

Abstract
Objectives To describe a technique for harvesting larger temporal bone specimens from human cadavers for the training of otolaryngology residents and fellows on the various approaches to the lateral and posterolateral skull base.
Design Human cadaveric anatomical study. The calvarium was excised 6 cm above the superior aspect of the ear canal. The brain and cerebellum were carefully removed, and the cranial nerves were cut sharply. Two bony cuts were performed, one in the midsagittal plane and the other in the coronal plane at the level of the optic foramen.
Setting Medical school anatomy laboratory.
Participants Human cadavers.
Main Outcome Measures Anatomical contents of specimens and technical effort required.
Results Larger temporal bone specimens containing portions of the parietal, occipital, and sphenoidal bones were consistently obtained using this technique of two bone cuts. All specimens were inspected and contained pertinent surface and skull base landmarks.
Conclusions The skull base block method allows for larger temporal bone specimens using a two bone cut technique that is efficient and reproducible. These specimens have the necessary anatomical bony landmarks for studying the complexity, utility, and limitations of lateral and posterolateral approaches to the skull base, important for the education of otolaryngology residents and fellows.
Keywords: temporal bone, temporal bone removal, temporal bone harvest, block method, modified block method, skull base
Introduction
The dissection of temporal bone specimens has been performed for > 100 years and has been instrumental in our modern-day understanding of middle ear, mastoid, and skull base anatomy and surgery. Harvesting intact temporal bone specimens from human cadavers is a technically challenging process that is invaluable in the education of medical students, otolaryngology and neurosurgery residents, and fellows.1 Dissection of these specimens is important for understanding the anatomical components of the temporal bone and their proximity to adjacent structures in all three dimensions, for practicing surgical procedures, and in comprehending surgical anatomy of the temporal bone.2
We describe a simple and novel technique of harvesting temporal bone specimens from human cadavers called the skull base block method (SBBM). In this technique, specimens are larger in the anterior, posterior, superior, and inferior dimensions when compared with the traditional block methods (BMs) or modifications of the BM,2 because they contain portions of adjoining occipital, sphenoidal, and parietal bones.
Methods
This study was a collective effort between the Department of Otolaryngology at the University of Miami and the Department of Cell Biology and Anatomy. Consent was obtained through the Department of Cell Biology and Anatomy for the dissection of the temporal bones in human cadavers. Instruments used during the dissection include a Stryker autopsy saw (Kalamazoo, Michigan, United States), hand saw, large blade scalpel, pair of heavy scissors, hammer, and large osteotome.
Similar to other methods of temporal bone removal, the scalp was incised ∼ 6 cm above the external auditory canal circumferentially around the calvarium. An electric saw was then used to make bony cuts circumferentially around the skull at this level. The brain was carefully lifted from the bony vault, the tentorium was incised to elevate the cerebellum, and all cranial nerves (CNs) were sharply amputated using a scalpel at the brainstem. Subsequently, the cranial skull base could be visualized.
In the SBBM (Fig. 1A), the first bony cut was made in the midsagittal plane from the optic foramen to the occipital bone, proceeding inferiorly to the second cervical vertebra. The second bony cut was made in the coronal plane at the level of the optic foramen spanning the lateral aspects of the right and left temporal bones. When needed, hand saw, hammer, and osteotome aided in deeper dissection to continue the bone cuts inferiorly through the angles of the mandible. Then the remaining skin and soft tissues of the face and neck were cut with heavy scissors in an axial plane at the level of the oral commissure until the entire temporal bone specimen was only attached by the cervical vertebrae. Lastly, C1 was dislocated from the C2 vertebrae, and the two temporal specimens were removed.
Fig. 1.
