

Abstract
Background and aims. Early Childhood Caries (ECC) is a public health problem with biological, social and behavioural determinants and the notion that the principal etiology is inappropriate feeding modalities is no longer tenable. Hence this study was undertaken to assess the relationship between ECC and socio-demographic factors, dietary habits, oral hygiene habits and parental characteristics.
Materials and methods. The study involved a dental examination of 1400 children aged 0-71 months, recording caries using Gruebbel’s deft index and a structured questionnaire to interview parents or caretakers. The tabulated data was statistically analyzed using t-test and ANOVA at 5% level of significance.
Results. The variables significantly associated with ECC were age (P<0.001), geographical location (P<0.05), duration of breast/bottle feeding (P<0.001), use of sweetened pacifiers (P<0.001), frequency of snacking (P<0.05), frequency of tooth brushing (P<0.001), the person responsible for child’s oral health care (P<0.05) and education level of parents (P<0.05). However, other variables like child’s gender, number of siblings, types of snack the child preferred and age at which tooth brushing was instituted did not have statistically significant relationship with ECC (P>0.05).
Conclusion. ECC is preventable and manageable with proper information and skills. It is important for healthcare professionals, family physicians and parents to be cognizant of the involved risk factors as their preventive efforts represent the first line of defense.
Keywords: Preschool children, dental caries, questionnaire, risk factors, tooth brushing
Introduction
Dental caries is a multifactorial disease that starts with microbiological shifts within the complex biofilm and is affected by salivary flow and composition, exposure to fluoride, consumption of dietary sugars, etc.1Dental caries affects humans of all ages all over the world and remains a major dental health problem among schoolchildren globally.2 It is a disease that can never be eradicated because of the complex interaction of cultural, social, behavioral, nutritional and biological risk factors that are associated with its initiation and progression.3
Childhood and early adolescence are crucial periods in the development of healthy dentition. ECC is a major public health problem, being the most common chronic infectious childhood disease, which is difficult to control. While not life-threatening, its impact on individuals and communities is considerable, resulting in pain, impairment of function, deleterious influence on the child’s growth rate, body weight, and ability to thrive, thus reducing quality of life.4
Caries in infants and young children has long been recognized as a clinical syndrome, described by Belterami5 in 1930s as “Les dents noire de tout-petits” which means “black teeth of the very young.” Fass is perhaps the most popular in this perspective for defining the term “nursing bottle mouth”.6
Subsequently, other terms such as “baby bottle tooth decay”, “nursing bottle syndrome”, “bottle mouth caries”, “nursing caries”, “rampant caries”, “nursing bottle mouth”, “milk bottle syndrome”, “breast milk tooth decay” and “facio-lingual pattern of decay” have also been used to describe this condition.7
ECC was historically attributed to inappropriate and prolonged bottle use or breastfeeding. The use of the bottle, especially at bedtime, is believed to be associated with increased risk for caries, but this might not be the only factor in caries development in early childhood. The associated risk factors have also been found to vary from population to population.8 Moreover, the associations between ECC and improper feeding modalities are not consistent,9,10 and they are no longer considered to be the principal etiology. Fruit juices and carbonated beverages have also been implicated in children diagnosed with ECC.
Some studies have reported that a child’s brushing habit and frequency of brushing are also associated with the occurrence and development of dental caries.11,12 The education level of parents has been shown to be co-related with the occurrence and severity of ECC in their children. Lower prevalence of dental caries have been associated with higher levels of parental education.13 ECC is more common in children from single-parent families and those with parents of low educational level, especially of illiterate mothers.14
The universal prevalence of dental disease is a constant reminder of the need for effective preventive dental health education. Intervention during early childhood would seem to be the most appropriate action to ensure healthy dental habits throughout life. For the implementation of preventive attributes in a given population, knowledge about the existing standards of health and existing practices and attributes of that particular population is essential.
Hence this study aimed to assess the associations between early childhood caries and child’s age, gender, feeding habits, brushing habits, dietary habits and socioeconomic status of parents so that the physical, psychological and economic consequences of ECC can be avoided.
Materials and Methods
The study sample comprised of 1400 preschool children age 71 months or younger with early childhood caries reporting to the Outpatient Department of Pedodontics and Preventive Dentistry, Postgraduate Institute of Dental Sciences, Rohtak, Haryana (India), during the study period. Consent was obtained for dental examination of the child from the concerned guardian to cooperate with the examiner explaining the importance of the study. The children with any systemic or any congenital syndromes or suffering from any skeletal and dental developmental disorders were excluded from the study.
