

Abstract
Introduction George Winter attempted to assess the depth and difficulty of extracting impacted mandibular wisdom molars by describing three imaginary lines drawn on an intra-oral radiograph. Of these lines, the red line is the only one which is measured and great importance is attached to its actual length. Method The authors of this short paper describe the difficulty in drawing this red line accurately through examples. Conclusion The authors believe that Winter’s lines and their interpretation are only of historical value and have no place in contemporary texts on oral surgery.
Keywords: Winter’s lines, Difficulty index, Third molar depth
Introduction
In third molar surgery, it is imperative that a careful radiological evaluation be carried out prior to attempting extraction. The purpose of this exercise is to complement the clinical examination by providing additional information about the third molar, the related teeth and anatomical features and the surrounding bone. This is necessary in order to make a sound decision about the proposed surgical procedure, the most appropriate location for this to take place, and to highlight aspects of management that may require specific mention to the patient [1]. The current methods of estimating difficulty of extraction have been dominated by dental factors evident on radiological assessment of the third molar. This is reflected in the development of three classification systems based on dental factors (WHARFE-Macgregor 1985, Winters lines 1926 and Pell & Gregory classification 1933) [2].
George Winter was reputed to have devoted most of his time to study the various positions and the easiest way to remove impacted mandibular third teeth [3]. He described three imaginary lines which can be drawn on a standard intraoral radiograph that indicate the angulation, depth of the tooth in bone and the anticipated difficulty in removal. These lines are called Winter’s lines and are colour coded in order to facilitate discussion. The first “white” line is drawn along the occlusal surfaces of the erupted mandibular molars and extended posteriorly over the third molar region. This line is used to assess the axial inclination of the impacted tooth as it becomes immediately apparent. The second “amber” line is drawn from the surface of the bone lying distally to the third molar to the crest of the interdental septum between the first and second mandibular molars. It indicates the amount of alveolar bone enclosing the impacted tooth. The third or “red” line is used to measure the depth at which the impacted tooth lies within the mandible. It is a perpendicular dropped from the “amber” line to an imaginary point of application for an elevator which is usually the cemento-enamel (CE) junction on the mesial surface of the impacted tooth (except in case of a disto-angular impaction where the point of elevation lies on the buccal aspect of the tooth) [4].
It was claimed that the “red line”, if 5 mm or longer, is indicative that the tooth should be removed under general anesthesia. If the red line is 9 mm or more in length, the inferior surface of the crown of the impacted third molar may be either level with or below the apex of the 2nd molar. Based on his personal experience, Geoffrey Howe opined further that each mm increase in “red line” makes the tooth 3 times more difficult to remove [4]. These unsubstantiated claims have no scientific basis and have been contradicted in recent years [3].
The Winter’s WAR (white, amber, red) lines, though little used in daily practice, continue to be taught to dental students unchanged and unchallenged in many countries. Indeed, several recent Indian textbooks also propagate verbatim the method of drawing these lines [1, 5, 6]. Post-graduate students in India are expected to trace these lines and accurately interpret them as an integral part of their practical examination in oral surgery.
This paper describes the reason why Winter’s “red line” is conceptually flawed and should not be used to assess the difficulty for extraction of an impacted wisdom tooth.
The Difficulty of Drawing the Red-Line
Winter stated that the “red line” is a perpendicular drawn from the “amber line” to a point of elevation usually at the mesial cemento-enamel junction of an impacted tooth. A perpendicular in geometry is defined as a straight line drawn at an angle of 90° to a given line, plane, or surface. In the description given by Howe and others, it is unclear how to draw this line from a curved line (amber line: which traces the interdental bone and runs along the anterior border of the mandible) to a curved surface (outline of the impacted tooth). Since no horizontal plane is defined on the radiograph by the authors, where exactly the 90° angle forms is not mentioned.
The confusion is apparent in the illustration given in a popular website on oral surgery which erroneously shows the “red line” dropped from the “white line” (Fig. 1) [7].
Fig. 1.

The red line is erroneously shown as being perpendicular to the white line
One assumes from the diagrams that illustrate these lines in various texts that the perpendicular dropped from the “amber-line” to the point of elevation at the CE junction of the tooth, if extended will intersect with the inferior edge (true horizontal) of the radiograph at right angle (Fig. 2).
Fig. 2.
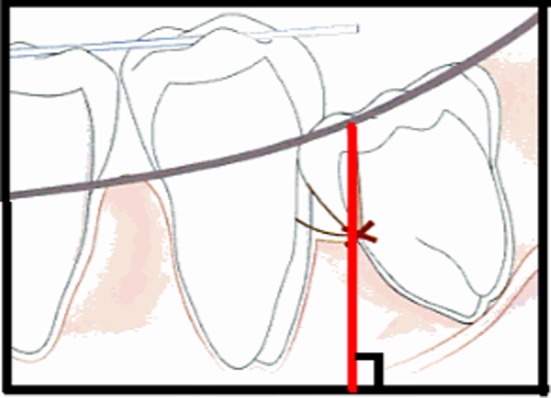
The red line when extended to the inferior edge of the radiograph should meet at 90°
The Changing Length of Redline with Change in Horizontal Angulation of the Film
If the above is true, then the “red line” is not a constant on intraoral radiographs which are not taken with the help of positioning devices (see later). Any deviation from horizontal orientation while placing the film will cause a change in the length of the “red line” as illustrated in Fig. 3. It is therefore an unreliable measurement to make on non-standardized IOPA radiographs.
