

Abstract
Introduction
Early onset of substance use is a risk factor for later drug use, abuse, and dependence. This study examines how the rate of nicotine dependence differs as a function of age of onset of regular smoking in continuous time, in order to identify critical age periods that are most predictive of later dependence for males and females.
Methods
Time-varying effect modeling (TVEM) can reveal specific ages of onset that confer greatest risk for adult nicotine dependence. The rate of dependence in adulthood is modeled as a flexible function of age of onset using a subset of adults (N=15,748) from the National Epidemiologic Survey on Alcohol and Related Conditions who ever smoked regularly.
Results
The peak risk of adult nicotine dependence coincides with onset of regular use at approximately 10 years old, with an elevated risk persisting to 20 years. The risk of dependence is significantly higher for females compared to males for onset of regular use between ages 9 and 18.
Conclusions
Results suggest that the risk of adult nicotine dependence is highest when onset of regular smoking occurs at around 10 years, though the associated risk is high for ages of onset into young adulthood. Early onset of regular use is a relatively stronger risk factor for adolescent females than males. Smoking prevention programs should focus on late childhood through early adolescence, particularly among females. TVEM provides a more nuanced understanding of the risk associated with different ages of onset of health risk behaviors.
Keywords: nicotine dependence, cigarette smoking, time-varying effects, age of onset, sex differences
1. Introduction
Smoking is the leading cause of preventable death in the United States and worldwide (Centers for Disease Control and Prevention (CDC), 2004; World Health Organization (WHO), 2009). One reason for the high rates of smoking-related problems is the highly addictive nature of nicotine, which makes quitting smoking difficult once regular smoking has begun (Stolerman & Jarvis, 1995); only about 5% of smokers who attempt to quit are successful (CDC, 2004). About 17% of all adults meet lifetime criteria for nicotine dependence (Goodwin, Pagura, Spiwak, Lemeshow, & Sareen, 2011), with about half of adults who had ever engaged in regular smoking progressing to nicotine dependence (Breslau, Johnson, Hripi, & Kessler, 2001).
The progression to nicotine dependence is understood as an outcome of a series of milestones, including contemplating cigarette use, first cigarette, experimental smoking, regular smoking, and then ultimately dependence (Mayhew, Flay, & Mott, 2000). The age at which individuals reach particular smoking milestones has been implicated as a risk factor for nicotine dependence (Dierker et al., 2008). Early initiation is related to factors such as smoking susceptibility (Pierce, Choi, Gilpin, Farkas, & Merritt, 1996), neurobehavioral disinhibition (Tarter et al., 2003), and cigarette availability (Roberts, Colby, & Jackson, 2015). Early exposure to nicotine predicts higher rates of nicotine dependence in both animals (e.g., Brielmaier, McDonald, & Smith, 2007; Kota, Robinson, & Imad Damaj, 2009) and humans (e.g., Kendler, Myers, Damaj, & Chen, 2013). Several studies have found initiation of smoking before age 14 (Behrendt, Wittchen, Höfler, Lieb, & Beesdo, 2009), before age 16 (Breslau, Fenn, & Peterson, 1993), and before age 20 (Storr, Zhou, Liang, & Anthony, 2004) is associated with increased odds of nicotine dependence compared to initiation at later ages. However, as these studies compared different age groups rather than examining age continuously, it is not clear exactly which ages are associated with greater odds of dependence. In addition, most studies of the impact of smoking milestones on nicotine dependence focus on smoking initiation rather than regular smoking, and thus less is known about the effect of onset of regular smoking at different ages on later nicotine dependence (CDC, 2010).
The progression to nicotine dependence differs by sex. Although the mean age of first cigarette is slightly older for females (12.5 years) than males (12.0 years), mean age of onset of regular cigarette use is similar across sex (Dierker et al., 2012). Overall rates of adult nicotine dependence are slightly higher for men than women (14.1% v. 11.5%; Grant, Hasin, Chou, Stinson, & Dawson, 2004), but women may have a more difficult time quitting smoking than men once they are nicotine dependent (Cepeda-Benito, Reynoso, & Erath, 2004; Piper et al., 2010).
To derive more nuanced information about the association between age of onset and subsequent nicotine dependence and how this complex association varies across sex, we use the time-varying effect model (TVEM; Tan, Shiyko, Li, Li, & Dierker, 2012) to estimate regression coefficients as a flexible function of continuous age of onset. Previous applications of TVEM in tobacco research have used ecological momentary assessments to shed light on the dynamic associations between negative affect and craving (Lanza, Vasilenko, Liu, Li, & Piper, 2014), and between craving and cessation fatigue (Liu, Lanza, Vasilenko, & Piper, 2013) and between negative affect and smoking lapse (Vasilenko et al., 2014). A recent study (Selya et al., 2015) used TVEM to examine the mood between smoking and mood across continuous levels of dependence.
