

Abstract
Background:
The aim was to assess the validity and reliability of the Persian version of shortened disabilities of the arm, shoulder, and hand (Quick-DASH) questionnaire in patients with upper extremity conditions.
Methods:
We administered the Persian version of Quick-DASH to 202 patients with upper extremity conditions, of which 71 patients randomly returned after 3 days to respond to the questionnaire for the 2nd time. In order to test the construct validity of the questionnaire, patients responded to the Michigan Hand Outcome Questionnaire (MHOQ) and Short Form 36 Health Survey (SF-36) as well. Internal consistency was tested using the Cronbach's alpha, and test-retest reliability was measured using intra-class correlation coefficient (ICC).
Results:
Cronbach's alpha was 0.90. ICC was 0.89. Convergent validity was confirmed, as the Spearman correlation between the Quick-DASH and MHOQ was 0.67 and ranged from 0.24 to 0.56 between the subscales of the SF-36 and Quick-DASH.
Conclusions:
Observation of excellent internal consistency, good to excellent test-retest reliability, and moderate to strong construct validity confirms the validity and reliability of the Persian version of Quick-DASH for evaluating the magnitude and level of disability in upper extremity conditions.
Keywords: Persian, psychometric, Quick-disabilities of the arm, shoulder and hand, reliability, validity
INTRODUCTION
Outcome measures are important means in the evaluation of the quality of life and function. Disabilities of the arm, shoulder, and hand (DASH) questionnaire is a patient-reported outcome measure (PROM) that measures the magnitude of disability for the upper extremity.[1] It consists of 30 items, 21 of which assess the ability to perform physical activities, 5 items measure pain, and 4 items measure the psychosocial effects.[1] Item elimination in order to shorten the questionnaire resulted in an 11-item instrument, which proved to be as reliable as the original DASH instrument.[2] This shortened version was introduced as Quick-DASH in 2005.[2] Retention of the clinically oriented questions in the Quick-DASH made it a comparable instrument to the full DASH questionnaire. The Quick-DASH is more appealing than the DASH because it can be administered in the clinic in a shorter time.[3]
A well-translated and adapted questionnaire would facilitate multicenter studies and increases the feasibility of meta-analysis studies.[4] Farsi is spoken in several countries including Iran, Tajikistan, Afghanistan, and some regions of Pakistan and Iraq. Validity of the Quick-DASH has been tested in several other languages.
In this study, our aim was to assess the validity and reliability of the Persian version of the Quick-DASH in patients with upper extremity conditions.
METHODS
Patients
In total, 202 patients with upper extremity problems enrolled in this study from January 2013 to December 2013. Inclusion criteria were age above 18 years, ability to read and write Persian as a mother tongue, and a minimum of 4-week symptom duration [Table 1]. At the first visit, all patients responded to the Persian Quick-DASH as well as the Persian Short Form 36 Health Survey (SF-36) and the Michigan Hand Outcome Questionnaire (MHOQ) [Table 2]. To test the reliability, 71 patients accepted to return for the second visit after 3 days to fill the Persian Quick-DASH without receiving any major treatment or changes in symptoms. This study was reviewed and approved by the Committee of Research and patients consented verbally to participate in the study.
Table 1.
