trials. Brain 2010;133:2592–2602. [DOI] [PubMed] [Google Scholar]
- 15.Petzold A, de Boer JF, Schippling S, et al. Optical coherence tomography in multiple sclerosis: a systematic review and meta-analysis. Lancet Neurol 2010;9:921–932. [DOI] [PubMed] [Google Scholar]
- 16.Gabilondo I, Martínez-Lapiscina EH, Fraga-Pumar E, et al. Dynamics of retinal injury after acute optic neuritis. Ann Neurol 2015;77:517–528. [DOI] [PubMed] [Google Scholar]
- 17.Huang-Link Y-M, Al-Hawasi A, Lindehammar H. Acute optic neuritis: retinal ganglion cell loss precedes retinal nerve fiber thinning. Neurol Sci 2015;36:617–620. [DOI] [PubMed] [Google Scholar]
- 18.Trip SA, Schlottmann PG, Jones SJ, et al. Retinal nerve fiber layer axonal loss and visual dysfunction in optic neuritis. Ann Neurol 2005;58:383–391. [DOI] [PubMed] [Google Scholar]
- 19.Henderson AP, Altmann DR, Trip SA, et al. Early factors associated with axonal loss after optic neuritis. Ann Neurol 2011;70:955–963. [DOI] [PubMed] [Google Scholar]
- 20.Costello F, Coupland S, Hodge W, et al. Quantifying axonal loss after optic neuritis with optical coherence tomography. Ann Neurol 2006;59:963–969. [DOI] [PubMed] [Google Scholar]
- 21.Hood DC, Anderson SC, Wall M, Kardon RH. Structure versus function in glaucoma: an application of a linear model. Invest Ophthalmol Vis Sci 2007;48:3662–3668. [DOI] [PubMed] [Google Scholar]
- 22.Balk LJ, Steenwijk MD, Tewarie P, et al. Bidirectional trans-synaptic axonal degeneration in the visual pathway in multiple sclerosis. J Neurol Neurosurg Psychiatry 2014;86:419–424. [DOI] [PubMed] [Google Scholar]
- 23.Gabilondo I, Martínez-Lapiscina EH, Martínez-Heras E, et al. Trans-synaptic axonal degeneration in the visual pathway in multiple sclerosis. Ann Neurol 2014;75:98–107. [DOI] [PubMed] [Google Scholar]
- 24.Alshowaeir D, Yiannikas C, Garrick R, et al. Latency of multifocal visual evoked potentials in nonoptic neuritis eyes of multiple sclerosis patients associated with optic radiation lesions. Invest Ophthalmol Vis Sci 2014;55:3758–3764. [DOI] [PubMed] [Google Scholar]
- 25.Sakai RE, Feller DJ, Galetta KM, Galetta SL, Balcer LJ. Vision in multiple sclerosis: the story, structure-function correlations, and models for neuroprotection. J Neuroophthalmol 2011;31:362–373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Walter SD, Ishikawa H, Galetta KM, et al. Ganglion cell loss in relation to visual disability in multiple sclerosis. Ophthalmology 2012;119:1250–1257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Di Maggio G, Santangelo R, Guerrieri S, et al. Optical coherence tomography and visual evoked potentials: which is more sensitive in multiple sclerosis? Mult Scler 2014;20:1342–1347. [DOI] [PubMed] [Google Scholar]
- 28.Naismith RT, Tutlam NT, Xu J, et al. Optical coherence tomography is less sensitive than visual evoked potentials in optic neuritis. Neurology 2009;73:46–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Araie M. Test-retest variability in structural parameters measured with glaucoma imaging devices. Jpn J Ophthalmol 2013;57:1–24. [DOI] [PubMed] [Google Scholar]
- 30.Watson GM, Keltner JL, Chin EK, Harvey D, Nguyen A, Park SS. Comparison of retinal nerve fiber layer and central macular thickness measurements among five different optical coherence tomography instruments in patients with multiple sclerosis and optic neuritis. J Neuroophthalmol 2011;31:110–116. [DOI] [PubMed] [Google Scholar]
- 31.Schippling S, Balk L, Costello F, et al. Quality control for retinal OCT in multiple sclerosis: validation of the OSCAR-IB criteria. Mult Scler 2015;21:163–170. [DOI] [PubMed] [Google Scholar]
- 32.Rinalduzzi S, Brusa A, Jones SJ. Variation of visual evoked potential delay to stimulation of central, nasal, and temporal regions of the macula in optic neuritis. J Neurol Neurosurg Psychiatry 2001;70:28–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hood DC, Odel JG, Winn BJ. The multifocal visual evoked potential. J Neuroophthalmol 2003;23:279–289. [DOI] [PubMed] [Google Scholar]
- 34.Jenkins T, Ciccarelli O, Toosy A, et al. Dissecting structure-function interactions in acute optic neuritis to investigate neuroplasticity. Hum Brain Mapp 2010;31:276–286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Klistorner A, Arvind H, Garrick R, Graham SL, Paine M, Yiannikas C. Interrelationship of optical coherence tomography and multifocal visual-evoked potentials after optic neuritis. Invest Ophthalmol Vis Sci 2010;51:2770–2777. [DOI] [PubMed] [Google Scholar]
- 36.Klistorner A, Arvind H, Nguyen T, et al. Axonal loss and myelin in early ON loss in postacute optic neuritis. Ann Neurol 2008;64:325–331. [DOI] [PubMed] [Google Scholar]
- 37.Klistorner A, Arvind H, Nguyen T, et al. Multifocal VEP and OCT in optic neuritis: a topographical study of the structure-function relationship. Doc Ophthalmol 2009;118:129–137. [DOI] [PubMed] [Google Scholar]
