

Abstract
Background:
Obesity and hypertension among school children have a huge impact on public health. Hence, we estimated the prevalence and sociodemographic correlates of childhood obesity and elevated blood pressure (BP) among adolescent schoolchildren (11-19 years) in urban areas of Gangtok, Sikkim, India.
Materials and Methods:
A population based cross-sectional study was conducted on 979 school children, during November 1, 2009 - April 30, 2010 in Gangtok, East Sikkim India. Anthropometric measurements and BP were recorded among the study population. Obesity and hypertension prevalent among adolescent school children and their correlates were analyzed.
Results and Conclusion:
Prevalence of obesity, overweight, and hypertension was 2.04%, 14.5% and 5.62%, respectively. The average fast food intake, screen time and limited outdoor activities were significantly associated with obesity. Increase in abdominal height positively correlated with increase in body mass index and body fat; however waist — hip ratio was not a reliable index. The burden of overweight/obesity as well as hypertension with all its associated risk was found to high among our study population, which necessitates framing of policies and actions at national level to address the risk associated with these noncommunicable diseases.
Keywords: Body mass index, hypertension, obesity
INTRODUCTION
Childhood obesity is evolving as a major public health problem, which increases the risk of subsequent morbidity[1,2] as a consequence to hypertension, type 2 diabetes mellitus, dyslipidemia, left ventricular hypertrophy, nonalcoholic steatohepatitis, obstructive sleep apnea, and orthopedic and psychosocial problems.[3,4,5,6] Studies on urban Indian schoolchildren from selected regions report a high prevalence of obesity among children's.[7,8,9,10,11] In addition, the prevalence of hypertension in overweight children is significantly higher compared to normal weight children.[12,13,14] Childhood obesity is frequently undiagnosed and currently nationally representative data are not available in India, which makes initiating any necessary future actions difficult,. Hence, this study was undertaken to determine the prevalence and sociodemographic correlates of childhood obesity and elevated blood pressure (BP) in a representative sample of school children (11-19 years) from the city of Gangtok, Sikkim, India.
MATERIALS AND METHODS
A population-based cross-sectional study was conducted during November 1, 2009-April 30, 2010 among 979 school children 11-19 years from the urban schools of Gangtok. The sample was calculated considering 29% prevalence of obesity in Urban Indian school children[15] with a relative error of 10%. The sample was selected using stratified random sampling from four out of ten senior secondary schools. All senior secondary schools including Government schools, medium-fee structured schools and high fee structured schools listed with the education department of Government of Sikkim were numbered, and four of them selected randomly. 245 students were selected from each schools starting from standard VII upwards, and every 3rd roll numbers were selected for the study. Anthropometric measurements and BP were recorded. Institution ethics committee of Sikkim Manipal Institute of Medical Sciences Gangtok approved the project. The students present on the day of the visit were included in the study. Those children whose obesity or hypertension was secondary to some known disease identity or as a consequence of any medication or under treatment of these two morbidities were excluded from the study.
The main outcome measures were obesity and hypertension prevalent among adolescent schoolchildren and their socioeconomic correlates. The data collection tool used for the study was an interview schedule that was developed at the Institute with the assistance from the faculty members and other experts. By initial translation, back-translation, re-translation followed by pilot study carried out at the outpatients department of the institute among comparable subjects, the schedule was custom-made for the study. All concerned Principals, teachers and students were briefed about the study. They were explained about the purpose of the study and were assured strict confidentiality, and Informed consent was obtained from each of the participants before the total procedure. The participants were given the options not to participate in the study if they wanted. Data regarding family and personal characteristics were recorded by personal interview by the principal investigator body mass index (BMI), and body fat was estimated by a noninvasive technique using body fat Monitor Model-306, OMRON. It was crosschecked by estimating the weight and height and subsequently BP were monitored using standard techniques.
Overweight and obesity were defined by BMI for gender and age. Gender, age and height were considered for determining the hypertension. Children with a BMI >85th percentile of reference data were considered overweight, and those with a BMI >95th percentile was considered obese.[16] The reference data used to identify the cut-off points were taken from the Centers for Disease Control 2000 dataset for BMI[16] BMI cut-off for Asians were also considered.[17] Average systolic or diastolic BP >95th percentile for gender, age and height was considered as hypertensive, whereas >90th percentile, but <95th percentile were considered as prehypertensive.[18]
Statistical analysis
The data collected are presented as % incidence or mean ± standard deviation the data association and difference in means were analyzed using Chi-square test and one-way ANOVA, respectively. P < 0.05 was considered to be significant.
