

The management of patients with type 2 diabetes remains a frequent and often unresolved challenge encountered in clinical practice. The complex pathophysiology, the numerous barriers and difficulties faced by patients, and the rapid rise in obesity prevalence contribute to the enormity of this challenge, making it essential that patient management be individualized.
Fortunately, advances in treatment provide greater opportunities to individualize therapy. For example, insulin analogs are vastly improved compared to the animal-sourced insulins that were used for decades; they also have important advantages compared to short- and intermediate-acting human insulins.1,2
Another advance has been the development of glucagon-like peptide-1 (GLP-1) receptor agonists and dipeptidyl peptidase-4 (DPP-4) inhibitors that act on the incretin system to stimulate insulin secretion and inhibit glucagon secretion, both in a glucose-dependent manner.3–7 GLP-1 receptor agonists currently available in the United States are exenatide twice daily (BID), exenatide once weekly (QW), and liraglutide; currently available DPP-4 inhibitors are alogliptin, linagliptin, saxagliptin, and sitagliptin.
Although both drug classes work via the incretin system, there are important differences between the two. This article highlights these differences and provides a more focused discussion of strategies to initiate and optimize the use of the GLP-1 receptor agonists in collaboration with patients.
The results of clinical trials, particularly head-to-head comparisons, serve as the primary evidence base for this discussion. However, strict inclusion and exclusion criteria and abbreviated descriptions of study methodology in many clinical trials present challenges in applying these results to the care of individual patients.8 Because evidence-based medicine is about integrating the best external evidence with clinical experience, as described by Sackett et al.9 and others,10,11 this article supplements the evidence base with the author’s experience as a clinician and investigator. The article is not intended to provide a detailed discussion regarding the basic pharmacology of incretin-based therapy, which may be found elsewhere.12–14
Role of Incretin-Based Therapy in Type 2 Diabetes
GLP-1 receptor agonists and DPP-4 inhibitors are included in the 2012 American Diabetes Association (ADA)/European Association for the Study of Diabetes (EASD) and 2013 American Association of Clinical Endocrinologists guidelines as second-line therapy for patients who do not achieve glycemic control with the combination of lifestyle management and metformin.1,2 They are also included as recommended options for three-drug combination therapy.
The glucose-lowering effects of agents in both classes have been shown to be durable over 1.5–3 years of treatment.15–20 Both types of agents avoid some of the limitations associated with several other glucose-lowering therapies. For example, when avoidance of hypoglycemia is an important treatment goal in patients not at glycemic goal with metformin, the addition of a GLP-1 receptor agonist or DPP-4 inhibitor (or a thiazolidinedione [TZD]) is recommended by the ADA/EASD because of their low risk of hypoglycemia.21 Similarly, when avoidance of weight gain is an important treatment goal in patients not at glycemic goal with metformin, GLP-1 receptor agonists and DPP-4 inhibitors are the recommended treatment options.21 There are, however, important differences between the two drug classes that affect when and how they should be used to individualize therapy.
Comparison of GLP-1 Receptor Agonists and DPP-4 Inhibitors in Type 2 Diabetes
There are several key differences between the two classes of incretin-based therapy, with the first being that GLP-1 receptor agonists are delivered through subcutaneous injection, whereas DPP-4 inhibitors are taken orally. However, further comparison makes clear that DPP-4 inhibitors are not oral versions of the GLP-1 receptor agonists (Table 1).16,22–53
Table 1.