The accompanying guardians were first interviewed with a self-designed, structured questionnaire (see Additional file 1). The questionnaire consisted of 5 parts. Part I included questions on general information (age, sex, address, number of siblings) about the children; in parts II and III feeding and dietary habits of the children were assessed. Parts IV and V of the questionnaire determined the oral hygiene habits and socioeconomic status of the children, respectively. Prior to being finalized, the questionnaire was pilot-tested on a group of 100 parents to ensure validity and reliability. The questionnaire’s reliability was checked using SPSS, and Cronbach’s alpha coefficient was estimated at 0.79. The interviewer himself recorded the answers to the questions in order to minimize misinterpretation of questions and to ensure uniformity in data.
The dental examination was carried out in the clinic with the patient sitting comfortably in dental chair or using the knee-to-knee examination method in case of very young children. All the primary teeth were examined using a mouth mirror and a dental explorer. Diagnosis depended upon visual evidence of lesion. The explorer was used only to remove food debris and no attempt was made to use an explorer to confirm catch of the lesions. No radiographs were taken for any child. Sterilized instruments and separate gloves were used for each patient. Caries status of each child was recorded using ‘def’ index as described by Gruebbel in 1944.15
As defined by Gruebbel:
d = decayed teeth (evidence of dental caries, cavitation, including filled teeth with recurrent caries),
e = extracted teeth and decayed teeth indicated for extraction due to caries,
f = filled (restored teeth without recurrent caries).
Calculation of def index: Total d + e + f = def
Data management and statistical analysis was carried out using SPSS 19 to derive the results and draw conclusion. The statistical tests used were t-test for significance of differences in mean values between the two groups and ANOVA for significance of differences in mean values between more than two groups. Statistical significance was set at P<0.05.
Results
The study sample included 1400 children aged ≤71 months. Caries status of each child was recorded using ‘def’ index as described by Gruebbel in 1944.
The decayed teeth (92.6%) constituted the major component of deft, with missing teeth contributing to only 5.7% and filled teeth to only 1.7 % of deft (Figure 1).
Figure 1.
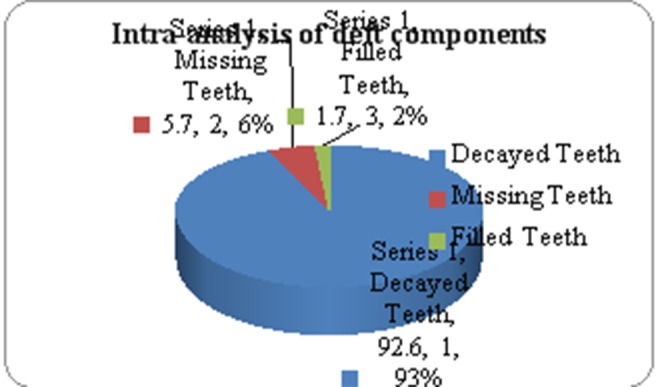
Intra-analysis of deft components
As shown in Table 1, the mean deft increased with age and differences in mean deft between different age groups were found to be highly significant statistically (P<0.001). The study sample included 686 (49%) male and 714 (51%) female children, with no significant differences in deft between male and female children (P>0.05). The mean deft was higher (5.19±2.909) in children from rural areas compared to those from urban areas (4.66±2.113). No significant association was found between deft and the number of siblings (P>0.05).
Table 1. Demographic characteristics and ECC .