RESULTS
Among 979 study subjects, majority were in the late adolescent age group (62.82%) and females (61.59%). As per WHO criteria, around 2.04% of study subjects were obese while 14.5% were overweight. Considering Asian standards the prevalence of obesity was found to be 3.78% while overweight was 24.31%. In regard to BP, 5.62% were hypertensive, and around 24.11% were in pre-hypertensive zone. Majority of those having prehypertension (49.58%) and hypertension (45.45%) were overweight. Obesity (50%) and overweight (54.22%) were also higher among upper socioeconomic class. Increased BMI was significantly associated with age, sex, status of increased BP and socioeconomic status [Table 1]. Average fast food intake, average screen time and limited outdoor activities, abdominal height, waist-hip ratio and body fat were found to be risk factors for obesity and overweight when compared to normal weight individuals. Association between increased BMI with fast food, screen time, physical activities, abdominal height and body fat were statistically significant. However, waist hip ratio did not statistically correlate with obesity and overweight [Table 2].
Table 1.
Prevalence of obesity and overweight and its correlates
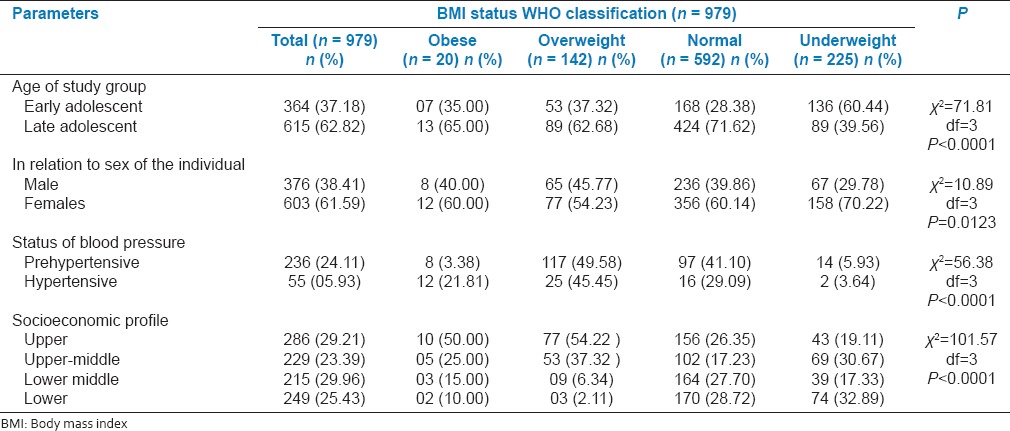
Table 2.
Risk factors associated with overweight and obesity

DISCUSSION
We conducted a cross-sectional study to determine the magnitude of childhood obesity, overweighted and hypertension in a representative population of schoolchildren from Sikkim, India. The risk factors of adolescent obesity and hypertension were explored.
Reports from various parts of India suggest significant heterogeneity in the distribution of childhood obesity prevalence rates.[7,8,9,10] A higher prevalence of obesity and overweight is reported among boys as compared to girls (12.4% vs. 9.9%, 15.7% vs. 12.9%); however, the prevalence of obesity is reported to decrease[7] as well increase with age.[8] In a recent study schoolchildren aged 5-16 years showed a progressive increase in overweight children's indicating a time trend of this rapidly growing epidemic.[19] Our observation of the correlation between obesity and hypertension is consistent with previous other reports.[11,20,21,22,23,24,25,26,27,28,29] Nevertheless, the prevalence of overweight and obesity is reported to be higher among boys than in girls.[30] Essential hypertension commonly recognized in adolescents is of multifactorial origin and has an early onset.[31] A positive linear relationship is reported between systolic and diastolic BP, and the BMI Z score.[8,21,24,25,27,30,31] The increased prevalence of prehypertension and hypertension among overweight and obese children compared to their nonoverweight counterparts is a significant cause for concern.[32] Overweight, as well as obesity, is positively correlated with less physical activity and higher socioeconomic group.[8] This is further enhanced by higher average fast food intakes and screen time.)[37,39,38,40,41] Upper and upper-middle social status contributed to a higher number of obese/overweight and hypertensive children and is previously shown to be a significant risk factor.[25,26,29,33,34,35,36,37,39,42] A significant number of school children's spent 1-4 h/day viewing TV or sitting at the computer.[28] Percentage body fat was highly correlated with BMI among boys and girls over 9 years although no significant difference was observed among the age group of 7-8 years.[43] Higher velocity of BMI and body fat percent were also observed during the pubertal period.[44] Body mass, BMI, skin folds and %fat were significantly (P < 0.001) higher for the sample of obese boys when compared with their nonobese counterparts.[45]
CONCLUSION
The burden of overweight/obesity and hypertension was found to be high among the study population. The high burden of the problem along with all its associated risk among the vulnerable group should act as an eye-opener for further research and framing of policies at national level to curtail the risk of noncommunicable diseases.