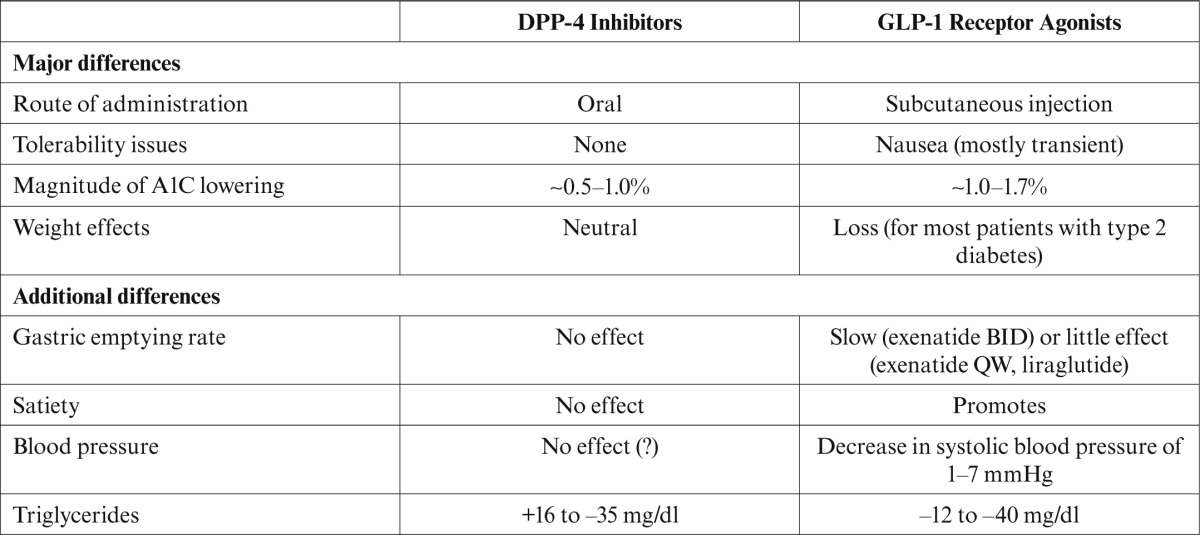
Second, initiation of GLP-1 receptor agonist therapy is sometimes associated with nausea, whereas DPP-4 inhibitors have no significant tolerability issues. Nausea with GLP-1 receptor agonists is usually mild, peaks within 8 weeks of starting exenatide BID and 4–8 weeks of starting liraglutide, and resolves in all but ∼ 10% of cases within 28 weeks with exenatide BID and 8 weeks with liraglutide.22–24 Nausea also peaks early after initiation of exenatide QW and resolves within 10 weeks in nearly all patients.25
A third difference is in A1C reduction, which is about 1.0–1.7% with GLP-1 receptor agonists16,25–29 compared to 0.5–1.0% with the DPP-4 inhibitors.30–34
Another difference is that GLP-1 receptor agonists promote a 1- to 4-kg weight loss in most people with type 2 diabetes, whereas DPP-4 inhibitors are weight neutral. DPP-4 inhibitors do not promote satiety, probably because their use results in a level of GLP-1 activity that is only approximately one-sixth that of the GLP-1 receptor agonists.35–37
There are additional differences between the two incretin-based drug classes. Unlike the DPP-4 inhibitors, the GLP-1 receptor agonists, especially exenatide BID, slow patients’ gastric emptying rate.38,39 This likely is one factor that contributes to the greater reduction in the postprandial glucose with the GLP-1 receptor agonists compared to DPP-4 inhibitors.1,39,40 In a 6-week crossover trial, postprandial glucose was reduced by 112 mg/dl with exenatide BID and 37 mg/dl with sitagliptin.39
Cardiovascular biomarkers are also positively affected with GLP-1 receptor agonists, which typically lower systolic blood pressure 1–7 mmHg, with diastolic blood pressure unaffected.7,21,25,27,41–48 The blood pressure effects of DPP-4 inhibitors are equivocal,41,42,49,50 although one study51 showed a 10-mmHg reduction in systolic blood pressure with sitagliptin over 6 months.
In terms of the lipid profile, the largest effect of both drug classes is on triglycerides, with a reduction of 12–40 mg/dl with GLP-1 receptor agonists and changes of +16 to –35 mg/dl with DPP-4 inhibitors.7,23,27,29,41,44–48,50,52,53 Although these effects on blood pressure and lipids are modest and no cardiovascular outcomes trials have been completed, they may provide additional benefit in a population that is at increased risk of cardiovascular complications.
