

Abstract
There are ample modern diagnostic imaging tools available, but the affordability, availability and radiation exposure remains the concern. Intraoral periapical radiographs (IOPAR) are widely used for the preoperative planning and evaluation for most minor oral surgical procedures owing to it simplicity, significantly lower cost, less radiation exposure and easy availability in a dental clinical set-up. Using these radiographs with a grid aids in increasing the accuracy of the linear measurements for the treatment planning.
Keywords: Oral implantology, Dental implants, Intraoral periapical radiographs
Introduction
With current advances in oral implantology and dependability of currently available implant systems, dental implants have become a cornerstone of oral rehabilitation. Pre-surgical radiographic assessment is an important step for preoperative planning in dental implantology. There are ample modern diagnostic imaging tools available [1], but the affordability, availability and radiation exposure remains the concern. Intraoral periapical radiographs (IOPAR) are widely used for the preoperative planning and evaluation for most minor oral surgical procedures owing to it simplicity, significantly lower cost, less radiation exposure and easy availability in a dental clinical set-up [2]. When used, it is critical on the operator’s part to extract maximum information from two dimensional images of IOPARs. Using IOPARs with a grid aids in increasing the accuracy of the linear measurements for the treatment planning.
Gridded Intra-Oral Periapical Radiographs
A radio-opaque metal mesh or a grid can be placed between the object/structures to be imaged and the radiographic film/sensor at the time of x-ray exposure. The two adjacent parallel lines of the grid used should be equidistant. The linear distances in two dimensions can be measured for pre-surgical planning using the following mathematical formula:
 |
To find a linear distance on the gridded IOPAR, the actual known distance between two points on the grid divided by the distance measured between similar points on the grid lines on the radiograph can be equated to the actual unknown distance between the two anatomic points in question (e.g., crest of alveolar ridge to the superior cortex of the inferior alveolar canal) divided by the measured distance between those two anatomic points on the radiographic image.
Figure 1 shows an IOPAR taken with a grid with the actual linear calculated distance between the crest of alveolar ridge to the superior cortex of the inferior alveolar canal being 15.4 mm. This distance for the same patient was assessed on a cone beam computed tomography (CBCT) scan, and was found to be 15.6 mm (Fig. 2) demonstrating 98.7 % accuracy of the linear distance measured on a two dimensional image of a gridded IOPAR. Post-dental implant placement, the patient was re-assessed (Fig. 3). Although, these accuracy rates may vary in a larger clinical trial, IOPAR will hold its importance due to its wide availability in a dental clinical setup and minimal radiation exposure. CBCT was used to compare distances measured on the IOPAR as it is reported to provide near accurate tomographic evaluation of distances for dental implants when compared to the conventional plain film radiography [2, 3]. Apart from dental implantology, gridded IOPARs will also be useful and find application in surgeries involving removal of the third molar, procedures involving root resection, endodontics, evaluation of bone grafts and any dental procedure that involves measuring linear dimensions on a radiograph.
Fig. 1.
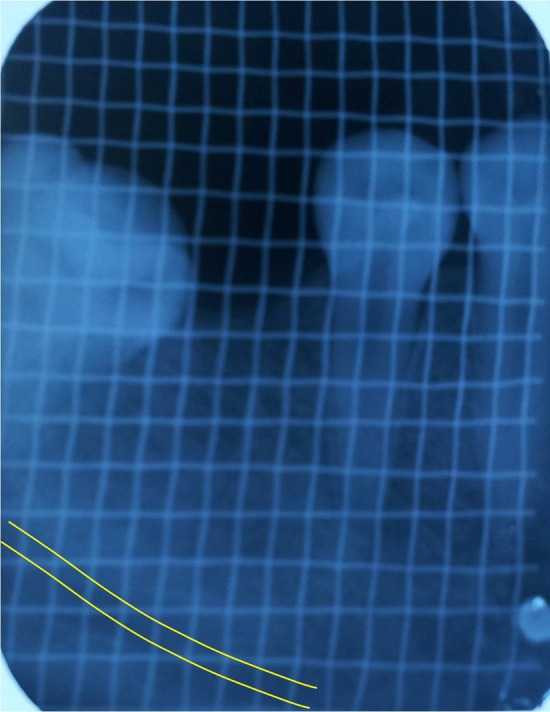
Intra-oral periapical radiographs with grids for pre-operative planning for placing a dental implant in the region of missing 46. Distance calculated from crest of alveolar ridge to the superior cortex of the inferior alveolar canal = 15.4 mm
Fig. 2.