ACKNOWLEDGMENTS
We acknowledge co-operation of Principals, teachers and the participants of the study in undertaking the project.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Geneva: World Health Organization; 2005. World Health Organization. Preventing Chronic Diseases: A Vital Investment. World Global Report; p. 23. [Google Scholar]
- 2.Must A, Jacques PF, Dallal GE, Bajema CJ, Dietz WH. Long-term morbidity and mortality of overweight adolescents. A follow-up of the Harvard Growth Study of 1922-1935. N Engl J Med. 1992;327:1350–5. doi: 10.1056/NEJM199211053271904. [DOI] [PubMed] [Google Scholar]
- 3.Barlow SE, Dietz WH. Obesity evaluation and treatment: Expert Committee recommendations. The Maternal and Child Health Bureau, Health Resources and Services Administration and the Department of Health and Human Services. Pediatrics. 1998;102:E29. doi: 10.1542/peds.102.3.e29. [DOI] [PubMed] [Google Scholar]
- 4.Nanda K. Non-alcoholic steatohepatitis in children. Pediatr Transplant. 2004;8:613–8. doi: 10.1111/j.1399-3046.2004.00241.x. [DOI] [PubMed] [Google Scholar]
- 5.Li X, Li S, Ulusoy E, Chen W, Srinivasan SR, Berenson GS. Childhood adiposity as a predictor of cardiac mass in adulthood: The Bogalusa Heart Study. Circulation. 2004;110:3488–92. doi: 10.1161/01.CIR.0000149713.48317.27. [DOI] [PubMed] [Google Scholar]
- 6.Li S, Chen W, Srinivasan SR, Berenson GS. Childhood blood pressure as a predictor of arterial stiffness in young adults: The bogalusa heart study. Hypertension. 2004;43:541–6. doi: 10.1161/01.HYP.0000115922.98155.23. [DOI] [PubMed] [Google Scholar]
- 7.Chhatwal J, Verma M, Riar SK. Obesity among pre-adolescent and adolescents of a developing country (India) Asia Pac J Clin Nutr. 2004;13:231–5. [PubMed] [Google Scholar]
- 8.Ramachandran A, Snehalatha C, Vinitha R, Thayyil M, Kumar CK, Sheeba L, et al. Prevalence of overweight in urban Indian adolescent school children. Diabetes Res Clin Pract. 2002;57:185–90. doi: 10.1016/s0168-8227(02)00056-6. [DOI] [PubMed] [Google Scholar]
- 9.Marwaha RK, Tandon N, Singh Y, Aggarwal R, Grewal K, Mani K. A study of growth parameters and prevalence of overweight and obesity in school children from delhi. Indian Pediatr. 2006;43:943–52. [PubMed] [Google Scholar]
- 10.Khadilkar VV, Khadilkar AV. Prevalence of obesity in affluent school boys in Pune. Indian Pediatr. 2004;41:857–8. [PubMed] [Google Scholar]
- 11.Kapil U, Singh P, Pathak P, Dwivedi SN, Bhasin S. Prevalence of obesity amongst affluent adolescent school children in delhi. Indian Pediatr. 2002;39:449–52. [PubMed] [Google Scholar]
- 12.Verma M, Chhatwal J, George SM. Obesity and hypertension in children. Indian Pediatr. 1994;31:1065–9. [PubMed] [Google Scholar]
- 13.Mohan B, Kumar N, Aslam N, Rangbulla A, Kumbkarni S, Sood NK, et al. Prevalence of sustained hypertension and obesity in urban and rural school going children in Ludhiana. Indian Heart J. 2004;56:310–4. [PubMed] [Google Scholar]
- 14.Anand NK, Tandon L. Prevalence of hypertension in schoolgoing children. Indian Pediatr. 1996;33:377–81. [PubMed] [Google Scholar]
- 15.29 per cent urban school children obese: Study. Statesman News Service. The Sunday Statesman New Delhi. [Last accessed on 2009 Oct 29]. Available from: http://www.worlddiabetesfoundation.org/composite-1220.htm .
