

Abstract
Acquired immunodeficiency syndrome (AIDS)-associated Kaposi's sarcoma (KS) occurs with increased frequency in all HIV transmission groups and at a particularly high rate among homosexual men. It usually presents initially as violaceous cutaneous lesions, but oral mucosa, lymph nodes and visceral organs may be affected, sometimes without skin involvement. KS in a 20-year-old HIV-seropositive patient with oral involvement as the sole presentation of the disease is presented herewith; thus contributing a new AIDS-related KS case reported in Indian Literature.
Keywords: Acquired immunodeficiency syndrome, HIV, Kaposi's sarcoma, oral, palate
INTRODUCTION
Kaposi's Sarcoma (KS), being first described in 1872,[1] is an unusual vascular neoplasm that most likely arises from endothelial cells, with some evidence of lymphatic origin. Among the various clinical forms of KS recognized, acquired immunodeficiency syndrome (AIDS)-associated KS is the most aggressive form; with the vast majority of the patients discovered to date have been HIV-1 infected homosexual men,[2] although a few heterosexual males and females have been afflicted as well.
Lesions of KS typically manifests as bluish-purple macules and plaques on the skin, particularly of the face and lower extremities. Oral mucosa, lymph nodes and visceral organs may be affected, sometimes without cutaneous involvement. Although any mucosal site may be involved; the hard palate, gingiva and tongue are affected most frequently.[3] Of significance is that, oral lesion may be the initial site of involvement (nearly 20-25% cases) or the only site or the first indication of HIV infection.
This paper reviews one such case of KS in a 20-year-old HIV-seropositive female patient with oral involvement as the sole presentation of the disease.
CASE REPORT
A 20-year-old married HIV-seropositive woman was referred to our service for the evaluation of a painless swelling on the hard palate that had appeared 2 months earlier, with the rapid evolution. The patient informed the deferment of antiretroviral therapy for 4 months. Extra-oral examination revealed no significant findings with respect to area in question. Palpable cervical lymphadenopathy was present; with the lymph nodes being firm and non-tender on palpation [Figure 1a].
Figure 1.
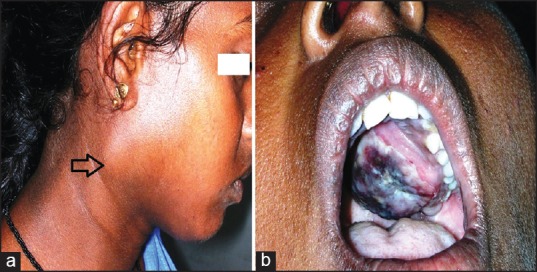
(a) Extra-oral view depicting cervical lymphadenopathy (arrow head) (b) Bluish-red nodular enlargement of the left hard palate
On Intra-oral examination, diffuse bluish-red nodular enlargement on the left side of the hard palate was verified, extending anteriorly from the left maxillary canine to the tuberosity region posteriorly. The nodular enlargement was observed crossing the midline, involving almost the entire hard palate and protruding at the level of the occlusal plane, thus interfering with the mastication. On palpation, the swelling was firm in consistency; non-tender and exhibited surface ulceration [Figure 1b]. None of the regional teeth exhibited mobility. Panoramic radiograph revealed no significant changes in the adjacent bone. No other similar lesions in any other region of the body were detected. In view of the history and clinical findings, a diagnostic possibility of KS was hypothesized with differential diagnosis of bacillary angiomatosis and lymphoma.
Subsequently, an incisional biopsy was performed and the specimen was submitted for the histopathological examination. Light microscopic examination of the sections stained with hematoxylin and eosin revealed fibrous connective tissue stroma with numerous irregular slit like spaces containing extravasated red blood cells and surrounded by ill-defined fascicles of spindle shaped cells [Figure 2]. Chronic inflammatory cell infiltrate was evident beneath the surface epithelium. The histopathological features confirmed the clinical diagnosis of KS.
Figure 2.
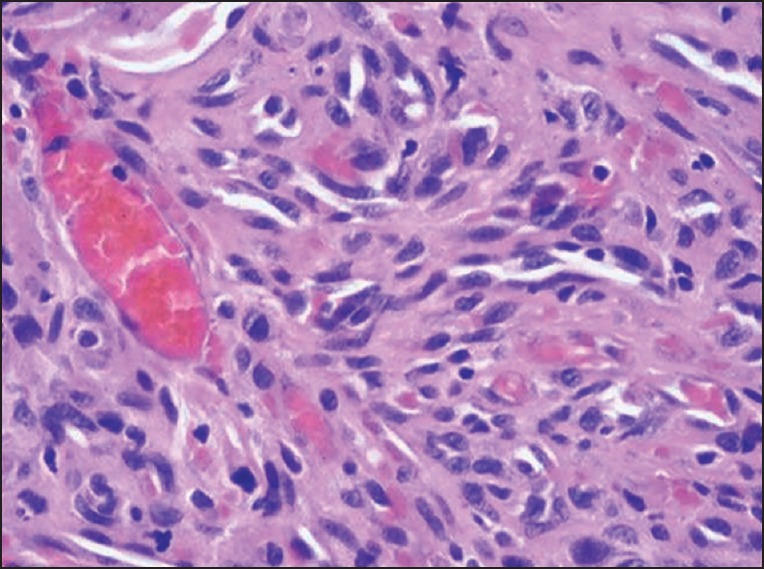
Photomicrograph of the histopathologic section reveals fibrous connective tissue stroma with numerous irregular slit like spaces containing extravasated red blood cells and surrounded by ill-defined fascicles of spindle shaped cells (H-E)
Further to rule out distant metastasis, chest radiography [Figure 3] and ultrasonography of the abdomen were performed that revealed no pathology. The patient was classified as a good risk according to the staging classification system for AIDS-related KS proposed by the AIDS Clinical Trial Group.[4] The patient was referred to the medical oncologist for the completion of the treatment. The oncologist suggested the re-establishment of highly active antiretroviral treatment (HAART) in order to control the progression of KS and to allow Immune restoration, since the suppression of viral replication and restoration of immunity by HAART has been effective in tumor control in most patients considered to have a good prognosis. After that unfortunately, we lost communication with the patient for follow-up.
