

Abstract
Aim
The aim of the present study was to analyze clinical, radiological and histopathological features of aneurysmal bone cysts (ABCs) of jaws.
Materials and Methods
Archival data from 2009 to 2012 present in the Oral Pathology Department was retrieved and clinicopathological features of all the cases which had been previously diagnosed as ABC were analyzed in detail.
Results
Seven cases ranging in age from 10 to 50 years were included, in which maximum (5/7) cases were below 20 years. Ratio of presentation of lesion in male to female and in maxilla to mandible was 3:6 and 1:6 respectively. Swelling and pain were the most common presenting features. Variable presentation of the lesion was observed radiographically; although multilocular, well defined, bone expansion and perforation were the most common observations. Histopathological analysis revealed association of one case with ossifying fibroma and two cases with trabecular variety of juvenile ossifying fibroma. Predominance of solid variety was noted and other features like stroma, giant cells, nature of blood vessels, bone destruction and perforation and presence of any osteoid or calcified material was also accounted for. The current study showed association of two cases with trabecular variety of juvenile ossifying fibroma, which is a rare finding.
Conclusion
ABCs of jaws, thus have varying patterns of presentation which are diagnostically challenging. A thorough examination of the incisional/excisional tissue is thus required to confirm the association with any other lesion which will affect the treatment plan for the patient.
Keywords: Aneurysmal bone cyst, Juvenile ossifying fibroma, Trabecular juvenile ossifying fibroma
Introduction
Aneurysmal bone cyst (ABC) as defined by WHO is an expansile osteolytic lesion consisting of blood filled spaces separated by connective tissue septae that contain osteoid material and multinucleated giant cells [1]. ABCs are relatively rare lesions. Most cases of ABC involve long bones such as femur or tibia and only about 12 % affect the head and neck region of which 2 % occur in jaws [2, 3]. Jaw aneurysmal bone cysts (JABC) occur mainly in the mandible, accounting for about two-thirds of the cases [4].
The etiopathogenesis of ABC is uncertain. Several theories have been put forward like post traumatic, reactive malformation, genetic predisposition, dilatation of local vascular network due to increased venous pressure caused by local circulatory abnormalities. Some researchers have demonstrated that chromosomal translocation t(16;17) (q22;p13) is a cytogenic abnormality which could result in the development of ABCs. They can arise de-novo, when they are known as primary ABC, or in co-existence with other lesions such as ossifying fibroma (OF), chondroblastoma, solitary bone cyst, giant-cell tumor of the bone, osteosarcoma, osteoblastoma, giant cell reparative granuloma, fibrous dysplasia and fibromyxoma when they are secondary in nature [5, 6].
The aim of the present study was to analyze clinical, radiological and histopathological features of seven cases of JABC diagnosed over a period of 3 years. An analysis of the nature, whether primary or secondary was also considered.
Materials and Method
Archival data of the cases which were histopathologically diagnosed as ABC were retrieved from January 2009 to June 2012. Seven cases were selected for which all relevant clinical, radiological and histopathological data was available.
Clinical features of age, sex, site of lesion and the presentation were analyzed along with density, periphery, locularity of the lesion and association with any teeth as visible on the radiographs.
Based on the criteria previously described by Henriques et al. [7], the lesions were divided into solid, mixed and vascular subtype. The following morphological features were analyzed and graded by three oral pathologists:
Stroma
Blood vessels
Giant cells
Osteoid/calcified material
Stroma was described as loose, dense, cellular or highly cellular while blood vessels, giant cells, osteoid/calcified material were quantitatively graded in the following manner:
+ → Few/mild
++ → Intermediate/moderate
+++ → Numerous/severe
++++ → Criteria under observation is the predominant feature
Following observations were made from the surgical findings given by the operating surgeon:
Bone destruction and perforation
Bleeding on surgery
Those lesions having dense connective tissue stroma, few small capillaries and oozing of blood at surgical site with very little bone expansion/perforation were classified as solid subtype. On the other hand, lesions consisting of loose connective tissue stroma, numerous and large blood filled spaces, welling up of blood on surgical opening with extensive bone expansion and perforation were described as vascular subtype. Lesions having features lying in between these two varieties, namely cellular stroma with moderately sized blood filled spaces, were classified as mixed subtype.