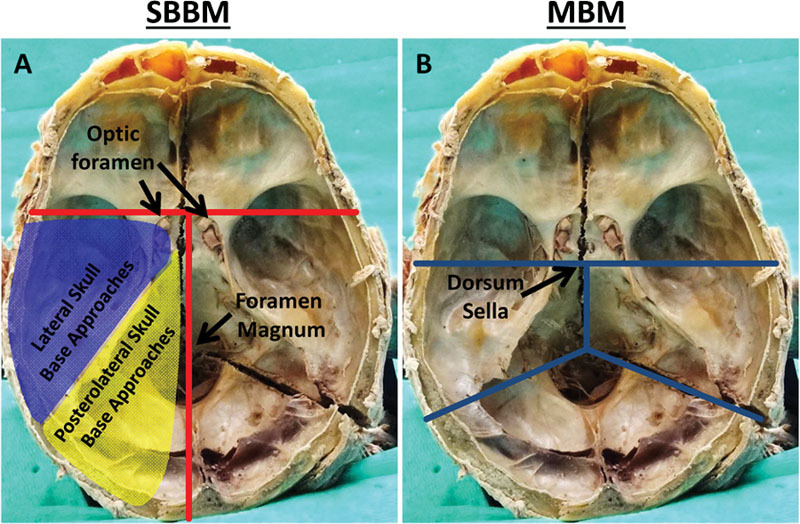
(A) The skull base block method (SBBM) requires two bone cuts (red lines): one in the midsagittal plane and the second in a coronal plane across bilateral optic foramina. The approaches to the lateral skull bases and posterolateral skull base are highlighted in blue and yellow, respectively. (B) The modified block method (MBM) requires four bone cuts (blue lines).
In the modified block method (MBM), four bony cuts are made through the dorsum sella, midsagittal plane, and oblique planes in the right and left posterior cranial fossae (Fig. 1B). The soft tissue is dissected off the temporal bone specimens, and the temporomandibular joint is dislocated from the glenoid fossa.2 In one cadaveric head, the SBBM was performed on the left side and the MBM was performed on the right side to juxtapose the two techniques (Fig. 1C).
Results
The SBBM was performed on eight human cadavers. The skull base specimens obtained by the SBBM were inspected and possessed necessary surface and skull base landmarks important for the study of approaches to the lateral and posterolateral skull base. The specimens were larger than those obtained from the MBM (Fig. 2), and they possessed all portions of the temporal bone including the squamous, mastoid, petrous, tympanic, and styloid components and portions of the adjacent parietal, sphenoidal, and occipital bones. The auricle, external auditory canal, condyle, ramus, mandibular angle, part of the zygomatic arch, CNs II through XII, superior petrosal and transverse sinuses, intact dura of the middle and posterior fossae, eustachian tube orifice, and contents of the carotid sheath were also present.
Fig. 2.
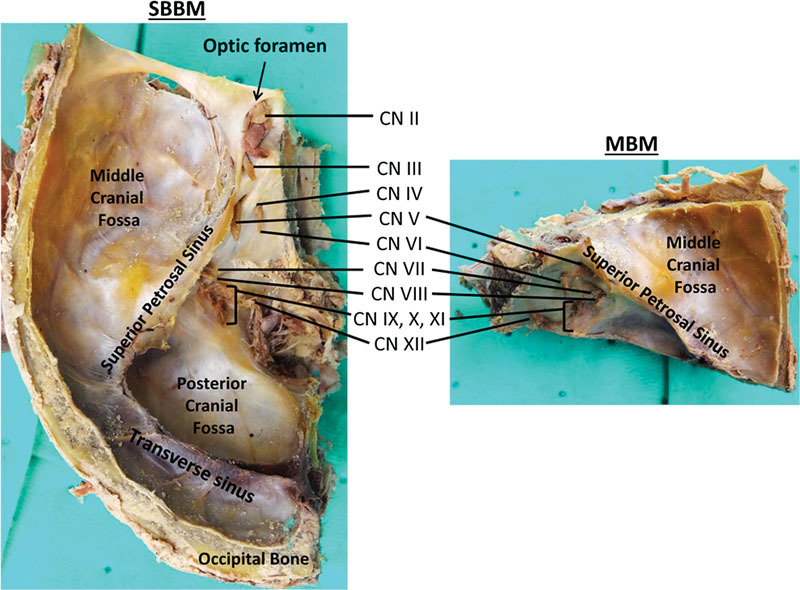
The skull base block method (SBBM) produces larger temporal bones than the modified block method (MBM). Temporal bones obtained using the SBBM contain cranial nerves (CNs) II and III, the transverse sinus, a significantly greater portion of the middle and posterior cranial fossae, as well as other extracranial skull base structures that specimens obtained by the MBM do not possess.
Discussion
Several techniques have been described for temporal bone removal, such as the bone plug cutter method, the traditional BM, and several modifications of the BM.1 2 3 4 5 The SBBM is a novel, simple, and efficient way to section bilateral temporal bone specimens from human cadavers for the study of skull base anatomy using two bony cuts. Larger specimens are possible with this technique and are more suitable for studying the complexity, utility, and limitations of various approaches to the lateral and posterolateral skull base that are important for surgical planning.