Although agents from both classes are well tolerated, acute pancreatitis has been observed in a small percentage of patients treated with either one. Whether the acute pancreatitis resulted directly from treatment with these agents is widely debated54,55 and is being actively investigated.56–61 Until this issue is clarified, it is suggested that the two incretin-based therapies be avoided in patients with a history of pancreatitis.
The long-term safety of both drug classes is only beginning to emerge.62 One safety concern that has arisen from studies in animals and from postmarketing reports is the possibility of an increased risk of thyroid C-cell tumors with GLP-1 receptor agonists. Data from studies in rodents using liraglutide doses eight times higher than in humans showed an increased risk of C-cell tumors; however, tumors were also observed in rodents not receiving a GLP-1 receptor agonist.57 Investigation in monkeys using doses > 60 times human exposure levels for 20 months has shown no evidence of C-cell hyperplasia.63
The risk to humans is thought to be low because GLP-1 receptors are not present to a high degree in the human thyroid as they are in the rodent thyroid.63 In addition, calcitonin (a marker of C-cell tumors) in patients exposed to liraglutide for 2 years has been shown to remain at the lower end of the normal range, and the proportion of patients whose calcitonin increased above the clinically relevant cutoff value of 20 pg/ml was similar with liraglutide and comparator treatments in nine clinical trials.63
Numerous long-term safety investigations are ongoing for various disorders such as acute pancreatitis, thyroid cancer, cardiovascular events, renal safety, and hypersensitivity reactions.56,58–61,64
Comparison of GLP-1 Receptor Agonists in Type 2 Diabetes
There are many important differences among the three GLP-1 receptor agonists (Table 2). Several of these relate to the dosing and administration of the three agents.
Table 2.
Key Differences Among the GLP-1 Receptor Agonists
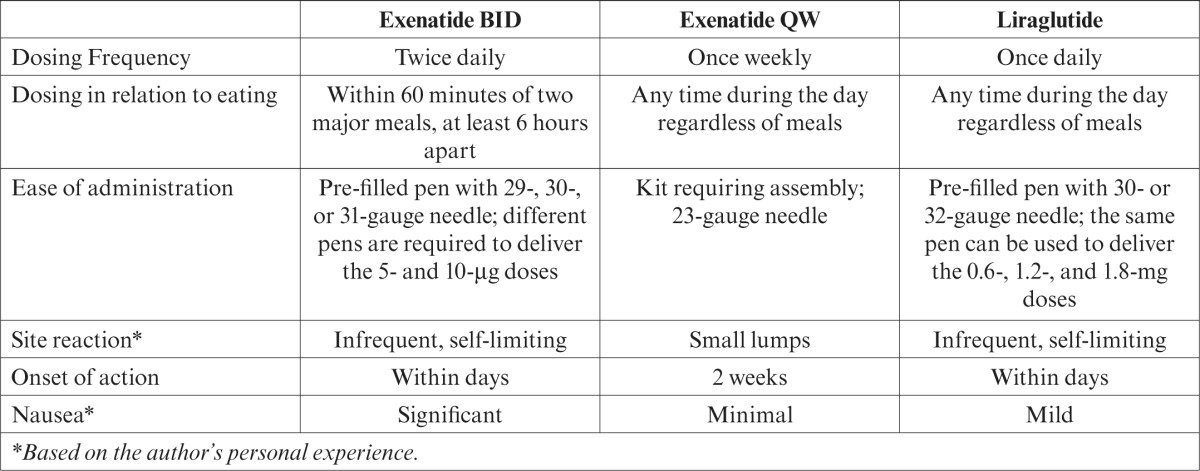
The need to administer exenatide BID twice daily at least 6 hours apart and within 60 minutes of eating can be difficult for patients. There is greater flexibility with exenatide QW and liraglutide, both of which can be administered without regard to meals. The once-weekly administration of exenatide QW and once-daily administration of liraglutide also serve to simplify administration.
