

Abstract
Background
Dermatofibromas are common benign skin neoplasms.
Main observations
The authors report the clinical, dermoscopic and histopathological features of a hemosiderotic dermatofibroma mimicking melanoma in an 85-year-old woman.
Conclusions
Atypical dermoscopic patterns may prove difficult to differentiate from melanocytic lesions, and because of its polymorphic, melanoma-like presentation, definite diagnosis of hemosiderotic dermatofibroma can be reached by histopathological examination.
Keywords: dermatofibroma, dermoscopy, dermatoscopy, melanoma, skin cancer
Introduction
Dermatofibromas (DF) or fibrous histiocytomas are common benign skin neoplasms composed of fibrohistiocytic cells. They occur predominantly on the extremities or trunk of young adults, with a slight predominance in females. Clinically, these neoplasms appear as firm, single or multiple papules, plaques or nodules that are red to brown in colour. The lateral compression of dermatofibromas characteristically produce a depression in the overlying skin, that is the dimple sign.[1] Several histopathological variants have been described, including cellular, hemosiderotic / aneurysmal, atypical, epithelioid and deep fibrous histiocytomas.[2]
Although the knowledge of dermoscopic structures and patterns of DFs facilitates its clinical recognition, atypical patterns may prove difficult to differentiate from melanocytic lesions, including melanoma.
Case Report
An 85-year-old woman, skin type III, presented with an asymptomatic black macule on the right leg, which had been present for at least 3 years. She noticed progressive darkening of the lesion. The patient reported no previous trauma or insect bite to the area involved. She had no personal or family history of skin cancer. On examination, there was a hyperpigmented macule on the anterior aspect of the right leg with a background of moderate to severe actinic-damaged skin [Fig. 1]. The macule measured 8 mm and had irregular shape and borders. The dimple sign was absent.
Figure 1.

An irregular black macule (white arrow) with actinic-damaged skin on the anterior aright leg.
Dermoscopy with polarized light showed a lesion with asymmetrical structures and colour distribution. It showed atypical peripheral brown pigment network, central red to blue homogenous area with chrysalis and irregular dark brown blotches [Fig. 2].
Figure 2.
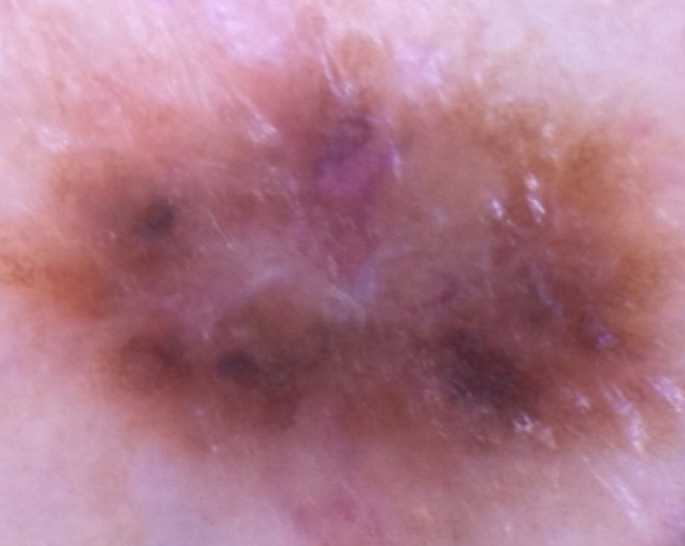
Dermoscopy (DermLite, DL3Ò, original magnification x 10): peripheral atypical brown pigment network, central red-bluish homogenous area with chrysalis, and irregular dark-brown blotches.
The lesion was completely excised. Histopathological examination revealed epidermal hyperplasia. A grenz zone was present between the epidermis and the dermal lesion. The dermis showed a dense fibrohistiocytic infiltrate with hemosiderin pigments deposition and dilated blood vessels. A grenz zone was present between the epidermis and the dermal lesion [Fig. 3].
Figure 3.
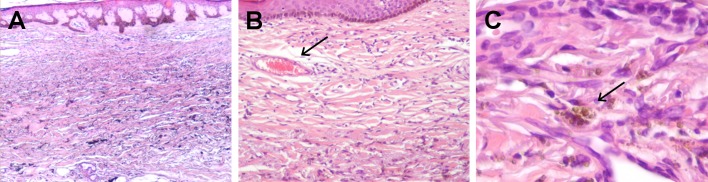
Histopathological examination: (A) hyperplasia of the epidermis with thickened rete ridges and basal hyperpigmentation and a dense infiltrate composed of fibrocytes and histiocytes; a grenz zone is seen between the epidermis and the dermal lesion (Haematoxylin and eosin, original magnification x40), (B) small-blood filled spaces (Haematoxylin and eosin, original magnification x100), and (C) hemosiderin deposition throughout the reticular dermis (Haematoxylin and eosin, original magnification x400).