The data was tabulated and analyzed in detail.
Results
Of the seven cases studied, four females and three males were affected. Age of the patients ranged from 10 to 50 years (average age being 20.7 years). The pattern of site distribution showed a predominance of posterior mandible (5/7). Swelling was observed in all the cases (Fig. 1) and was associated with pain in two cases (Table 1).
Fig. 1.

a Extraoral view showing swelling over right ramus of mandible (case #6), b intraoral view showing buccal expansion (case #5)
Table 1.
Clinical presentation
| Age (years) | Sex | Site | Symptom | Bony changes | |
|---|---|---|---|---|---|
| 1 | 50 | Male | Right posterior mandible | Swelling | Expansion + perforation |
| 2 | 35 | Male | Right posterior mandible | Swelling | Expansion |
| 3 | 10 | Female | Left anterior maxilla | Swelling | Expansion + resorption of alveolar bone |
| 4 | 13 | Female | Left posterior mandible | Swelling and pain | Expansion |
| 5 | 10 | Male | Left posterior mandible | Swelling | Expansion + resorption of roots + perforation |
| 6 | 14 | Female | Right posterior mandible | Swelling | Expansion |
| 7 | 13 | Female | Right anterior mandible | Swelling and pain | Expansion + perforation |
Radiographically, radiolucent lesion was almost as common as mixed radiolucent-radiopaque appearance. Well-defined multilocular lesions were predominantly observed (Fig. 2). Some other features like association with impacted teeth (2 cases), resorption of roots (1 case) and alveolar bone (1 case) were also observed (Table 2). Ballooning expansion of the cortex was noted in two cases (case #5 and case #7).
Fig. 2.
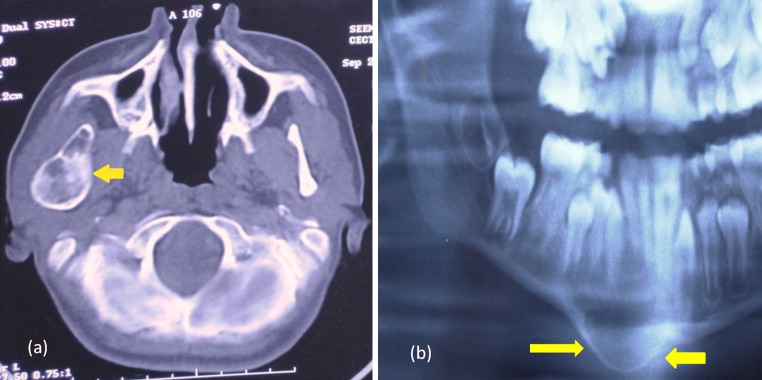
a Computed tomography scan showing radiolucent, multilocular lesion (case #6), b panoramic view showing well defined, unilocular, radiolucent lesion with ballooning expansion of the inferior border of mandible (case #7)
Table 2.
Radiological presentation
| Density | Border | Locularity | Tooth association | |
|---|---|---|---|---|
| 1 | Radiolucent | Well defined | Multilocular | – |
| 2 | Radiolucent | Well defined | Multilocular | – |
| 3 | Mixed | Well defined | Multilocular | – |
| 4 | Mixed | Well defined | Multilocular | Impacted #38 |
| 5 | Mixed | Well defined | Unilocular | – |
| 6 | Radiolucent | Well defined | Multilocular | – |
| 7 | Radiolucent | Well defined | Unilocular | Unerupted 43, 44, 45 |
Histopathologically (Fig. 3), predominance of solid subtype was observed (4/7); two of which were found to be associated with trabecular variety of juvenile ossifying fibroma (TJOF). Only one case was found to be of vascular subtype which was associated with OF. Remaining two cases were of mixed variety (Table 3).
Fig. 3.