| Number of children | % | Average deft | Standard deviation | P | |||
| 1 | Age | 0-12 mos | 0 | 0 | 0 | 0 | P<0.001 |
| 12-23 mos | 14 | 1 | 1 | 0.00 | |||
| 24-35 mos | 140 | 10 | 2.1 | 0.703 | |||
| 36-47 mos | 308 | 22 | 3.72 | 0.864 | |||
| 48-59 mos | 490 | 35 | 4.74 | 1.156 | |||
| 60-71 mos | 448 | 32 | 4.88 | 3.10 | |||
| 2 | Gender | Male | 686 | 49 | 4.92 | 2.844 | P>0.05 |
| Female | 714 | 51 | 4.84 | 2.082 | |||
| 3 | Geographical location | Rural | 574 | 41 | 5.19 | 2.909 | P<0.05 |
| Urban | 826 | 59 | 4.66 | 2.113 | |||
| 4 | Number of siblings | 0 | 154 | 11 | 4.81 | 2.13 | P>0.05 |
| 1 | 672 | 48 | 5.08 | 2.50 | |||
| 2 | 490 | 35 | 4.74 | 2.625 | |||
| 3 or more | 84 | 6 | 4.16 | 1.875 |
Table 2summarizes the association of ECC with feeding habits of children. The average deft was lowest (4.65±1.996) in children who were breast-fed only up to 1 year of age and highest (5.2±2.978) in children who were breast-fed for more than 2 years and this difference in deft was found to be statistically significant (P<0.05). Of 1400 children, only 28 (2%) children were not bottle-fed, 784 (56%) children were bottle-fed for 1‒2 years and 364 (26%) children were bottle-fed for more than 2 years. The mean deft was lowest (1.5±0.509) in children who were not bottle-fed and highest (6.3±2.675) in children who were fed for more than 2 years. There was also a strong association between deft and use of sweetened pacifiers (P<0.001).
Table 2. Feeding habits, dietary habits and ECC.
| No. of children | % | Average Deft | Standard deviation | P | |||
| 1 | Duration of breast-feeding | <1 year | 448 | 32 | 4.65 | 1.996 | P<0.05 |
| 1-2 year | 742 | 53 | 4.92 | >2.585 | |||
| >2 year | 210 | 15 | 5.2 | 2.978 | |||
| 2 | Duration of bottle-feeding | Not Bottle fed |
28 | 2 | 1.5 | 0.509 | P<0.001 |
| <1 year | 224 | 16 | 3.37 | 1.320 | |||
| 1-2 year | 784 | 56 | 4.76 | 2.277 | |||
| >2 year | 364 | 26 | 6.3 | 2.675 | |||
| 3 | Whether child fell asleep with bottle/breast-feeding at night | Yes | 1036 | 74 | 5.31 | 2.532 | P<0.001 |
| No | 364 | 26 | 3.65 | 1.862 | |||
| 4 | Use of sweetened pacifiers | No | 1078 | 7 | 4.4 | 2.159 | P<0.001 |
| Yes | 322 | 23 | 6.4 | 2.815 | |||
| 5 | Frequency of snacking between meals | Seldom | 56 | 4 | 2.75 | 1.3111 | P<0.05 |
| Once | 182 | 13 | 3.07 | 1.210 | |||
| Twice | 560 | 40 | 5.27 | 2.392 | |||
| >3times | 602 | 43 | 5.32 | 2.597 | |||
| 6 | Type of snacks preferred | Sugary | 840 | 60 | 4.93 | 2.576 | P>0.05 |
| Salty | 560 | 40 | 4.8 | 2.339 |
There was a significant increase in deft with frequent snacking (P<0.05) but the difference in deft between children who preferred sugary snacks than in children who preferred salty snacks was not found to be statistically significant (P>0.05; Table 2).
The average deft was lower (1.5±0.509) among the children who brushed their teeth twice daily compared to those who brushed their teeth once daily (4.3±1.012) and average deft was highest (5.42±3.048) in children who did not brush at all. However, the association between the age of commencement of tooth brushing and average deft was not found to be statistically significant (P>0.05).The education level of mother and whether both parents were working had a significant association with the severity of decay (P<0.05; Table 3).
Table 3. Oral hygiene habits, social factors and ECC .