Exenatide BID and liraglutide are available as pre-filled pen devices with narrow-gauge needles that simplify administration and can minimize concerns of patients with needle phobia. Exenatide QW is available as a system that requires assembly, after which the dose must be promptly administered. People with vision problems or limited manual dexterity, such as those with arthritis, may find assembling the exenatide QW system difficult.
Exenatide QW commonly causes a small lump at the injection site shortly after injection due to its microsphere formulation.65 Although the lump generally disappears within 3–4 weeks, its occurrence can be a concern to patients, particularly if they are not informed of this ahead of time. Injection site reactions suggesting an allergic reaction have been observed with each of the GLP-1 receptor agonists; when they occur, discontinuation is recommended.
Other differences among the GLP-1 receptor agonists relate to their glucose-lowering effects. The onset of glucose lowering occurs within a few days with exenatide BID and liraglutide and up to 2 weeks with exenatide QW.23,26,37,66,67 The slower onset of activity with exenatide QW results from a delay in the achievement of a blood concentration of exenatide within the therapeutic range until 2–5 weeks after initiation.37,67
Before initiating exenatide QW, it is important to inform patients that their blood glucose would not be expected to improve significantly until a few weeks after starting the therapy.25,42 If hyperglycemia is unacceptable, then a bridging therapy such as short-term basal insulin may be considered.
A1C reduction with GLP-1 receptor agonists