This study is the first to use TVEM to model the nuanced association between age of onset of a behavior and a later outcome. The rate of nicotine dependence in adulthood is modeled as a flexible function of age of first regular cigarette use; sex is examined as a moderator.
2. Methods
2.1 Participants and procedure
This study used data from Wave 1 of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC; National Institutes of Health, 2006), a national sample of the non-institutionalized U.S. population 18 years of age and older. The Wave 1 sample of N=43,093 adults was drawn from a survey administered by the National Institute on Alcohol Abuse and Alcoholism in 2001–2002. Participants in the overall sample were 43.0% male with mean age of 46.4 (SD=19.1); the racial/ethnic composition was 56.9% non-Hispanic White, 19.1% non-Hispanic Black, 19.3% Hispanic, 3.1% Asian/Native Hawaiian/Pacific Islander, and 1.6% American Indian/Alaska Native. Because of our focus on timing of first regular smoking, we limited our sample to those adults who reported ever having smoked cigarettes regularly by age 40. This resulted in a sample of 15,748 individuals (50.5% male; M age=48.7, SD=17.3; 66.9% non-Hispanic White, 16.5% non-Hispanic Black, 12.5% Hispanic, 1.9% Asian/Native Hawaiian/Pacific Islander, and 2.3% American Indian/Alaska Native).
2.2 Measures
Sex was measured by self-report. Age of onset of regular cigarette use was assessed by a self-report item about the age at which participants first started smoking cigarettes every day. Nicotine dependence, a binary indicator of whether the individual met the symptom criteria in the past 12 months, was assessed by the tobacco module of the Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV (AUDADIS-IV; Grant, Dawson, & Hasin, 2001). Diagnosis required respondents to satisfy at least 3 of 7 DSM-IV (American Psychiatric Association, 1994) criteria in the past year. Of the overall NESARC sample of adults, 11.5% met this definition; 29.5% of the analysis sample (adults who reported ever having smoked cigarettes regularly by age 40) met this definition. Among those with past-year nicotine dependence, past-year rates of tobacco product use were 95.3% cigarettes, 7.1% cigars, 1.2% pipe, 6.0% snuff, and 3.4% chew tobacco.
2.3 Analytic approach
Models were run using intercept-only logistic TVEM, a semi-parametric model that estimates regression coefficients as functions of continuous time (Vasilenko et al., 2014). Intercept-only models estimating the rate of adult dependence as a function of age of regular smoking onset were run for the full analysis sample, and then separately for male and female participants to allow sex to fully moderate the complex association. All models were run in SAS 9.3 using the %TVEM_logistic macro (Li et al., 2014).
3. Results
The mean age of onset of regular smoking was 18.6 (SD=4.7), and was significantly younger for males than females (18.2 and 19.1, respectively; t=12.5; p<.0001). The rate of past-year nicotine dependence differed significantly across sex, with 27.4% of males and 31.7% of females meeting this definition (chi-square=35.1, df=1, p<.0001).
3.1 Complex association between age of onset and nicotine dependence
Figure 1 shows the exponentiated intercept coefficient function for the full sample, reflecting the rate of nicotine dependence in adulthood as a function of age at first regular cigarette use. The rate of adult dependence is highest for individuals who experienced onset of regular use in middle childhood to early adolescence, with peak risk of adult dependence (43%) corresponding to regular smoking onset at approximately 10 years old. For ages of onset between 10 and 18, the rate of nicotine dependence in adulthood decreased steadily and steeply to about half the original rate, and then leveled off at about 25% for ages of onset from about 18 to 35; thereafter the rate decreased to around 15% for age of onset at age 40.
Figure 1.

Rate of nicotine dependence among ever-regular smokers as a function of age of first regular cigarette use.
3.2 Sex differences in the role of age of onset
Figure 2 shows prevalence of adult dependence as a function of age of onset separately for men and women. Ages where the confidence bands do not overlap indicate significantly different rates of nicotine dependence in adulthood for the two groups. There are significant sex differences at ages 9 to 18: females who first smoked regularly during those ages having higher rates of dependence in adulthood compared to males. Females’ rates of adult dependence peaked at more than 50% for an age of onset of approximately 10 years; this rate was double that for females with an age-of-onset of age 20 or older. For males, the rate of adult dependence peaked at 36% for an age of onset of around 10 years and was approximately 25% for an age of onset of 20 or older.