- 16.Department of Health and Human Services. Centers for Disease Control and Prevention, USA. CDC Growth Charts for the United States. [Last accessed on 2007 Jan 12]. Available from: http://www.cdc.gov/nchs/data/nhanes/growthcharts/zscore/bmiagerev.xls .
- 17.Australia: IASO and IOTF; 2000. The International Association for the Study of Obesity and the International Obesity Task Force. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment. [Google Scholar]
- 18.National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114(2):555–76. Suppl 4 th Report. [PubMed] [Google Scholar]
- 19.Raj M. Obesity and cardiovascular risk in children and adolescents. Indian J Endocrinol Metab. 2012;16:13–9. doi: 10.4103/2230-8210.91176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zeberio N, Malpeli A, Apezteguía M, Carballo MA, González HF. Nutritional status of school-aged children and its relation to blood pressure. Arch Argent Pediatr. 2013;111:92–7. doi: 10.5546/aap.2013.eng.92. [DOI] [PubMed] [Google Scholar]
- 21.Schwiebbe L, Talma H, Renders C, Visser R, Kist-van Holthe JE, Hirasing RA. High prevalence of hypertension in obese children in the Caribbean. Paediatr Int Child Health. 2012;32:204–7. doi: 10.1179/2046905511Y.0000000011. [DOI] [PubMed] [Google Scholar]
- 22.Deoke A, Hajare S, Saoji A. Prevalence of overweight in high school students with special reference to cardiovascular efficiency. Glob J Health Sci. 2012;4:147–52. doi: 10.5539/gjhs.v4n2p147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Menghetti E, Musacchio P, Tawill L, Vicini S, Spagnolo A. Obesity and arterial hypertension in children: Current calamity. Clin Ter. 2012;163:e107–10. [PubMed] [Google Scholar]
- 24.Hong B, Jin XJ, Su YL, Xiao L, Cai QF, Zou HF, et al. Epidemiological survey on pre-hypertension and hypertension prevalence among adolescents aged 11-17 years in Shanghai. Zhonghua Xin Xue Guan Bing Za Zhi. 2012;40:427–31. [PubMed] [Google Scholar]
- 25.Oduwole AA, Ladapo TA, Fajolu IB, Ekure EN, Adeniyi OF. Obesity and elevated blood pressure among adolescents in Lagos, Nigeria: A cross-sectional study. BMC Public Health. 2012;12:616. doi: 10.1186/1471-2458-12-616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chakraborty P, Dey S, Pal R, Kar S, Zaman FA, Pal S. Obesity in Kolkata children: Magnitude in relationship to hypertension. J Nat Sci Biol Med. 2011;2:101–6. doi: 10.4103/0976-9668.82310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Rao S, Kanade A, Kelkar R. Blood pressure among overweight adolescents from urban school children in Pune, India. Eur J Clin Nutr. 2007;61:633–41. doi: 10.1038/sj.ejcn.1602555. [DOI] [PubMed] [Google Scholar]
- 28.Aggarwal T, Bhatia RC, Singh D, Sobti PC. Prevalence of obesity and overweight in affluent adolescents from Ludhiana, Punjab. Indian Pediatr. 2008;45:500–2. [PubMed] [Google Scholar]
- 29.Jain S, Pant B, Chopra H, Tiwari R. Obesity among adolescents of affluent public schools in Meerut. Indian J Public Health. 2010;54:158–60. doi: 10.4103/0019-557X.75740. [DOI] [PubMed] [Google Scholar]