Characteristics of patients with upper extremity conditions (n=202)
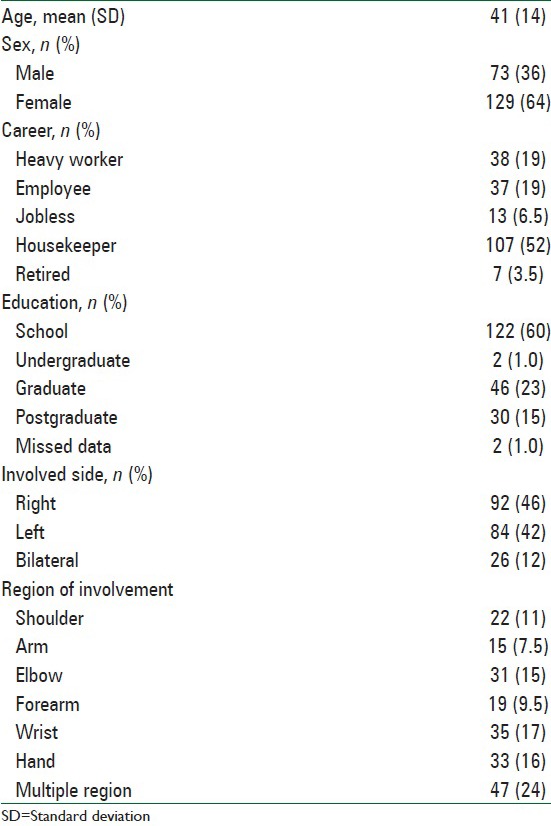
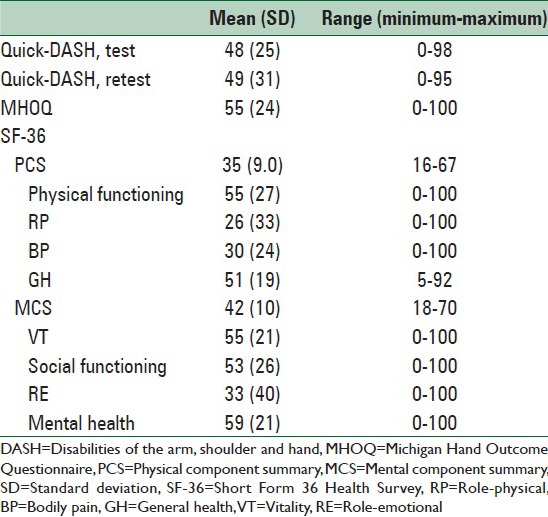
Table 2.
Average functional score of patients with upper extremity conditoins (n=202)
Reliability testing
Reliability can be test by either measuring the Cronbach's alpha for internal consistency[5] or intra-class correlation coefficient (ICC) for test-retest reliability (reproducibility).[6] Internal consistency measures the consistency of responses across the questionnaire and the subscales. Commonly accepted values for Cronbach's alpha are described as excellent for α > 0.9, good for 0.9 > α > 0.7, acceptable for 0.7 > α > 0.6, poor for 0.6 > α > 0.5, and unacceptable for α < 0.5. Test-retest reliability is tested by administering a questionnaire to a patient on two separate occasions without any substantial changes in his/her symptoms. A correlation coefficient of 0 indicates no reliability, whereas a value of 1 indicates excellent reliability. To measure test-retest reliability in our study, 71 patients randomly filled the Persian Quick-DASH for a 2nd time 3 days after the first visit, without being given any major treatment or surgery.
Construct validity
To test the construct validity, the new questionnaire is tested against a validated questionnaire with similar or relevant context to assess the correlation between the two questionnaires.[7] We tested the Persian Quick-DASH against the SF-36 questionnaire and MHOQ, which have been validated in Persian. The correlation was calculated using Spearman's correlation coefficient.
Statistics
Statistical analysis performed using SPSS version 11.5 (SPSS Inc., Chicago, IL, USA). P < 0.05 were considered as significant.
Short Form 36 Health Survey questionnaire
The SF-36 is an easily administered PROM that is frequently used to measure the quality of life. It consists of 36 questions divided into two major domains of physical and mental components, each one consisting of four sub-domains physical function, role-physical, bodily pain, and general health are sub-domains of functional health. Vitality, social function, role-emotional and mental health are sub-domains of psychometrical health. Montazeri et al. in 2005[8] and Jafari et al.[9] in 2008 have validated the Persian version of the SF-36.