Figure 2.
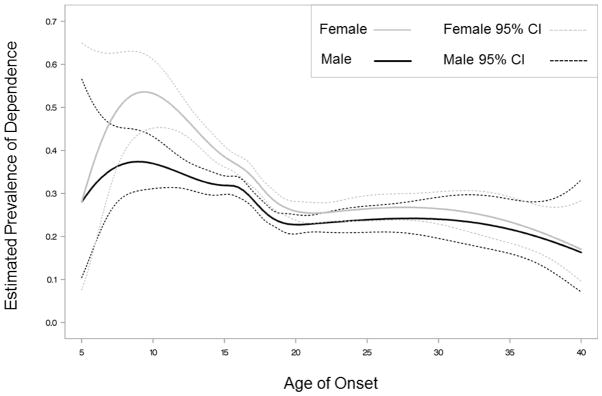
Rate of nicotine dependence among ever-regular smokers as a function of age of first regular cigarette use, by sex.
4. Discussion
4.1 Key findings
This paper used TVEM to examine how the odds of nicotine dependence in young adulthood differed depending on the age an individual first began regular smoking. We found that the peak risk for adult nicotine dependence corresponded to onset of regular smoking at around age 10; more than 40% of individuals beginning regular smoking at that age were dependent in adulthood, compared to less than 25% of those who imitated regular smoking after age 20. This is consistent with prior research (Behrendt, et al., 2009; Breslau et al., 1993; Storr et al., 2004) suggesting earlier smoking onset is associated with greater odds of dependence in adulthood. However, although early regular smoking confers a high risk of adult dependence, there are still a large number of people with early regular smoking who are not nicotine dependent, and future research should aim to better understand the factors that may protect individuals who smoke regularly from later dependence.
We also examined how the impact of early onset of regular smoking differed for men and women. We found that onset of regular smoking during the teen years was a greater risk for adult nicotine dependence among women. This suggests that once females begin regular smoking they may have more difficulty quitting and thus be more likely to progress to dependence, consistent with other research (Cepeda-Benito et al., 2004). Future research should aim to better understand these mechanisms in order to better intervene during this progression to dependence.
4.2 Limitations
Although there are important strengths of the NESARC data for studying nicotine dependence across the life span, the retrospective nature of questions about age of onset may introduce error. Additionally, age and historical year are confounded, and future longitudinal analyses could help differentiate age and cohort effects. We also note that age 40 as the cutoff of regular smoking onset was somewhat arbitrary; however results were robust to different choices of age of onset. Finally, estimates of adult nicotine dependence reflect current rates, rather than lifetime rates. By not taking into account the development of–and recovery from–nicotine dependence that may have occurred at some point prior to the timing of their NESARC assessment, the risk of regular cigarette smoking may be underrepresented.
4.3 Implications and future directions
Early first regular use of cigarettes confers high risk of nicotine dependence in adulthood. Important next steps include building on this investigation to consider the role of quantity of smoking after initiation, the complex associations of other smoking milestones, such as first full cigarette, with later nicotine dependence, and how age of reaching the different milestones is associated with later dependence across a variety of population subgroups. Such information could suggest promising behaviors to focus on in targeted intervention programs. In addition, a careful examination of the link between age of regular smoking onset and other substance use behaviors in adulthood, such as marijuana use, would shed light on broader health implications of early onset.
This study used data from a large epidemiologic study to demonstrate that the association between age of first regular smoking and nicotine dependence in adulthood is more complex than can be represented with a single cut-point. The pattern of the association was remarkably similar across sex, however it was significantly stronger among females across a full decade. The novel application of TVEM to existing data can provide important new insights about links between risk factors and a variety of health behaviors, thereby informing the development of more effective behavioral interventions (Coyle & DiClemente, 2014), including adaptive interventions that are tailored to meet the needs of the most at-risk individuals at specific times when they may be most vulnerable.
Highlights.
We examine the rate of adult nicotine dependence as flexible function of age of onset.
Peak risk of adult nicotine dependence coincides with onset of regular use at approximately 10 years old, with an elevated risk persisting to 20 years, for both males and females.
Risk of dependence is significantly higher for females compared to males for onset of regular use between ages 9 and 18.
Early onset of regular use is a relatively stronger risk factor for adolescent females than males.
Time-varying effect modeling provides more nuanced understanding of risk associated with different ages of onset of health risk behaviors.
Acknowledgments
Role of funding sources: This study was funded by awards P50 DA010075 from the National Institute on Drug Abuse and R01 CA168676 from the National Cancer Institute. This content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse, the National Cancer Institute, or the National Institutes of Health.