| No. of children | % | Average Deft | Standard deviation | P | |||
| 1 | Frequency of Tooth Brushing | No brushing | 784 | 56 | 5.42 | 3.048 | p<0.001 |
| Once | 588 | 42 | 4.3 | 1.012 | |||
| Twice | 28 | 2 | 1.5 | 0.509 | |||
| 2 |
Age at which
tooth brushing started |
No brush | 784 | 56 | 5.4 | 3.048 | p>0.05 |
| <2 year | 154 | 11 | 4 | 1.048 | |||
| 2-3 year | 238 | 17 | 4.05 | 1.477 | |||
| >3 year | 224 | 16 | 4.43 | 0.706 | |||
| 3 | Whether the mother assisted child in tooth brushing or not | Yes | 336 | 24 | 4.20 | 1.259 | p<0.05 |
| No | 1064 | 76 | 5.09 | 2.726 | |||
| 4 |
Whether both parents were
working outside home or not |
Yes | 350 | 25 | 5.36 | 2.942 | p<0.05 |
| No | 1050 | 75 | 4.72 | 2.291 | |||
| 5 | Educational level of mother | Illiterate | 224 | 16 | 5.87 | 3.245 | p<0.05 |
| School level | 504 | 36 | 5.13 | 2.499 | |||
| Graduate | 672 | 48 | 4.35 | 2.007 |
Discussion
ECC is a complex disease in which various genetic, environmental and behavioral risk factors interact. Many of these variables are highly influenced by the prevailing socioeconomic conditions, behavioral patterns and educational levels. The caries prevalence and severity cannot be determined by taking into consideration any one factor. All the factors have to be considered as a whole for health promotion so as to help promote new preventive and treatment strategies for dental caries. The term “early childhood caries” was suggested at a 1994 workshop sponsored by the Centers for Disease Control and Prevention in an attempt to focus attention on the multiple factors (i.e. socioeconomic, behavioral and psycho-social) that contribute to caries at such early ages, rather than ascribing sole causation to inappropriate feeding methods.16
The results of this study demonstrated that in ‘d’ component (92.6%) dominated the ‘deft’ score. The low level of dental treatment was attributed to limited accessibility to preventive and treatment services, unwillingness of practitioners to provide care for young children and primary teeth being a low priority for consideration of treatment because of a parental belief that they are temporary.
Demographic Characteristics and ECC
The caries severity increased with age in primary dentition. This can be explained by the fact that dental caries is a cumulative process and develops over years. Thus the decayed teeth increased with age. This is in accordance with the study carried out by Hold et al (1982),17 Roeters et al (1995),18 Namal et al (2005),19 and Retnakumari (2012).20 This indicates that educational programs intended to prevent caries in deciduous teeth should begin in the first year of life among children before the condition becomes too advanced to prevent, with a view to avoiding the difficulties and huge expenses.
The mean deft was higher in children from rural areas than those from urban areas and the difference in deft was found to be statistically significant (P<0.05). This is in accordance with studies by Matilla et al (2000)21 and Du Minquan et al (2007).22 This can be explained on the basis that rural children reported less use of toothpaste or brushes, less frequent visits to a dentist and more frequent intake of sugary food. No significant association (P>0.05) was found between mean deft and the number of siblings in the present study. Namal et al (2005)19 also reported that the number of siblings did not increase dental caries significantly; however, there was still a slight increase.
Feeding Habits and ECC
As this study also attempted to assess the influence of feeding habits on ECC, it was concluded that breast-feeding for longer duration increases the risk of nursing caries. Thus, although breast milk contains other immunological, nutritional and psychological advantages, prolonged breast-feeding seems to be correlated to dental diseases.23 Breast milk contains lactose (7%) at a higher concentration compared to bovine milk. There is decreased severity of early childhood caries with breast-feeding up to 12 months of age as compared with no breast-feeding at all. However, Albbey24 reported that breast-feeding, if unrestricted, results in early caries development in infants. In addition, the highest deft was recorded in children who were bottle-fed for more than 2 years. Hallet et al (2003),25 Mazhari et al (2007),26 Ekta Malvania et al (2011)27 and Retnakumari et al (2012)20 also reported increasing severity of caries with increasing duration of bottle-feeding.
In this study it was observed that 74% of children were bottle/breast-fed over night and night feeding habit was significantly associated with much more caries experience. This finding can be attributed to the fact that there is less salivary flow at night and hence less capacity for neutralization. This causes stagnation of milk in the mouth for longer periods of time and prolonged exposure of teeth to fermentable carbohydrates. The conclusion of the present finding supports AAPD statement that ‘ad libitum nocturnal breast-feeding should be avoided after the primary teeth begin to erupt’.
Dietary Habits and ECC
The frequent intake of sweet snacks increased the risk of developing dental caries in young children, supporting nutritional recommendation of “limiting snacking times in children and encouraging regular meals but the association between type of snacks preferred and caries severity was not found to be statistically significant (P>0.05). This is consistent with a study by Maciel et al (2001),14 who also reported no statistically significant relationship between preference for sweets and dental caries in 4-5-year-old Brazilian children.