a Photomicrograph of solid type ABC showing dense stroma with few small vascular spaces (black arrows), H&E ×100, b photomicrograph of mixed type ABC showing cellular stroma with moderate amount of blood filled spaced and associated giant cells H&E ×100; inset showing multinucleated giant cells X400, c photomicrograph of vascular type ABC showing loose connective tissue stroma with abundant large blood filled spaces, H&E ×100, d photomicrograph of solid ABC with TJOF: highly cellular stroma with abundant immature bone formation (yellow arrows) associated with large blood filled areas (black arrows), H&E ×100, e photomicrograph of vascular ABC with OF: abundant blood filled spaces (black arrows) with ossifying fibroma (yellow arrows), H&E ×100
Table 3.
Histopathological and surgical features
| Histopathlogical findings | Surgical findings | |||||||
|---|---|---|---|---|---|---|---|---|
| Stroma | Nature of blood vessels | Giant cells | Osteoid/calcified material/any other | Bone destruction/perforation | Bleeding on surgery | Final diagnosis and type | ||
| 1 | Dense | Small blood filled spaces + | +++ | – | – | Oozing out blood | ABC (solid) | Primary |
| 2 | Dense | Small blood filled spaces + | – | – | – | Oozing out blood | ABC (solid) | Primary |
| 3 | Very highly cellular with juvenile ossifying fibroma | Blood filled spaces ++ | + 1/2 | +++++ Trabecular juvenile ossifying fibroma |
Present | – | ABC + trabecular juvenile ossifying fibroma (solid) | Secondary |
| 4 | Cellular | Sinusoidal Spaces ++ | ++ | ++ | – | Abundant bleeding | ABC (mixed) | Primary |
| 5 | Loose | Blood filled spaces +++ | + | +++ | Extensive destruction and perforation | Welling up of blood | ABC + ossifying fibroma (vascular) | Secondary |
| 6 | Highly cellular with juvenile ossifying fibroma | Blood filled spaces ++ | + | +++++ Trabecular juvenile ossifying fibroma |
– | – | ABC + trabecular juvenile ossifying fibroma (solid) | Secondary |
| 7 | Cellular | Blood filled spaces ++ | – | ++ | – | Abundant bleeding | ABC (mixed) | Primary |
Discussion
Aneurysmal bone cyst was first described by Jaffe and Lichtenstein in 1942 as blood filled cysts in which tissue from cyst wall contained conspicuous spaces, areas of hemosiderin deposition, giant cells and occasional bone trabeculae [6].
Aneurysmal bone cyst is more common in first three decades with a peak from 10 to 20 years [8]. Sex incidence varies in literature with a tendency towards equal distribution between males and females. The current study also showed similar results compatible with previously reported literature [9, 10]. Mandibular involvement was predominant over maxilla (6:1) with posterior mandible being the most frequent site. Rare occurrence of one case involving anterior maxilla was noted. Clinically evident expansion of the bone was noticed in all cases, with cortical perforation seen as an associated feature. Motamedi and Yazdi has reported a similar description for the vascular type of ABC [3].
Aneurysmal bone cysts have variable radiological appearances and should be considered in the differential diagnosis of any unilocular or multilocular radiolucencies of the jaws and any mixed radiopaque-radiolucent lesion [11]. The current case series also showed an almost equal distribution of mixed radiopaque-radiolucent and only radiolucent appearance with ballooning expansion in two cases.
Histologically, ABCs have been classified into solid, mixed and vascular variants. The present study revealed four cases of solid variety, followed by two cases of mixed type and one case of vascular type. This concurs with Henriques et al. [7] who have reported that the vascular variety was least common as opposed to Vergel et al. [12] who proposed that the vascular variety is the most common.
An important feature of the current study is that four cases were primary in nature and three cases had an associated lesion of OF/TJOF. The cases associated with TJOF were of solid type and that associated with OF was vascular. Such an association with OF of the jaws has been previously reported in literature by Sun et al. [9]; where 64.7 % cases were associated with OF. In secondary ABCs involving long bones, giant cell lesions are the most common associated lesions accounting for 39 % of all secondary lesions [13].