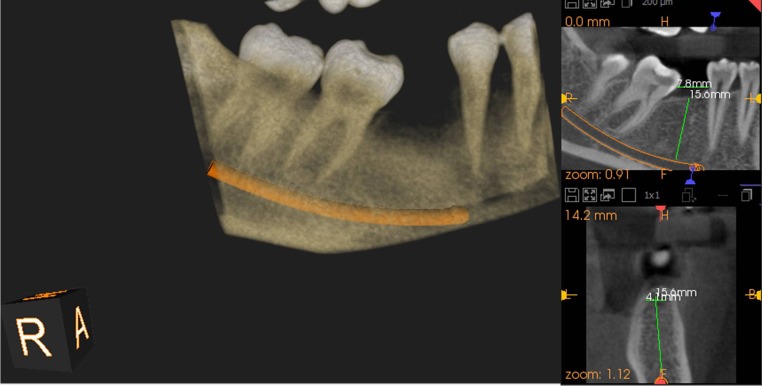
CBCT scan of the same patient showing crest of alveolar ridge to the superior cortex of the inferior alveolar canal distance = 15.6 mm
Fig. 3.
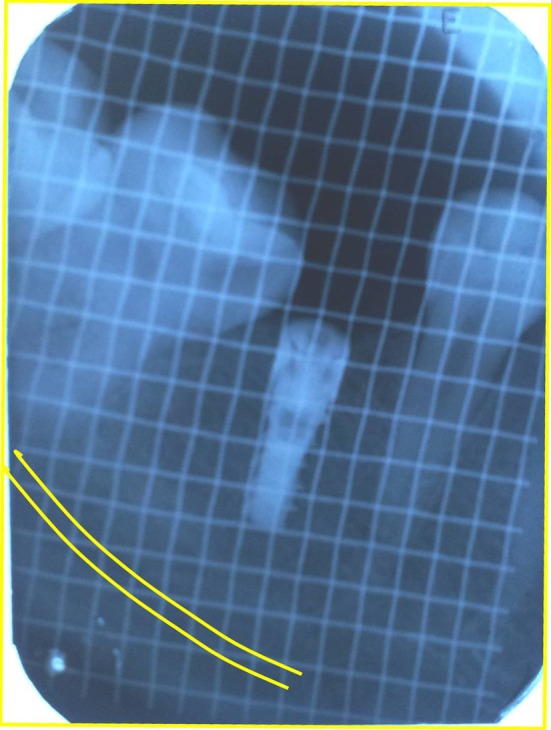
Gridded IOPAR after the surgical placement of the dental implant for post-operative evaluation
Conflict of interest
Authors declare no conflict of interest.
References
- 1.Mupparapu M, Singer SR. Implant imaging for the dentist. J Can Dent Assoc. 2004;70:32. [PubMed] [Google Scholar]
- 2.Bhargava D, Deshpande A, Sreekumar K, Deshpande A. Relationship of mandibular canal to root apices of mandibular molars: accuracy of intraoral periapical radiographs. J Stomat Occ Med. 2011;4:118–122. doi: 10.1007/s12548-011-0017-4. [DOI] [Google Scholar]
- 3.Bassam H. Reliability of periapical radiographs and orthopantomograms in detection of tooth root protrusion in the maxillary sinus: correlation results with cone beam computed tomography. J Oral Maxillofac Res. 2010;1:e6. doi: 10.5037/jomr.2010.1106. [DOI] [PMC free article] [PubMed] [Google Scholar]