Discussion
DFs can exhibit a wide range of clinical and dermoscopic patterns. In 2008, Zaballos et al. identified 10 global dermoscopic patterns associated with DF. The most common (35%) consists of a peripheral delicate annular pigment network with a central scar-like white patch. The remaining typical patterns may include only a single dermoscopic structure or a combination of delicate pigment network, central white patch, homogeneous brown pigmentation or white network. Less frequently, an atypical pattern may be seen, including peripheral atypical pigment network, erythema, vascular structures, central red-bluish homogeneous area and chrysalis.[3] Recently, Ferrari et al. described a group of atypical "non DF like" patterns, including melanoma-like, vascular tumour-like, basal cell carcinoma-like, collision tumour-like and psoriasis-like.[4] Increased collagen within the papillary dermis of a DF with intense fibrosis corresponds to the white scar-like patch or bright white areas, under nonpolarized or polarized light, respectively. The presence of collagen around the widened rete ridges relates to the white network. Peripheral delicate network correlates to long and hyperpigmented rete ridges with accumulation of melanin in basal keratinocytes due to inflammation.[2,5]
In our case, clinical and dermoscopic features were highly suspicious of melanoma and the definite diagnosis could only be made by histopathological examination. According to Ferrari et al. a significant association was found between atypical, melanoma-like dermoscopic pattern of DF and the hemosyderotic / aneurysmal histopathological subtype.[4] Most hemosiderotic or aneurysmal DFs have a multicomponent dermoscopic pattern, including a central bluish or reddish homogenous areas that according to Zaballos et al. were seen in all the histopathologically diagnosed cases.[2,6] The most probable histologic correlate of this structure are the blood-filled spaces, and intra-and-extracellular hemosiderin deposits. Also seen in our patient, the chrysalis represent dermal collagen, and the blotches or "ring-like globules" may correlate with the flattened and hyperpigmented rete ridges.[6-8]
Some dermatopathologists consider hemosiderotic DF is probably a precursor in the development of aneurysmal DF. This early stage may result from slow extravasation of small amounts of blood from capillaries, leading to the production of hemosyderin within the tumour that will be phagocytized by its cells.[9] The dynamics of hemosiderotic and aneurysmal variants might explain its atypical presentation and some of the many morphological faces of DFs. They are dependent of the evolutive stages and histopathological subtypes of this tumour, hence not always reproducible.[4,10]
Conclusions
We reported additional clinical and dermoscopic features of this relatively rare subtype of DF. Because of its polymorphic and atypical dermoscopic, melanoma-like pattern, a complete excision is advised. Histopathologic examination confirms its benign nature.
References
- Arpaia N, Cassano N, Vena GA. Dermoscopic patterns of dermatofibroma. Dermatol Surg. 2005;31:1336–1339. doi: 10.1111/j.1524-4725.2005.31215. [DOI] [PubMed] [Google Scholar]
- Agero AL, Taliercio S, Dusza SW, Salaro C, Chu P, Marghoob AA. Conventional and polarized dermoscopy features of dermatofibroma. Arch Dermatol. 2006;142:1431–1437. doi: 10.1001/archderm.142.11.1431. [DOI] [PubMed] [Google Scholar]
- Zaballos P, Puig S, Llambrich A, Malvehy J. Dermoscopy of dermatofibromas: a prospective morphological study of 412 cases. Arch Dermatol. 2008;144:75–83. doi: 10.1001/archdermatol.2007.8. [DOI] [PubMed] [Google Scholar]
- Ferrari A, Argenziano G, Buccini P, Cota C, Sperduti I, De Simone P, Eibenschultz L, Silipo V, Zlaudek I, Catricalà C. Typical and atypical dermoscopic presentations of dermatofibroma. J Eur Acad Dermatol Venereol. 2013;27:1375–1380. doi: 10.1111/jdv.12019. [DOI] [PubMed] [Google Scholar]
- Kilinc Karaarslan I, Gencoglan G, Akalin T, Ozdemir F. Different dermoscopic faces of dermatofibromas. J Am Acad Dermatol. 2007;57:401–406. doi: 10.1016/j.jaad.2006.10.984. [DOI] [PubMed] [Google Scholar]
- Zaballos P, Llambrich A, Ara M, Olazarán Z, Malvehy J, Puig S. Dermoscopic findings of hemosiderotic and aneurysmal dermatofibroma: report of six patients. Br J Dermatol. 2006;154:244–250. doi: 10.1111/j.1365-2133.2005.06844.x. [DOI] [PubMed] [Google Scholar]
- Cardoso R, Massone C, Soyer HP, Hofmann-Wellenhof R. Additional dermoscopic presentation of hemosiderotic dermatofibroma. Br J Dermatol. 2007;156:199–200. doi: 10.1111/j.1365-2133.2006.07611.x. [DOI] [PubMed] [Google Scholar]
- Roldán-Marín R, Barreiro-Capurro A, García-Herrera A, Puig S, Alarcón-Salazar I, Carrera C, Malvehy J. Green colour as a novel dermoscopic finding in the diagnosis of hemosiderotic dermatofibroma. Australas J Dermatol. 2014;55:196–197. doi: 10.1111/ajd.12076. [DOI] [PubMed] [Google Scholar]
- Scalvenzi M, Balato A, De Natale F, Francia MG, Mignogna C, De Rosa G. Hemosiderotic dermatofibroma: report of one case. Dermatology. 2007;214:82–84. doi: 10.1159/000096918. [DOI] [PubMed] [Google Scholar]
- Alves JW, Matos DM, Barreiros H, Bártolo AE. Variants of dermatofibroma – a histopathological study. An Bras Dermatol. 2014;89:472–477. doi: 10.1590/abd1806-4841.20142629. [DOI] [PMC free article] [PubMed] [Google Scholar]