- 30.Khadilkar V, Khadilkar A. Growth charts: A diagnostic tool. Indian J Endocrinol Metab. 2011;15(Suppl 3):S166–71. doi: 10.4103/2230-8210.84854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Raj M. Essential hypertension in adolescents and children: Recent advances in causative mechanisms. Indian J Endocrinol Metab. 2011;15(Suppl 4):S367–73. doi: 10.4103/2230-8210.86981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rahman AJ, Qamar FN, Ashraf S, Khowaja ZA, Tariq SB, Naeem H. Prevalence of hypertension in healthy school children in Pakistan and its relationship with body mass index, proteinuria and hematuria. Saudi J Kidney Dis Transpl. 2013;24:408–12. doi: 10.4103/1319-2442.109619. [DOI] [PubMed] [Google Scholar]
- 33.Lu X, Shi P, Luo CY, Zhou YF, Yu HT, Guo CY, et al. Prevalence of hypertension in overweight and obese children from a large school-based population in Shanghai, China. BMC Public Health. 2013;13:24. doi: 10.1186/1471-2458-13-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Babinska K, Kovacs L, Janko V, Dallos T, Feber J. Association between obesity and the severity of ambulatory hypertension in children and adolescents. J Am Soc Hypertens. 2012;6:356–63. doi: 10.1016/j.jash.2012.08.002. [DOI] [PubMed] [Google Scholar]
- 35.Xu YJ, Li M, Xu PR, Zheng YS, Zhang L, Ye MG, et al. Correlation between obesity index and blood pressure in Kazak childhood from Yili, Xinjiang. Zhonghua Liu Xing Bing Xue Za Zhi. 2012;33:774–8. [PubMed] [Google Scholar]
- 36.Buch N, Goyal JP, Kumar N, Parmar I, Shah VB, Charan J. Prevalence of hypertension in school going children of Surat city, Western India. J Cardiovasc Dis Res. 2011;2:228–32. doi: 10.4103/0975-3583.89807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Gupta AK, Ahmad AJ. Childhood obesity and hypertension. Indian Pediatr. 1990;27:333–7. [PubMed] [Google Scholar]
- 38.Maher C, Olds TS, Eisenmann JC, Dollman J. Screen time is more strongly associated than physical activity with overweight and obesity in 9- to 16-year-old Australians. Acta Paediatr. 2012;101:1170–4. doi: 10.1111/j.1651-2227.2012.02804.x. [DOI] [PubMed] [Google Scholar]
- 39.Musaiger AO, Al-Mannai M, Zagzoog N. Association between food intake frequency and obesity among adolescent girls in Saudi Arabia. Int J Adolesc Med Health. 2014;26:145–7. doi: 10.1515/ijamh-2012-0115. [DOI] [PubMed] [Google Scholar]
- 40.Fraser LK, Clarke GP, Cade JE, Edwards KL. Fast food and obesity: A spatial analysis in a large United Kingdom population of children aged 13-15. Am J Prev Med. 2012;42:e77–85. doi: 10.1016/j.amepre.2012.02.007. [DOI] [PubMed] [Google Scholar]
- 41.Shan XY, Xi B, Cheng H, Hou DQ, Wang Y, Mi J. Prevalence and behavioral risk factors of overweight and obesity among children aged 2-18 in Beijing, China. Int J Pediatr Obes. 2010;5:383–9. doi: 10.3109/17477160903572001. [DOI] [PubMed] [Google Scholar]
- 42.Wang Y, Lim H. The global childhood obesity epidemic and the association between socio-economic status and childhood obesity. Int Rev Psychiatry. 2012;24:176–88. doi: 10.3109/09540261.2012.688195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Khadgawat R, Marwaha RK, Tandon N, Mehan N, Upadhyay AD, Sastry A, et al. Percentage body fat in apparently healthy school children from northern India. Indian Pediatr. 2013;50:859–66. doi: 10.1007/s13312-013-0237-3. [DOI] [PubMed] [Google Scholar]
- 44.Sood A, Sundararaj P, Sharma S, Kurpad AV, Muthayya S. BMI and body fat percent: Affluent adolescent girls in Bangalore City. Indian Pediatr. 2007;44:587–91. [PubMed] [Google Scholar]
- 45.Chatterjee S, Chatterjee P, Bandyopadhyay A. Skinfold thickness, body fat percentage and body mass index in obese and non-obese Indian boys. Asia Pac J Clin Nutr. 2006;15:231–5. [PubMed] [Google Scholar]