These larger specimens allow for dissection and study of vital structures such as the carotid artery as it courses from the neck and through the petrous apex before it traverses the cavernous sinus. Understanding the three-dimensional relationships of the superior petrosal, transverse, sigmoid, and inferior petrosal sinuses as well as the jugular bulb and internal jugular vein are crucial to avoid excessive bleeding, air emboli, and cerebrovascular complications during surgery. Advantages and limitations of exposures obtained by the middle cranial fossa, translabyrinthine, and retrosigmoid approaches to the internal auditory canal for resection of intracanalicular and cerebellopontine angle tumors can also be examined in these larger temporal bone specimens (Fig. 3A). Furthermore, combined petrosal approaches to the petroclival junction (Fig. 3B), transzygomatic approaches to the infratemporal fossa, and transmastoid and transcervical approaches to the jugular foramen can also be studied in these larger specimens that cannot be adequately examined in smaller temporal bones. Fewer separate bony cuts and two skull base specimens per head offer additional advantages. Storage for two larger skull base specimens is easier than for complete heads. However, the main limitation to the SBBM for skull base training is that the brain has been removed and CNs severed.
Fig. 3.
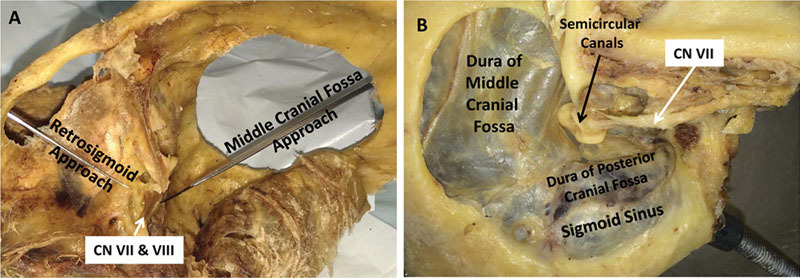
(A) Relationship between retrosigmoid and middle cranial fossa approach to the internal auditory canal. (B) Combined middle cranial fossa and retrolabyrinthine approach for petroclival lesions. CN, cranial nerve.
Conclusion
The SBBM is a quick and efficient method for harvesting larger temporal bones using a two bone cut technique. These larger temporal bone specimens are great resources for otolaryngology residents and fellows for studying the complexity, utility, and limitations of various approaches to the lateral and posterolateral skull base that cannot be performed in smaller temporal bones.
Acknowledgments
The authors acknowledge Associate Professor Thomas Champney from the Department of Cell Biology and Anatomy for his assistance and support.
References
- 1.Nadol J B Jr. Techniques for human temporal bone removal: information for the scientific community. Otolaryngol Head Neck Surg. 1996;115(4):298–305. doi: 10.1016/S0194-5998(96)70042-6. [DOI] [PubMed] [Google Scholar]
- 2.Walvekar R R, Harless L D, Loehn B C, Swartz W. Block method of human temporal bone removal: a technical modification to permit rapid removal. Laryngoscope. 2010;120(10):1998–2001. doi: 10.1002/lary.21052. [DOI] [PubMed] [Google Scholar]
- 3.Schuknecht H. Temporal bone removal at autopsy. Preparation and uses. Arch Otolaryngol. 1968;87(2):129–137. doi: 10.1001/archotol.1968.00760060131007. [DOI] [PubMed] [Google Scholar]
- 4.Sando I, Doyle W, Okuno H, Takahara T, Kitajiri M, Coury W J III. How to remove, process, and study the temporal bone with the entire eustachian tube and its accessory structures: a method for histopathological study. Auris Nasus Larynx. 1985;12 01:S21–S25. doi: 10.1016/s0385-8146(85)80089-4. [DOI] [PubMed] [Google Scholar]
- 5.Sando I, Doyle W J, Okuno H, Takahara T, Kitajiri M, Coury W J III. A method for the histopathological analysis of the temporal bone and the eustachian tube and its accessory structures. Ann Otol Rhinol Laryngol. 1986;95(3 Pt 1):267–274. doi: 10.1177/000348948609500311. [DOI] [PubMed] [Google Scholar]