Trabecular variety of juvenile ossifying fibroma is a well established aggressive type of juvenile ossifying fibroma in which ABC formation is relatively rare. Usually, ABC formation is more common in the psammomatoid type [14]. The current study showed two cases of ABC associated with juvenile ossifying fibroma wherein the histopathological appearance was characteristic of TJOF with osteoid seams and highly immature woven bone in highly cellular fibroblastic stroma. These two cases were seen in a younger age group. Hence, the criteria for diagnosing TJOF have to be applied both clinically as well as histopathologically. A thorough search of literature has revealed only three cases of TJOF with ABC published till date [15–17], with another two cases being reported by us recently [18].
Dormans et al. (5), in their study on 52 primary ABCs, found rearrangements of CDH11 and/or USP6 in almost 70 % of the cases. Rearrangements of these genes were found to be restricted to the spindle cells in the walls of the ABCs and were not found in the multinucleated giant cells, inflammatory cells, endothelial cells or osteoblasts. Oliveira et al. [19] also investigated CDH11 and USP6 rearrangements in 17 secondary ABCs but with negative results, indicating that secondary ABCs seemed to represent a nonspecific morphologic pattern in a different group of neoplasms.
Treatment of ABC depends upon the extent of the lesion ranging from simple curettage to surgical resection [9]. In the current series, curettage was the predominant treatment modality followed. Although, one case of ABC with solid TJOF was treated by surgical resection and another was treated by surgical excision.
Recurrence has not been noted after 1.5–2 years of follow up, though literature reveals that recurrence usually occurs within the first year after initial treatment [8].
To conclude, ABC of the jaws can present in varying patterns which are diagnostically challenging as the lesion can be primary or secondary in nature. Thorough histopathological examination of the incisional/excisional tissue will confirm the association of a secondary lesion which needs to be treated accordingly. Further studies on the clonality of the lesion on a large sample size are needed to ascertain its true nature.
Acknowledgments
Conflict of interest
None.
Contributor Information
Aadithya B. Urs, Phone: +91-9582948857, Email: draadithya@sify.com
Jeyaseelan Augustine, Email: j_augustine@rediffmail.com.
Himanshi Chawla, Email: himanshichawla@ymail.com.
References
- 1.Rosenberg AE, Nielson GP, Fletcher JA. Aneurysmal bone cyst. In: Fletcher CDM, Unni KK, Mertens F, editors. WHO classification of tumors: pathology and genetics of tumors of soft tissue and bone. 3. Lyon: IARCPress; 2005. pp. 338–339. [Google Scholar]
- 2.Fennessy BG, Vargas SO, Silveria MV, Ohlms LA, Mcgill TJ, Healy GB, et al. Paediatric aneurysmal bone cysts of the head and neck. J Laryngol Otol. 2009;123:635–641. doi: 10.1017/S002221510800337X. [DOI] [PubMed] [Google Scholar]
- 3.Motamedi MH, Yazdi E. Aneurysmal bone cyst of the jaws: analysis of 11 cases. J Oral Maxillofac Surg. 1994;52:471–475. doi: 10.1016/0278-2391(94)90343-3. [DOI] [PubMed] [Google Scholar]
- 4.Mohammad MH, Navi F, Eshkevari PS, Jafari SM, Shams MG, Taheri M, et al. Variable presentations of aneurysmal bone cysts of the jaws: 51 cases treated during a 30-year period. J Oral Maxillofac Surg. 2008;66:2098–2103. doi: 10.1016/j.joms.2008.05.364. [DOI] [PubMed] [Google Scholar]