Fig. 3.
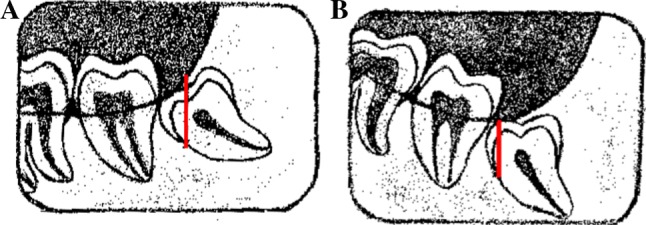
Change of angulation of the film causes the “red-line” to change in length significantly. The red-line in B is shorter by >30 % than in A with a 15° change in angulation of the film
The Radiograph on Which Measurements are Made is Not Standardized
Howe describes the method of taking the standardized intraoral radiograph [4]. The requirements for a standard intraoral radiograph for assessment of an impacted wisdom tooth is that it should be taken by the paralleling technique in which an enamel cap appearance of the second molar is seen [4]. This appearance is considered critical in the analysis of local factors causing difficulty in removing an impacted third molar. The advantage of intra-oral paralleling technique for radiographic evaluation is that there is no image enlargement, or distortion, while the radiation dose is decreased [8]. However, there is a “hit and miss” element involved in shooting these radiographs by utilizing the technique described, which may necessitate multiple exposures unless positioning devices are used.
Experience in implant surgery and endodontic procedures have underlined the importance of better techniques to reduce the angulation and magnification errors, if accurate measurements are to be taken on the intraoral radiograph. For this purpose many techniques for radiographic standardization procedures have been described using different X-ray devices, and adaptations, to meet the ideal radiographic criteria resulting in accurate diagnosis [9]. Techniques using a radiographic positioning device with an occlusal registration for geometric standardization are mostly utilized. Additionally, these techniques can be augmented with a gauge pin, as utilized by Kugelberg et al. [10] which allows easy calibration.
Contemporary textbooks on oral surgery rarely mention these methods of canceling the magnification and angulation errors on intraoral radiographs taken for assessing an impacted third molar. Also as mentioned by Pogrel [11], these methods are difficult and impractical to use in routine clinical practice. As a result most oral surgeons do not use positioning devices for intraoral radiographs taken for assessing an impacted third molar. The prevalent practice is therefore to rely on intraoral radiograph taken in a non-standardized manner or on orthopantomograms. Both radiographs are inappropriate as far as linear measurements between two points are to be made.
Conclusion
The authors therefore conclude that the Winter’s “red-line” is unreliable and of little practical value in assessing the depth or difficulty in removal of an impacted third molar. Since better radiographic assessment tools are available, it is time that undergraduate texts on oral surgery do away with the mention of WAR lines and relegate them to the pages of history.
References
- 1.Balaji SM. Textbook of oral and maxillofacial surgery. 2. New Delhi: Elsevier; 2013. [Google Scholar]
- 2.Renton T, Smeeton N, McGurk M. Factors predictive of difficulty of mandibular third molar surgery. Br Dent J. 2001;190:607–610. doi: 10.1038/sj.bdj.4801052. [DOI] [PubMed] [Google Scholar]
- 3.Biechina AE, Oji C, Fasola AO. Impacted mandibular third molars: depth of impaction and surgical methods of extraction among Nigerians. Odonto-Stomatol Trop. 2001;94:33–36. [PubMed] [Google Scholar]
- 4.Howe GL. Minor oral surgery. 2. Bristol: John Wright and Sons Publishers Ltd.; 1971. pp. 89–115. [Google Scholar]
- 5.Malik NA. Textbook of oral and maxillofacial surgery. 2. New Delhi: Jaypee Brothers Medical Publishers; 2008. [Google Scholar]
- 6.Ghosh PK. Synopsis of oral and maxillofacial surgery: an update overview. New Delhi: Jaypee Brothers Medical Publishers; 2008. p. 17. [Google Scholar]
- 7.Doran J (2013) Indices of difficulty in removing of 3rd molars (wisdom teeth). http://www.exodontia.info/Indices_of_Difficulty_of_3rd_Molar_Removal.html. Accessed on 9 May 2013
- 8.Jacobs R, van Steenberghe D. Radiographic planning and assessment of endosseous oral implants. Berlin: Springer; 1998. [Google Scholar]
- 9.Ana FI, Mercedes GT. A modified device for intraoral radiography to assess the distal osseous defects of mandibular second molar after impacted third molar surgery. Imaging Sci Dent. 2011;41:115–121. doi: 10.5624/isd.2011.41.3.115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kugelberg CF, Ahlstrom U, Ericson S, Hugoson A. Periodontal healing after impacted lower third molar surgery. Precision and accuracy of radiographic assessment of intrabony defects. Int J Oral Maxillofac Surg. 1986;15:675–678. doi: 10.1016/S0300-9785(86)80108-9. [DOI] [PubMed] [Google Scholar]
- 11.Pogrel MA. Removal of third molars. In: Khan HA, Bagheri SC, Bryan Bell R, editors. Current therapy in oral & maxillofacial surgery. Philadelphia: Elsevier Inc.; 2012. pp. 129–134. [Google Scholar]