Preparation of this article was supported by the National Institute on Drug Abuse (grant no. P50 DA010075) and the National Cancer Institute (grant no. R01 CA168676). The authors wish to thank Ms. Amanda Applegate for helpful comments on an early draft.
Footnotes
Contributors: Author Stephanie T. Lanza conceptualized the study, analyzed the data, and wrote the first draft of the manuscript. Author Sara A. Vasilenko contributed to the summary of the literature, refined the draft, and created the figures.
Conflict of interest
The authors have no conflicts of interest to disclose.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4. American Psychiatric Association; Washington, DC: 1994. [Google Scholar]
- Behrendt S, Wittchen HU, Höfler M, Lieb R, Beesdo K. Transitions from first substance use to substance use disorders in adolescence: is early onset associated with a rapid escalation? Drug and Alcohol Dependence. 2009;99:68–78. doi: 10.1016/j.drugalcdep.2008.06.014. [DOI] [PubMed] [Google Scholar]
- Breslau N, Fenn N, Peterson EL. Early smoking initiation and nicotine dependence in a cohort of young adults. Drug and Alcohol Dependence. 1993;33:129–137. doi: 10.1016/0376-8716(93)90054-t. [DOI] [PubMed] [Google Scholar]
- Breslau N, Johnson EO, Hiripi E, Kessler R. Nicotine dependence in the United States: Prevalence, trends, and smoking persistence. Archives of General Psychiatry. 2001;58:810–816. doi: 10.1001/archpsyc.58.9.810. [DOI] [PubMed] [Google Scholar]
- Brielmaier JM, McDonald CG, Smith RF. Immediate and long-term behavioral effects of a single nicotine injection in adolescent and adult rats. Neurotoxicology and Teratology. 2007;29:74–80. doi: 10.1016/j.ntt.2006.09.023. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC) Cigarette smoking among adults: United States, 2002. Morbidity and Mortality Weekly Report. 2004;53:427–431. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, & Office on Smoking and Health. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Atlanta (GA): Centers for Disease Control and Prevention (US); 2010. Nicotine Addiction: Past and Present. [PubMed] [Google Scholar]
- Cepeda-Benito A, Reynoso JT, Erath S. Meta-analysis of the efficacy of nicotine replacement therapy for smoking cessation: Differences between men and women. Journal of Consulting and Clinical Psychology. 2004;72:712–722. doi: 10.1037/0022-006X.72.4.712. [DOI] [PubMed] [Google Scholar]
- Coyle KK, DiClemente RJ. Time-varying risk behaviors among adolescents: Implications for enhancing the effectiveness of sexual risk reduction interventions. Journal of Adolescent Health. 2014;55:465–466. doi: 10.1016/j.jadohealth.2014.07.017. [DOI] [PubMed] [Google Scholar]
- Dierker L, He J, Kalaydjian A, Swendsen J, Degenhardt L, Glantz M, Merikangas K. The importance of timing of transitions for risk of regular smoking and nicotine dependence. Annals of Behavioral Medicine. 2008;36:87–92. doi: 10.1007/s12160-008-9051-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dierker L, Swendsen J, Rose J, He J, Merikangas K The Tobacco Etiology Research Network. Transitions to regular smoking and nicotine dependence in the adolescent national comorbidity survey (NCS-A) Annals of Behavioral Medicine. 2012;43:394–401. doi: 10.1007/s12160-011-9330-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grant BF, Dawson DA, Hasin DS. The Alcohol Use Disorder and Associated Disabilities Interview Schedule–DSM–IV Version. National Institute on Alcohol Abuse and Alcoholism; Bethesda, MD: 2001. [Google Scholar]
- Grant BF, Hasin DS, Chou SP, Stinson FS, Dawson DA. Nicotine dependence and psychiatric disorders in the United States: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Archives of General Psychiatry. 2004;61:1107–1115. doi: 10.1001/archpsyc.61.11.1107. [DOI] [PubMed] [Google Scholar]
- Goodwin RD, Pagura J, Spiwak R, Lemeshow AR, Sareen J. Predictors of persistent nicotine dependence among adults in the United States. Drug and Alcohol Dependence. 2011;118:127–133. doi: 10.1016/j.drugalcdep.2011.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kendler KS, Myers J, Damaj MI, Chen X. Early smoking onset and risk for subsequent nicotine dependence: A monozygotic co-twin control study. The American Journal of Psychiatry. 2013;170:408–413. doi: 10.1176/appi.ajp.2012.12030321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kota D, Robinson SE, Imad Damaj M. Enhanced nicotine reward in adulthood after exposure to nicotine during early adolescence in mice. Biochemical Pharmacology. 2009;78:873–879. doi: 10.1016/j.bcp.2009.06.099. [DOI] [PubMed] [Google Scholar]