Brushing Habits and ECC
In this study 56% of children did not brush at all while 42% brushed once daily. The average deft decreased as the brushing frequency increased and deft was lowest in children who brushed twice daily. This is in contrast with studies by Febres et al (1997)28 and Milgrom et al (2000),29 who failed to find any relationship between tooth brushing frequency and caries. This study supports that children who started brushing late had higher prevalence of early childhood caries so tooth brushing should be instituted when the first primary tooth erupts. Parents are models for their children and the establishment of healthy habits in their children is an important strategy for health promotion of their children. The lowest deft was found in subjects who had the supervision or assistance of an adult in brushing their teeth.
Social Factors and ECC
Mother’s educational level also proved to be a significant predictor for caries experience in the current study. Since mothers have a major influence on the oral health behavior (feeding practices, dietary habits, food choices and tooth brushing) of their children, lack of education and information potentially influenced the child’s health status. Szatko and co-workers30 also found a strong interdependence on the mother’s level of knowledge with that of her educational level which influenced the child’s oral health.
Conclusion
ECC cannot be considered only an infectious dental disease and multiple factors are involved in its etiology. It would be advisable to reach these children in time and to inform the parents about the possible causes of ECC. Thus, substantial efforts are required for early detection and treatment, and effective preventive strategies should be implemented to decrease the prevalence of ECC in preschool children.
Additional file 1. The questionnaire used for the study. This material is available online as a Word 97-2003 Document.
References
- 1.Selwitz RH, Ismail A I, Pitts AI. Dental caries. Lancet. 2007;369:51–9. doi: 10.1016/s0140-6736(07)60031-2. [DOI] [PubMed] [Google Scholar]
- 2. World Health Organisation (WHO). Global strategy for infant and young child feeding. Geneva: WHO 2003.
- 3.Ismail AI, Tanzer JM, Dingle JL. Current trends of sugar consumption in developing societies. Community Dent Oral Epidemiol. 1997;25:438–43. doi: 10.1111/j.1600-0528.1997.tb01735.x. [DOI] [PubMed] [Google Scholar]
- 4. American Academy of Pediatric Dentistry. Symposium on the prevention of oral disease in children and adolescents. Conference papers. Pediatr Dent 2006;28:96-198.
- 5. Belterami G. Les dents noires de tout-petits. Siecle Medical. In: Belterami G, ed. La Melandontie Infantile. Marseille: Leconte; 1952. [In French].
- 6.Fass E. Is bottle feeding of milk a factor in dental caries? J Dent Child 1962;29:245-51. J Dent Child. 1962;29:245–51. [Google Scholar]
- 7.Milnes AR. Description and epidemiology of nursing caries. J Public Health Dent. 1996;56:38–50. doi: 10.1111/j.1752-7325.1996.tb02394.x. [DOI] [PubMed] [Google Scholar]
- 8.RIPA LW. Nursing Caries: a comprehensive review. Pediatr Dent. 1988;10:268–82. [PubMed] [Google Scholar]
- 9.Tinanoff N. The Early Childhood Caries Conference, October 18-19, 1997. Pediatr Dent. 1997;19:453–4. [PubMed] [Google Scholar]
- 10.Tinanoff N, O’Sullivan DM. Early Childhood Caries: overview and recent findings. Pediatr Dent. 1997;19:12–6. [PubMed] [Google Scholar]
- 11.Vanobbergen J, Martens L, Lesaffre E, Bogaerts K, Declerck D. Assessing risk indicators for dental caries in the primary dentition. Community Dent Oral Epidemiol. 2001;29:424–34. doi: 10.1034/j.1600-0528.2001.290603.x. [DOI] [PubMed] [Google Scholar]
- 12.Tsai AI, Johnsen DC, Lin YH, Hsu KH. A study on risk factors associated with nursing caries in Taiwanese children aged 24-48 months. Int J Paediatr Dent. 2001;11:147–9. doi: 10.1046/j.1365-263x.2001.00258.x. [DOI] [PubMed] [Google Scholar]