The results of randomized clinical trials (RCTs) involving these agents as monotherapy or in combination with one or more other glucose-lowering agents show a reduction in the A1C of 0.5–1.1% with exenatide BID, 1.5–2.0% with exenatide QW, and 0.5–1.5% with liraglutide.7,24,25,28,37,42,44,68–71 In five head-to-head RCTs with GLP-1 receptor agonists, important differences among the agents were observed from baseline to study end and are detailed in Table 3 and summarized in Table 4.7,37,43,65,70
Table 3.
Head-to-Head Comparisons of GLP-1 Receptor Agonists
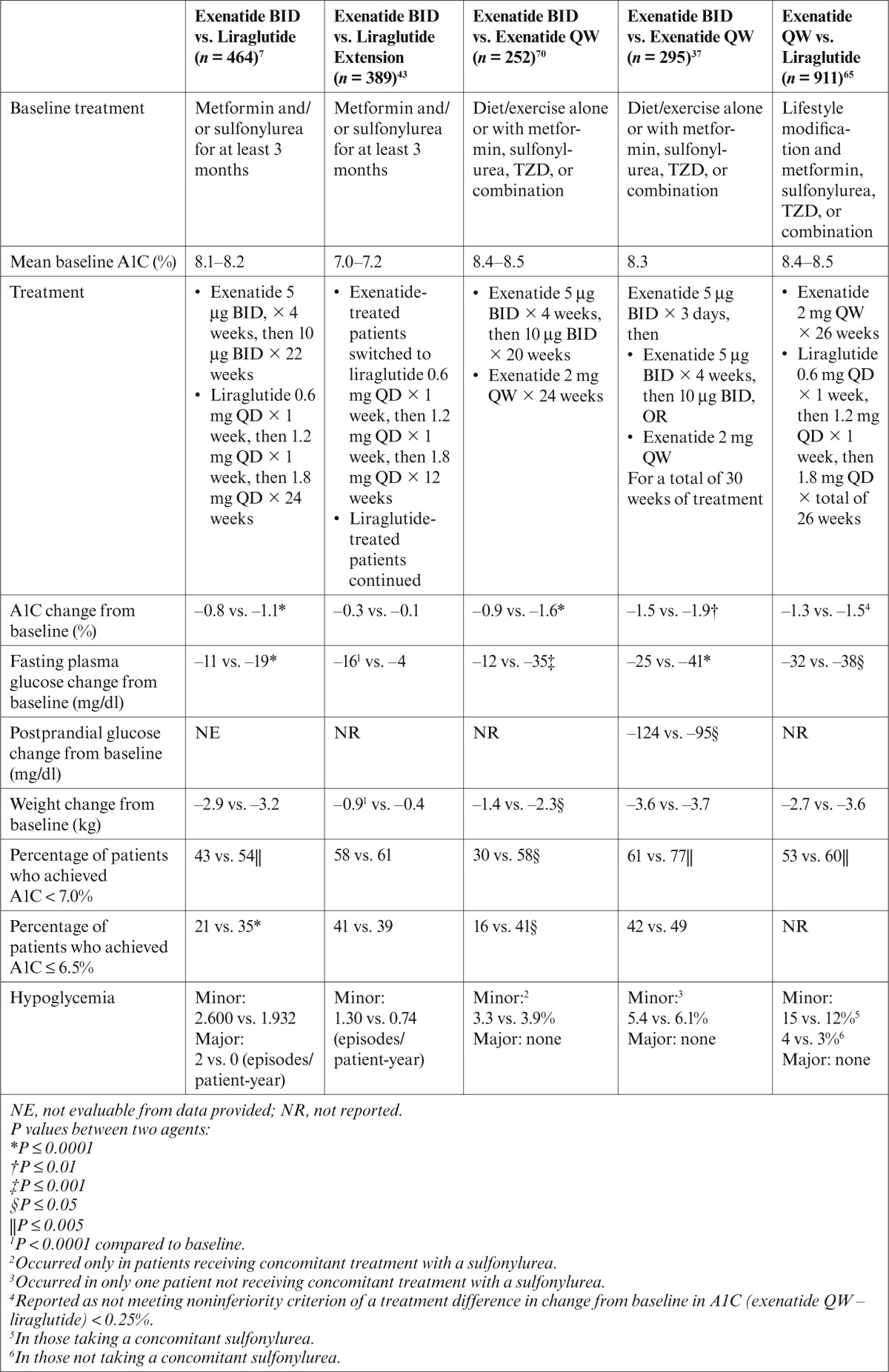
Table 4.
Summary of Significant Differences (P < 0.05) from Head-to-Head Comparisons of GLP-1 Receptor Agonists7,37,43,65,70
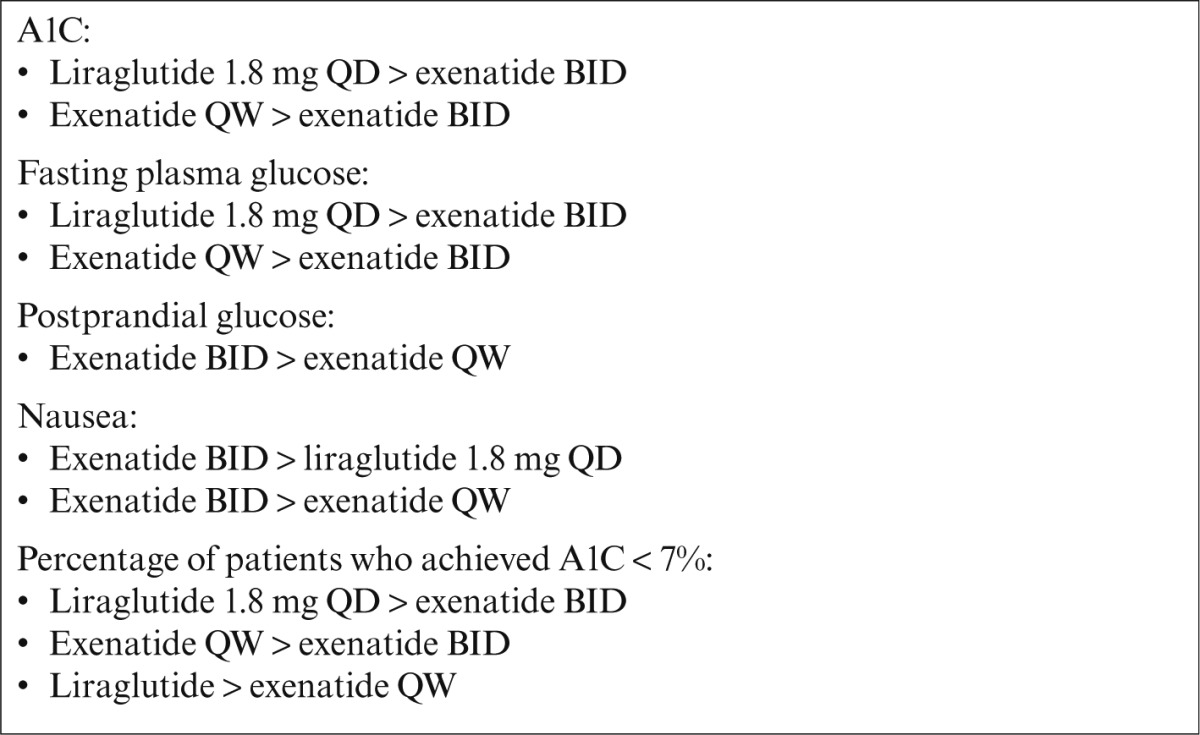
Significantly more patients treated with exenatide QW achieved an A1C of < 7% compared to exenatide BID, with a comparable incidence of minor hypoglycemia (events consistent with hypoglycemia with blood glucose < 54 mg/dl).37,70 In contrast, the incidence of minor and major hypoglycemia was slightly lower with liraglutide compared to exenatide BID and exenatide QW despite significantly more patients achieving an A1C of < 7% with liraglutide.7,43,65
These latter findings are consistent with the results of a prespecified meta-analysis of seven trials evaluating liraglutide with other glucose-lowering agents.72 At 26 weeks, the composite endpoint of A1C < 7%, no hypoglycemia, and no weight gain was observed in 40% of those treated with liraglutide 1.8 mg and 32% of those with liraglutide 1.2 mg compared to 25% of those treated with exenatide BID, 15% with insulin glargine, 8% with glimepiride, 11% with sitagliptin, and 8% with placebo.72