- Lanza ST, Vasilenko S, Liu X, Li R, Piper M. Advancing the understanding of craving during smoking cessation attempts: A demonstration of the time-varying effect model. Nicotine and Tobacco Research. 2014;16(Suppl 2):S127–S134. doi: 10.1093/ntr/ntt128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li R, Tan X, Huang L, Wagner AT, Yang J. TVEM (time-varying effect model) SAS macro suite users’ guide (Version 2.1.1) University Park: The Methodology Center; Penn State: 2014. Retrieved from http://methodology.psu.edu. [Google Scholar]
- Liu X, Li R, Lanza ST, Vasilenko S, Piper M. Understanding the role of cessation fatigue in the smoking cessation process. Drug and Alcohol Dependence. 2013;133:548–555. doi: 10.1016/j.drugalcdep.2013.07.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mayhew KP, Flay BR, Mott JA. Stages in the development of adolescent smoking. Drug and Alcohol Dependence. 2000;59:61–81. doi: 10.1016/S0376-8716(99)00165-9. [DOI] [PubMed] [Google Scholar]
- National Institutes of Health. Alcohol Use and Alcohol Use Disorders in the United States: Main Findings from the 2001–2002 National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) National Institute on Alcohol Abuse and Alcoholism; Rockville, MD: 2006. [Google Scholar]
- Pierce JP, Choi WS, Gilpin EA, Farkas AJ, Merritt RK. Validation of susceptibility as a predictor of which adolescents take up smoking in the United States. Health Psychology. 1996;15:355–361. doi: 10.1037//0278-6133.15.5.355. http://dx.doi.org/10.1037/0278-6133.15.5.355. [DOI] [PubMed] [Google Scholar]
- Piper ME, Smith SS, Fleming MF, Bittrich AA, Brown JL, Leitzke CJ, Zehner ME, Fiore MC, Baker TB. Psychiatric disorders in smokers seeking treatment for tobacco dependence: Prevalence and relations with tobacco dependence and cessation. Journal of Consulting and Clinical Psychology. 2010;78:13–23. doi: 10.1037/a0018065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts ME, Colby SM, Jackson KM. What predicts early smoking milestones? Journal of Studies on Alcohol and Drugs. 2015;76:256–266. doi: 10.15288/jsad.2015.76.256. http://dx.doi.org/10.15288/jsad.2015.76.256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Selya AS, Updegrove N, Rose JS, Dierker LC, Tan X, Hedeker D, Li R, Mermelstein RJ. Nicotine-dependence-varying effects of smoking events on momentary mood changes among adolescents. Addictive Behaviors. 2015;41:65–71. doi: 10.1016/j.addbeh.2014.09.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stolerman IP, Jarvis MJ. The scientific case that nicotine is addictive. Psychopharmacology. 1995;117:2–10. doi: 10.1007/BF02245088. [DOI] [PubMed] [Google Scholar]
- Storr CL, Zhou H, Liang KY, Anthony JC. Empirically derived latent classes of tobacco dependence syndromes observed in recent-onset tobacco smokers: epidemiological evidence from a national probability sample survey. Nicotine & Tobacco Research. 2004;6:533–45. doi: 10.1080/14622200410001696493. [DOI] [PubMed] [Google Scholar]
- Tan X, Shiyko MP, Li R, Li Y, Dierker L. A time-varying effect model for intensive longitudinal data. Psychological Methods. 2012;17:61–77. doi: 10.1037/a0025814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tarter RE, Kirisci L, Mezzich A, Cornelius JR, Pajer K, Vanyukov M, Gardner W, Blackson T, Clark D. Neurobehavioral disinhibition in childhood predicts early age at onset of substance use disorder. American Journal of Psychiatry. 2003;160:1078–1085. doi: 10.1176/appi.ajp.160.6.1078. [DOI] [PubMed] [Google Scholar]
- TVEM SAS Macro Suite (Version 2.1.1) [Software] University Park: The Methodology Center, Penn State; 2014. Retrieved from http://methodology.psu.edu. [Google Scholar]
- Vasilenko SA, Piper ME, Lanza ST, Liu X, Yang J, Li R. Time-varying processes involved in smoking lapse in a randomized trial of smoking cessation therapies. Nicotine and Tobacco Research. 2014;16:S135–S143. doi: 10.1093/ntr/ntt18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization (WHO) Report on the global tobacco epidemic: Implementing smoke-free environments. Geneva: 2009. [Google Scholar]