- 38.Yang EB, Hood DC, Rodarte C, Zhang X, Odel JG, Behrens MM. Improvement in conduction velocity after optic neuritis measured with the multifocal VEP. Invest Ophthalmol Vis Sci 2007;48:692–698. [DOI] [PubMed] [Google Scholar]
- 39.Cadavid D, Levin N, Costello F, Rahilly A, Klistorner A. Technical feasibility of implementing multifocal VEP for multicenter clinical trials. Neurology 2013;80:P02.245. [Google Scholar]
- 40.Grossman RI. Magnetization transfer in multiple sclerosis. Ann Neurol 1994;36(suppl):S97–S99. [DOI] [PubMed] [Google Scholar]
- 41.Le Bihan D, Mangin JF, Poupon C, et al. Diffusion tensor imaging: concepts and applications. J Magn Reson Imaging 2001;13:534–546. [DOI] [PubMed] [Google Scholar]
- 42.Melzi L, Rocca MA, Marzoli SB, et al. A longitudinal conventional and magnetization transfer magnetic resonance imaging study of optic neuritis. Mult Scler 2007;13:265–268. [DOI] [PubMed] [Google Scholar]
- 43.Wang Y, van der Walt A, Paine M, et al. Optic nerve magnetisation transfer ratio after acute optic neuritis predicts axonal and visual outcomes. PLoS One 2012;7:e52291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Naismith RT, Xu J, Tutlam NT, et al. Disability in optic neuritis correlates with diffusion tensor-derived directional diffusivities. Neurology 2009;72:589–594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Naismith RT, Xu J, Tutlam NT, et al. Diffusion tensor imaging in acute optic neuropathies: predictor of clinical outcomes. Arch Neurol 2012;69:65–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Xu J, Sun SW, Naismith RT, Snyder AZ, Cross AH, Song SK. Assessing optic nerve pathology with diffusion MRI: from mouse to human. NMR Biomed 2008;21:928–940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Heesen C, Böhm J, Reich C, Kasper J, Goebel M, Gold SM. Patient perception of bodily functions in multiple sclerosis: gait and visual function are the most valuable. Mult Scler 2008;14:988–991. [DOI] [PubMed] [Google Scholar]
- 48.Schinzel J, Zimmermann H, Paul F, et al. Relations of low contrast visual acuity, quality of life and multiple sclerosis functional composite: a cross-sectional analysis. BMC Neurol 2014;14:31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Mowry EM, Loguidice MJ, Daniels AB, et al. Vision related quality of life in multiple sclerosis: correlation with new measures of low and high contrast letter acuity. J Neurol Neurosurg Psychiatry 2009;80:767–772. [DOI] [PubMed] [Google Scholar]
- 50.Raz N, Hallak M, Ben-Hur T, Levin N. Dynamic visual tests to identify and quantify visual damage and repair following demyelination in optic neuritis patients. J Vis Exp Epub 2014 Apr 14. doi: 10.3791/51107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Raphael BA, Galetta KM, Jacobs DA, et al. Validation and test characteristics of a 10-item neuro-ophthalmic supplement to the NEI-VFQ-25. Am J Ophthalmol 2006;142:1026–1035. [DOI] [PubMed] [Google Scholar]
- 52.Nolan RC, Galetta KM, Wilson JA, et al. Quality of life after optic neuritis in MS: new data for the 10-item neuro-ophthalmic supplement to the NEI-VFQ-25. Poster presented at: 40th Annual Meeting of the North American Neuro-Ophthalmology Society; March 1–6, 2014; Rio Grande, Puerto Rico.
- 53.Sühs KW, Hein K, Pehlke JR, Käsmann-Kellner B, Diem R. Retinal nerve fibre layer thinning in patients with clinically isolated optic neuritis and early treatment with interferon-beta. PLoS One 2012;7:e51645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Balcer LJ, Galetta SL, Calabresi PA, et al. Natalizumab reduces visual loss in patients with relapsing multiple sclerosis. Neurology 2007;68:1299–1304. [DOI] [PubMed] [Google Scholar]
- 55.Meuth SG, Bittner S, Seiler C, Gobel K, Wiendl H. Natalizumab restores evoked potential abnormalities in patients with relapsing-remitting multiple sclerosis. Mult Scler 2011;17:198–203. [DOI] [PubMed] [Google Scholar]
- 56.Noseworthy JH, O'Brien PC, Petterson TM, et al. A randomized trial of intravenous immunoglobulin in inflammatory demyelinating optic neuritis. Neurology 2001;56:1514–1522. [DOI] [PubMed] [Google Scholar]
- 57.Sühs KW, Hein K, Sättler MB, et al. A randomized, double-blind, phase 2 study of erythropoietin in optic neuritis. Ann Neurol 2012;72:199–210. [DOI] [PubMed] [Google Scholar]
- 58.Tsakiri A, Kallenbach K, Fuglø D, Wanscher B, Larsson H, Frederiksen J. Simvastatin improves final visual outcome in acute optic neuritis: a randomized study. Mult Scler 2012;18:72–81. [DOI] [PubMed] [Google Scholar]
- 59.Johnson MA, Cadavid D. Simvastatin in acute optic neuritis. Mult Scler 2012;18:1657; author reply 1658. [DOI] [PubMed] [Google Scholar]
- 60.Tran JQ, Rana J, Barkhof F, et al. Randomized phase I trials of the safety/tolerability of anti-LINGO-1 monoclonal antibody BIIB033. Neurol Neuroimmunol Neuroinflamm 2014;1:e18. 10.1212/NXI.0000000000000018. [DOI] [PMC free article] [PubMed] [Google Scholar]