These head-to-head trials also generally showed a weight loss of 1–4 kg with GLP-1 receptor agonists. In addition, only two episodes of major hypoglycemia requiring the assistance of another person were observed, both in patients treated with exenatide BID; minor hypoglycemia was infrequent.7,37,43,65,70
Weight loss with GLP-1 receptor agonists
The average weight loss of 1–4 kg observed in the head-to-head trials is consistent with other clinical trials showing that weight loss is experienced by > 80% of people with type 2 diabetes who are treated with a GLP-1 receptor agonist.15,23,26,44,46,47 Although not all patients lose weight, most of those who do not still experience improvement in their glycemic profile.
A meta-analysis of seven 26-week phase 3 clinical trials involving liraglutide showed that weight loss > 5% was experienced by 17.7% treated with liraglutide 1.2 mg, 24.4% with liraglutide 1.8 mg, 17.7% with exenatide BID, and 9.9% with placebo.73 Patients with a higher BMI (e.g., ≥ 30 kg/m2) experience the greatest loss of weight.15,73
Nausea has been investigated as a potential cause for weight loss, but this generally has not been shown to be a contributing factor.23,24,46,73 It is likely that weight loss results from the ability of GLP-1 receptor agonists to promote satiety and reduce caloric intake.39,74–76 Therefore, patients should be encouraged to stop eating when they feel full.
It is not uncommon for patients to focus on the weight loss effect of GLP-1 receptor agonists, and this can serve as a motivating factor for initiating and adhering to this therapy. It is, however, important to counsel patients that weight loss is an added benefit and that the primary reason for using this therapy is to lower the blood glucose.1,2 Counseling patients about the continued importance of positive lifestyle behaviors is also necessary.