Michigan Hand Outcome Measure
Michigan Health Outcome Questionnaire is a hand specific questionnaire.[10] It consists of 37 items divided into six subscales, including hand function, pain, activities of daily living, work, esthetics, and patient satisfaction. The Persian version of the MHOQ was validated by Ebrahimzadeh et al. (under peer review).[11]
RESULTS
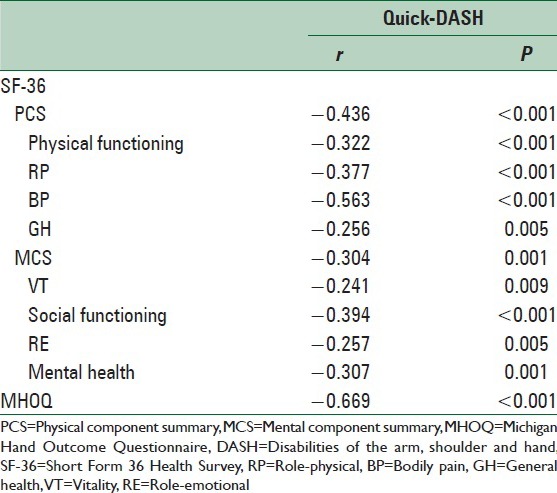
Cronbach's alpha was 0.90, indicating excellent internal consistency [Table 3]. ICC was 0.89, indicating good to excellent test-retest reliability [Table 3]. There was a high and significant inverse correlation between the Quick-DASH and the MHOQ, and the sub-domains of the SF-36, indicating a strong correlation between the Quick-DASH and the other validated questionnaire in the same domain [Table 4]. Convergent validity was confirmed, as the Spearman correlation between the Quick-DASH and MHOQ was 0.67 and ranged from 0.24 to 0.56 between the sub-domains of the SF-36 and Quick-DASH [Table 4].
Table 3.
Internal consistency and test-retest reliability of the Farsi version of the Quick-DASH
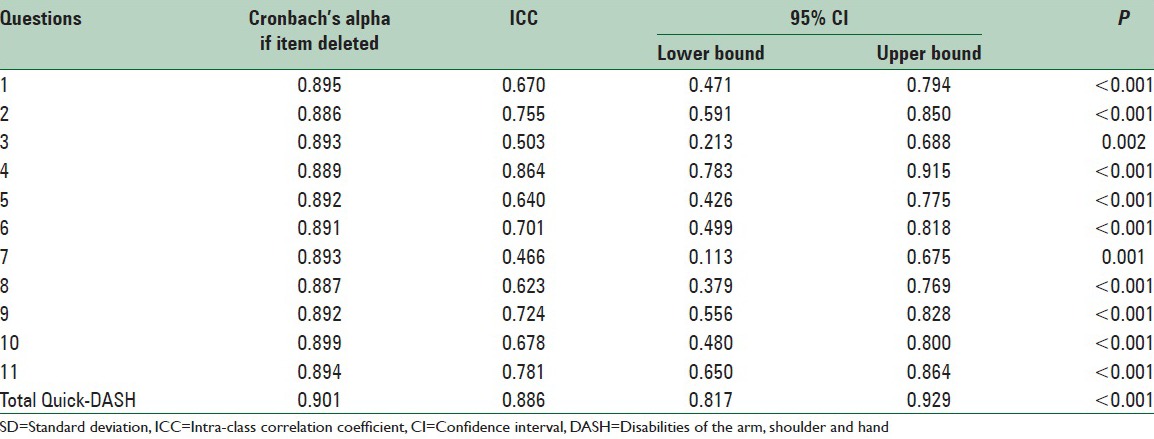
Table 4.
Convergent validity expressed by Spearman's rho correlation coefficient between Quick-DASH and subdomins of the SF-36 and MHOQ
DISCUSSION
The purpose of this study was to establish the validity of the Persian version of the Quick-DASH in patients with upper extremity conditions. Our results indicate that Farsi Quick-DASH is a reliable and valid instrument for studying outcomes in patients with upper extremity conditions. In the current study, internal consistency and test-retest reliability indicated the excellent reliability of the Farsi version of the Quick-DASH. Testing the construct validity revealed moderate to strong correlation between Quick-DASH and the MHQ and subscales of the SF-36.