Figure 3.
Chest radiograph
DISCUSSION
Before the advent of AIDS epidemic, KS was considered as a rare tumor. However, since the early 1980's, it has become quite common because of its propensity to develop in HIV infected individuals. In fact, the mere presence of KS lesions in HIV-seropositive subjects constitutes a diagnostic sign for AIDS. Early oral KS is represented by flat reddish purple discoloration and as the disease progresses; the later stage is characterized by nodular appearance with or without secondary ulceration;[3] as observed in the present case.
The etiology of the disease is unknown, but the condition is considered by most workers to be neoplastic in nature; while other theories have proposed KS representing reticuloendothelial hyperplasia. Current evidence suggests that KS is caused by human herpes virus 8 (HHV-8). The course of the disease is strongly influenced by the immune status of the patient.
To the best of our knowledge, of the 13 cases of AIDS-related KS described in the literature from India; 12 cases were reported in males.[5] In terms of clinical presentation of the disease; 8/13 reported cases manifested cutaneous and mucous membrane involvement while 5 cases presented with only cutaneous lesions. The present case is unique as the patient had oral KS, without the evidence of any cutaneous involvement.
Clinically KS strongly resembles certain vascular lesions that include ecchymosis or a deeply located low grade mucoepidermoid carcinoma (at initial stages); or these appear more like hemangiomas, lymphangiomas and arteriovenous hemangiomas (at papular or nodular stage). Even though uncommon, bacillary angiomatosis may appear as multifocal KS lesions. When present on the alveolar ridge, they may resemble pyogenic granuloma or peripheral giant cell proliferation.[6] A biopsy is, therefore, necessary to ascertain an accurate diagnosis.
Microscopically, from the differential diagnostic point of view, pathologies such as well-differentiated angiosarcoma (early KS lesion), fibrosarcoma (advanced KS lesion), arteriovenous malformations, Kaposiform hemangioendothelioma, spindle cell hemangioendothelioma and bacillary angiomatosis, should be included.[6,7] Careful histologic sampling reveals other characteristic components of these pathological entities; thus allows for appropriate diagnosis. Further, an accurate clinical history becomes of paramount importance for establishing the diagnosis of KS and thus distinguishing it from other lesions.
The prognosis is variable depending upon the form of the disease and the patient's immune status. KS is a progressive malignancy that may disseminate widely into lymph nodes and various organ systems. Extensive systemic therapy often further depresses the immune system, therefore, increasing the patient's susceptibility to infections and other neoplasms. Achievement of permanent cure has been elusive, although most patients of AIDS-associated KS die of other complications such as opportunistic infections. The introduction of HAART has greatly influenced the pattern of KS incidence in people with HIV. However it is not known if the improvement in the clinical course of HIV-KS response is due to an improvement in the host-immune status or a direct antiviral effect against HHV-8.
It is evident that in the majority of subjects who are HIV-seropositive with KS, effective HAART decreases the incidence and the prevalence of KS and causes regression of established lesions. But deferment of the antiretroviral therapy by the patient, in the present case culminated with the appearance and rapid evolution of the nodular lesion in the oral cavity.
CONCLUSION
The present case of KS in HIV-seropositive female, manifesting as palatal nodular enlargement without any cutaneous and visceral involvement, is first of its kind reported in the Indian Literature. Since the patients with oral KS may have a higher mortality rate than those with only cutaneous manifestations; prompt diagnosis is of paramount importance contributing to a good prognosis and better survival.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Kaposi M. Idiopanthisches multiples Pigmentsarkom der Haut. Arch Dermatol Syph. 1872;4:265–76. [Google Scholar]
- 2.Barnes L, Eveson JW, Reichart P, Sidransky D. Lyon: IARC Press; 2005. World Health Organization Classification of Tumors. Pathology and Genetics of Head and Neck Tumors; pp. 193–4. [Google Scholar]
- 3.Neville BW, Damm DD, Allen CM, Bouquot JE. 2nd ed. Philadelphia: Saunders; 2002. Oral & Maxillofacial Pathology. [Google Scholar]
- 4.Krown SE, Metroka C, Wentz JC. Kaposi's sarcoma in the acquired immune deficiency syndrome: A proposal for uniform evaluation, response, and staging criteria. AIDS Clinical Trials Group Oncology Committee. J Clin Oncol. 1989;7:1201–7. doi: 10.1200/JCO.1989.7.9.1201. [DOI] [PubMed] [Google Scholar]
- 5.Joshi U, Ceena DE, Ongole R, Sumanth KN, Boaz K, Jeena Priy K, et al. AIDS related Kaposi's sarcoma presenting with palatal and eyelid nodule. J Assoc Physicians India. 2012;60:50–3. [PubMed] [Google Scholar]
- 6.Marx RE, Stern D. 2nd ed. Chicago: Quintessence Publishing Company; 2012. Oral and Maxillofacial Pathology: A Rationale for Diagnosis and Treatment; pp. 508–12. [Google Scholar]
- 7.Weiss SW, Goldblum JR. 4th ed. Philadelphia: Mosby-Harcourt; 2001. Enzinger and Weiss's Soft Tissue Tumors; pp. 938–47. [Google Scholar]