Hypoglycemia risk with GLP-1 receptor agonists
The low risk of hypoglycemia with the GLP-1 receptor agonists is comparable to that of DPP-4 inhibitors, metformin, TZDs, and α-glucosidase inhibitors1,2,77 and is likely because of the glucose-dependent actions of GLP-1 receptor agonists. Although infrequent, most episodes of hypoglycemia associated with GLP-1 receptor agonist therapy are mild or moderate in severity.7,37,43,65,70
People who are at risk of GLP-1 receptor agonist–related hypoglycemia are generally the same as those at risk of hypoglycemia from other glucose-lowering agents, including those with a longer duration of diabetes, who perform intensive physical exercise, or have kidney dysfunction or liver disease. People are also at risk of hypoglycemia when a GLP-1 receptor agonist is added to a secretagogue or insulin.37,67,69,71 Thus, the dose of the sulfonylurea, meglitinide, or insulin should be reduced and blood glucose closely monitored to minimize this risk.
It is important to periodically remind patients about the signs and symptoms of hypoglycemia and actions they should take if they occur. Inclusion of this information in a written action plan can be helpful. Family members and caregivers should also be familiar with the hypoglycemia action plan because they may be called upon to recognize and initially manage a hypoglycemic episode.
Individualizing GLP-1 Receptor Agonist Therapy
The largely self-managed nature of type 2 diabetes requires that management decisions be made in collaboration with each patient based on that patient’s needs, interests, and capabilities, as well as disease course.1,2,77 As these discussions take place, it is important to keep in mind that the evidence presented above comes from clinical trials and may not be generalizable to a real-world patient population. It is also important to keep in mind that data cited above are mean results and that results in individual patients will be different. That is, some patients will experience more and others less weight loss or A1C lowering than these mean results suggest. This is clearly demonstrated by the fact that patients with a baseline A1C ≥ 9–10% generally experience greater lowering of A1C greater than the mean.7,78
Because the A1C-lowering differences among the GLP-1 receptor agonists are relatively small, one of the key factors in selecting a specific agent in this class is the patient’s glycemic profile. If fasting plasma glucose is the primary target, exenatide QW or liraglutide are better choices, whereas exenatide BID would be a better choice if postprandial glucose is the primary target.
In addition to the glycemic profile, the selection of a GLP-1 receptor agonist may be affected by other patient-related factors. For example, most patients find it easy to remember to administer a medication in the morning, but some have difficulty remembering to administer a dose at dinnertime. If this is the case, the use of exenatide BID may be problematic, and liraglutide or exenatide QW may be better choices. Once-weekly administration of exenatide QW is often preferred over once-daily administration of liraglutide. For some, however, this preference may be offset by the need to assemble the administration kit for exenatide QW, the larger-gauge needle, or the small lumps that can occur at the injection site with this agent.
Another factor to consider is the slower onset of glycemic lowering with exenatide QW because this may compromise adherence when patients see only small changes in fasting and postprandial glucose over the first few weeks. If the delay in glycemic response with exenatide QW is an identified concern and symptoms of hyperglycemia are present, the addition of basal insulin to exenatide QW can be helpful to more quickly reduce symptoms and achieve glycemic control. Once symptoms have improved and glycemic control is achieved, it is generally possible to titrate down and discontinue the basal insulin.
These scenarios are examples of how multiple factors often affect the selection of a glucose-lowering therapy for an individual patient. By considering the differences among the GLP-1 receptor agonists outlined in Table 2, therapy may individualized to provide each patient with the best opportunity for successful self-management.
Strategies to Enhance Patient Motivation
Patient motivation is a key factor affecting self-management and should be a focus during patient follow-up appointments.77,79–81 It is important to revisit with patients the long-term goals established around the time of their diagnosis because this reminds patients of their broad goals for diabetes management.