- 13.AI-Hosani E, Rugg-Gunn A. Combination of low parental educational attainment and high parental income related to high caries experience in preschool children in Abu Dhabi. Community Dent Oral Epidemiol. 1998;26:31–6. doi: 10.1111/j.1600-0528.1998.tb02080.x. [DOI] [PubMed] [Google Scholar]
- 14.Maciel SM, Marcenes W, Sheiham A. The relationship between sweetness preference, level of salivary mutans streptococci and caries experience in Brazilian pre-school children. Int J Paediatr Dent. 2001;11:123–30. doi: 10.1046/j.1365-263x.2001.00259.x. [DOI] [PubMed] [Google Scholar]
- 15.Gruebbel AO. A measurement of dental caries prevalence and treatment service for deciduous teeth. J Dent Res. 1944;23:163–8. doi: 10.1177/00220345440230030201. [DOI] [Google Scholar]
- 16.Schroth RJ, Brothwell DJ, Moffatt ME. Caregiver knowledge and attitudes of preschool oral health and early childhood caries (ECC) Int J Circumpolar Health. 2007;66:153–67. doi: 10.3402/ijch.v66i2.18247. [DOI] [PubMed] [Google Scholar]
- 17.Holt RD, Joels D, Winter GB. Caries in pre-school children: The Camden Study. Br Dent J. 1982;153:107–9. doi: 10.1038/sj.bdj.4804862. [DOI] [PubMed] [Google Scholar]
- 18.Roeters J, Burgersdijk R, Truin GJ, van 't Hof M. Dental caries and its determinants in 2-to-5-year-old children. ASDC J Dent Child. 1995;62:401–8. [PubMed] [Google Scholar]
- 19.Namal N, Vehit HE, Can G. Risk factors for dental caries in Turkish preschool children. J Indian Soc Pedod Prev Dent. 2005;23:115–8. doi: 10.4103/0970-4388.16881. [DOI] [PubMed] [Google Scholar]
- 20.Retnakumari N, Cyriac G. Childhood caries as influenced by maternal and child characteristics in pre-school children of Kerala—an epidemiological study. Contemp Clin Dent. 2012;3:2–8. doi: 10.4103/0976-237x.94538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Matilla ML, Rautava P, Sillanpaa M, Paunio P. Caries in five- year old children and associations with family related factors. J Dent Res. 2000;79:875–81. doi: 10.1177/00220345000790031501. [DOI] [PubMed] [Google Scholar]
- 22.Du Minquan, Luo Y, Zeng X, Alkhatib N, Bedi R. Caries in preschool children and its risk factors in 2 provinces in China. Quintessence Int. 2007;38:143–51. [PubMed] [Google Scholar]
- 23.Kotlow LA. Breast feeding A cause of dental caries in children. J Dent Child. 1977;44:192–3. [PubMed] [Google Scholar]
- 24.Albbey LM. Is breast feeding a likely cause of dental caries in young children? J Am Dent Assoc. 1979;98:21–3. doi: 10.14219/jada.archive.1979.0028. [DOI] [PubMed] [Google Scholar]
- 25.KB Hallett, PK O’Rourke. Social and behavioural determinants of early childhood caries. Aust Dent J. 2003;48:27–33. doi: 10.1111/j.1834-7819.2003.tb00005.x. [DOI] [PubMed] [Google Scholar]
- 26.Mazhari F, Talebi M, Zoghi M. Prevalence of Early childhood caries and its risk factors in 6-60 months old children in Quchan. Dent Res J. 2007;4:96–101. [Google Scholar]
- 27.Malvania EA, Ajith Krishnan CG. Nursing caries prevalence among preschool children of Piparia village, Vadodara, Gujarat. J Oral Health Community Dent. 2011;5:37–41. [Google Scholar]
- 28.Febres C, Echeverri EA, Keene HJ. Parental awareness, habits, social factors and their relationship to baby bottle tooth decay. Pediatric Dent. 1997;19:22–7. [PubMed] [Google Scholar]
- 29.Milgrom P, Riedy CA, Weinstein P. Dental caries and its relationship to bacterial infection, hypoplasia, diet and oral hygiene in 6 to 36 month old children. Community Dent Oral Epidemiol. 2000;28:295–306. doi: 10.1034/j.1600-0528.2000.280408.x. [DOI] [PubMed] [Google Scholar]
- 30.Szatko F, Wierzbicka M, Dybizbanska E, Struzycka I, I Wanickafrankowska. Oral health of Polish three-year olds and mothers oral health-related knowledge. Community Dental Health. 2004;21:175–80. [PubMed] [Google Scholar]