There are some limitations to our study. First of all, this is a single-center study, which may not represent the general patient population. However, this is a major tertiary referral center, providing care to the entire North East and East, and South East provinces of Iran. Another limitation was the administration of SF-36 questionnaire, which is more general than Quick-DASH, and MHOQ, which is more specific compared to the Quick-DASH, to test construct validity; however, some studies have shown relatively small differences in the responsiveness of the more general and more specific measures of disability.
Translations of the DASH questionnaire are available in most languages;[12] However, less work has been done in the cross-cultural adaptation of the Quick-DASH. Translations to French,[13] Turkish[14] and Japanese[15] are available and validated. In French, Japanese, and Turkish versions, Cronbach's alpha was 0.89, 0.88 and 0.84, respectively, showing good internal consistency. Similarly, ICC was 0.94, 0.93, and 0.82 in French, Turkish, and Japanese versions, respectively, showing good test-retest reliability. In our study, Cronbach's alpha and ICC were 0.90 and 0.89 respectively, showing comparable results with previously validated versions, indicating the reliability of our study.
We compared the Quick-DASH with SF-36 and MHOQ to test the construct validity, using Spearman's correlation coefficient. In order to test the construct validity of the Turkish version of the Quick-DASH, Koldas Dogan et al. studied patients with carpal tunnel syndrome using the Boston Carpal Tunnel Questionnaire, visual analogue scale-pain (VAS-pain), and pinch and grip strength tests to measure the correlation in responsiveness with Quick-DASH.[14] Quick-DASH showed moderate correlations with VAS-pain and grip strength test, a good correlation with the pinch strength test, and high correlation with Boston Carpal Tunnel Questionnaire. The Japanese version of the Quick-DASH was tested against the DASH, SF-36 and VAS. The correlation coefficients were 0.92 and 0.52 when compared with DASH and VAS, respectively. In addition, correlations between Quick-DASH and SF-36 subscales ranged from −0.29 to −0.73.[15] In a study to validate the French version, the correlation was tested using subjective assessment of activities of daily living (ADL), active range of motion (ROM), and measurement of abduction strength (strength). Correlation of the French Quick-DASH score with scores for French DASH (r = 0.96), perceived handicap score (r = 0.79), ADL (r = −0.73), pain during activities (r = 0.63), strength (r = −0.58), pain at rest (r = 0.57), and ROM (r = −0.51) indicated good construct validity.[12]
CONCLUSIONS
In this study, we evaluated the reliability and validity of the Persian version of the Quick-DASH. Observation of excellent internal consistency, good to excellent test-retest reliability, and moderate to strong construct validity confirms the validity and reliability of the Persian Quick-DASH in the evaluation of the magnitude of disability for upper extremity conditions.[13]
ACKNOWLEDGEMENTS
We would like to appreciate for support of Orthopedic Research Center at Mashhad University of Medical Sciences.
Footnotes
Source of Support: Orthopedic Research Center at Mashhad University of Medical Sciences.
Conflict of Interest: None declared.