- 5.Dormans JP, Hanna BG, Johnston DR, Khurana JS. Surgical treatment and recurrence rate of aneurysmal bone cysts in children. Clin Orthop Relar Res. 2004;421:205–211. doi: 10.1097/01.blo.0000126336.46604.e1. [DOI] [PubMed] [Google Scholar]
- 6.Martinez V, Sissons HA. Aneurysmal bone cyst: a review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer. 1988;61:2291–2304. doi: 10.1002/1097-0142(19880601)61:11<2291::AID-CNCR2820611125>3.0.CO;2-V. [DOI] [PubMed] [Google Scholar]
- 7.Henriques AC, Carvalho Mde V, Miguel MC, Queiroz LM, da Silveira EJ. Clinical pathological analysis of nine cases of aneurysmal bone cyst of the jaws in a Brazilian population. Eur Arch Otorhinolaryngol. 2012;269(3):971–976. doi: 10.1007/s00405-011-1705-9. [DOI] [PubMed] [Google Scholar]
- 8.Struthers PJ, Shear M. Aneurysmal bone cyst of the jaws (I). Clinicopathological features. Int J Oral Surg. 1984;13:85–91. doi: 10.1016/S0300-9785(84)80077-0. [DOI] [PubMed] [Google Scholar]
- 9.Sun ZJ, Zhao YF, Yang RL, Zwahlen RA. Aneurysmal bone cysts of the jaws: analysis of 17 cases. J Oral Maxillofac Surg. 2010;68:2122–2128. doi: 10.1016/j.joms.2009.07.111. [DOI] [PubMed] [Google Scholar]
- 10.Pelo S, Gasparini G, Boniello R, Moro A, Amorso PF (2009) Aneurysmal bone cyst located in the mandibular condyle. Head Face Med 5(8). doi:10.1186/1746-160X-5-8 [DOI] [PMC free article] [PubMed]
- 11.Moller B, Claviez A, Moritz JD, Leuschner I, Wiltfang J. Extensive aneurysmal bone cyst of the mandible. J Craniofac Surg. 2011;22:841–844. doi: 10.1097/SCS.0b013e31820f3703. [DOI] [PubMed] [Google Scholar]
- 12.Vergel De Dios AM, Bond JR, Shives TC, McLEOD RA, Unni KK. Aneurysmal bone cyst. A clinicopathologic study of 238 cases. Cancer. 1992;69:2921–2931. doi: 10.1002/1097-0142(19920615)69:12<2921::AID-CNCR2820691210>3.0.CO;2-E. [DOI] [PubMed] [Google Scholar]
- 13.Szendroi M, Cser I, Konya A, et al. Aneurysmal bone cyst: a review of 52 primary and 16 secondary cases. Arch Orthop Trauma Surg. 1992;111:318–322. doi: 10.1007/BF00420058. [DOI] [PubMed] [Google Scholar]
- 14.El-Mofty S. Psammomatoid and trabecular juvenile ossifying fibroma of the craniofacial skeleton: two distinct clinicopathological entities. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93:296–304. doi: 10.1067/moe.2002.121545. [DOI] [PubMed] [Google Scholar]
- 15.Silva CAB, Silva AD, de Carvalho Soares JA, Furuse C, de Araujo NS, de Araujo VC. Trabecular juvenile ossifying fibroma with aneurysmal bone cyst: a rare presentation. Pediatr Dent. 2011;33(5):388–391. [PubMed] [Google Scholar]
- 16.Sankaranayaran S, Srinivas S, Sivakumar P, Sudhakar (Capt) R, Elangovan S. J Oral Maxillofac Pathol. 2011;15(3):299–302. doi: 10.4103/0973-029X.86693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Noffke CEE. Juvenile ossifying fibroma of the mandible. An 8 year radiological follow-up. Dentomaxillofacial Radiol. 1998;27:363–366. doi: 10.1038/sj.dmfr.4600384. [DOI] [PubMed] [Google Scholar]
- 18.Urs AB, Augustine J, Arora S, Kumar P. Rare pediatric presentation of aneurysmal bone cyst with trabecular juvenile ossifying fibroma and ossifying fibroma. Int J Pediatr Otorhinolaryngol. 2013;77(4):576–580. doi: 10.1016/j.ijporl.2012.12.021. [DOI] [PubMed] [Google Scholar]
- 19.Oliveira AM, Chou MM, Perez-Atayde AR, Rosenberg AE (2006) Aneurysmal bone cyst: a neoplasm driven by upregulation of the USP6 oncogene. J Clin Oncol 24(1):e1 [DOI] [PubMed]