REFERENCES
- 1.Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand) [corrected] The Upper Extremity Collaborative Group (UECG) Am J Ind Med. 1996;29:602–8. doi: 10.1002/(SICI)1097-0274(199606)29:6<602::AID-AJIM4>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]
- 2.Beaton DE, Wright JG, Katz JN. Upper Extremity Collaborative Group. Development of the QuickDASH: Comparison of three item-reduction approaches. J Bone Joint Surg Am. 2005;87:1038–46. doi: 10.2106/JBJS.D.02060. [DOI] [PubMed] [Google Scholar]
- 3.London DA, Stepan JG, Boyer MI, Calfee RP. Performance characteristics of the verbal QuickDASH. J Hand Surg Am. 2014;39:100–7. doi: 10.1016/j.jhsa.2013.09.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kennedy CA, Beaton DE, Smith P, Van Eerd D, Tang K, Inrig T, et al. Measurement properties of the QuickDASH (disabilities of the arm, shoulder and hand) outcome measure and cross-cultural adaptations of the QuickDASH: A systematic review. Qual Life Res. 2013;22:2509–47. doi: 10.1007/s11136-013-0362-4. [DOI] [PubMed] [Google Scholar]
- 5.Kline P. 2nd ed. London: Routledge; 2000. The Handbook of Psychological Testing; p. 13. [Google Scholar]
- 6.Koch GG. Intraclass correlation coefficient. Encyclopedia of Statistical Sciences. In: Kotz S, Johnson NL, editors. 4th ed. New York: John Wiley and Sons; 1982. pp. 213–7. [Google Scholar]
- 7.Smith EV., Jr Evidence for the reliability of measures and validity of measure interpretation: A Rasch measurement perspective. J Appl Meas. 2001;2:281–311. [PubMed] [Google Scholar]
- 8.Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The Short Form Health Survey (SF-36): Translation and validation study of the Iranian version. Qual Life Res. 2005;14:875–82. doi: 10.1007/s11136-004-1014-5. [DOI] [PubMed] [Google Scholar]
- 9.Jafari H, Lahsaeizadeh S, Jafari P, Karimi M. Quality of life in thalassemia major: Reliability and validity of the Persian version of the SF-36 questionnaire. J Postgrad Med. 2008;54:273–5. doi: 10.4103/0022-3859.41432. [DOI] [PubMed] [Google Scholar]
- 10.Chung KC, Pillsbury MS, Walters MR, Hayward RA. Reliability and validity testing of the Michigan Hand Outcomes Questionnaire. J Hand Surg Am. 1998;23:575–87. doi: 10.1016/S0363-5023(98)80042-7. [DOI] [PubMed] [Google Scholar]
- 11.Mohammad H. Ebrahimzadeh, Ali Birjandinejad, Amir Reza Kachooei. Cross-cultural adaptation, validation, and reliability of the michigan hand outcomes questionnaire among persian population. Hand Surgery. 2015;20:25–31. doi: 10.1142/S0218810415500033. [DOI] [PubMed] [Google Scholar]
- 12.Mousavi SJ, Parnianpour M, Abedi M, Askary-Ashtiani A, Karimi A, Khorsandi A, et al. Cultural adaptation and validation of the Persian version of the Disabilities of the Arm, Shoulder and Hand (DASH) outcome measure. Clin Rehabil. 2008;22:749–57. doi: 10.1177/0269215508085821. [DOI] [PubMed] [Google Scholar]
- 13.Ayad F, Lefevre-Colau MM, Gautheron V, Macé Y, Fermanian J, Mayoux-Benhamou A, et al. Reliability, validity and responsiveness of the French version of the questionnaire Quick Disability of the Arm, shoulder and Hand in shoulder disorders. Man Ther. 2009;14:206–12. doi: 10.1016/j.math.2008.01.013. [DOI] [PubMed] [Google Scholar]
- 14.Koldas Dogan S, Ay S, Evcik D, Baser O. Adaptation of Turkish version of the questionnaire Quick Disability of the Arm, Shoulder, and Hand (Quick DASH) in patients with carpal tunnel syndrome. Clin Rheumatol. 2011;30:185–91. doi: 10.1007/s10067-010-1470-y. [DOI] [PubMed] [Google Scholar]
- 15.Imaeda T, Toh S, Wada T, Uchiyama S, Okinaga S, Kusunose K, et al. Validation of the Japanese Society for Surgery of the Hand Version of the Quick Disability of the Arm, Shoulder, and Hand (QuickDASH-JSSH) questionnaire. J Orthop Sci. 2006;11:248–53. doi: 10.1007/s00776-006-1013-1. [DOI] [PMC free article] [PubMed] [Google Scholar]