Short-term goals should also be discussed because they are more specific and generally more easily addressed.82 Short-term goals may relate to any or all of patients’ blood glucose indicators (A1C, fasting, or postprandial), body weight, hypoglycemia, or other issues such as improving adherence or reducing some other barrier. The key is to find out what is most important to the patient in the near term and then help the patient arrive at a solution to achieve that goal.79,82
Patient motivation can often be improved by having patients compare how they felt at the time of their diagnosis to how they now feel. Patient motivation can also be enhanced by reminding patients of the benefits of their current therapies, especially as they relate to what is most important to each patient.83
Including discussion about the benefits of treatment options when changes to the treatment plan are being considered can also help to motivate patients.79 With respect to the GLP-1 receptor agonists, the likelihood of weight loss and the low incidence of hypoglycemia have been shown to enhance patient satisfaction.84–87 The limitations and side effects of treatment options should also be discussed because these are a major determinant of short- and long-term adherence.80
Patient motivation can also be enhanced by simply asking patients if they have any concerns or are experiencing any difficulties with their self-management.83 If they are, finding solutions with patients rather than for patients can serve to enhance motivation and improve adherence.79,82,88 Developing a written action plan can be particularly helpful to patients who may be overwhelmed or have specific concerns about a medication.
Keeping the treatment plan as simple as possible while achieving the treatment goals is an important management goal.80 In some cases, a less aggressive treatment plan that a patient is willing to accept is better in the short-term because it can instill more confidence and better motivate the patient for the long-term. It can also strengthen the patient-physician relationship, which can be very helpful moving forward.
Logistical and Team Support
Discussing management issues with patients and providing education takes time in the short term but can reduce future problems and improve adherence, as well as possibly shorten office visits.80,89 Some of these discussions, as well as much of the ongoing support and follow-up, can be provided by staff or other health care professionals outside of the practice.83,90 It is important that those who provide these functions be appropriately trained and able to offer information and education that is appropriate for each patient’s level of understanding.90–93 Staff must be adequately trained regarding administration devices and techniques for GLP-1 receptor agonists because there are significant differences in these for the different agents.
Strategies for Specific Issues
Responders and nonresponders
Most patients treated with a GLP-1 receptor agonist experience a reduction in A1C. Some patients, however, do not achieve glycemic benefit. Possible reasons for not responding to GLP-1 receptor agonist therapy include nonadherence, severity of disease (i.e., more advanced pancreatic β-cell dysfunction), antibody formation, and genetic factors (e.g., different variants of proteins such as TCF7L2 that may be involved in GLP-1 signaling).
Patients should be questioned about their adherence. If poor adherence is identified, determining the causes is important so that a solution acceptable to the patient is identified and agreed upon.
A less likely reason for a patient not achieving glycemic benefit is the formation of antibodies leading to the attenuation of the glycemic response in some patients, particularly those with high titers resulting from exenatide BID or exenatide QW. In most patients treated with a GLP-1 receptor agonist, antibody titers are low and do not affect the glycemic response.94,95
Because measurement of GLP-1 receptor agonist antibodies is not routinely available in clinical practice, switching from one agent to another in this class is an option for those not responding. In patients with anti-exenatide antibodies, switching from exenatide BID to liraglutide has been shown to result in further glycemic reduction.95 For patients who do not achieve adequate glycemic control with a GLP-1 receptor agonist as monotherapy or in combination with metformin, adding a third oral glucose-lowering agent or basal insulin are options as recommended by current guidelines.1,2
Nausea and vomiting
Although nausea and vomiting are transient in most patients treated with a GLP-1 receptor agonist,7,65 it is important that these side effects be discussed with patients before initiating therapy. It is also important to keep in mind that some patients with type 2 diabetes have impaired satiety mechanisms that prevent them from feeling full despite overeating. After initiating this therapy, such patients may begin to experience a feeling of fullness that they may confuse with gastrointestinal discomfort and nausea.
Because nausea and vomiting are common, particularly with exenatide BID, patients should be provided with strategies to minimize their occurrence or to reduce their severity should they occur. The most commonly employed strategy is to initiate therapy with exenatide BID or liraglutide using a dose-escalation regimen; there is no dose-escalation plan for exenatide QW because nausea is minimal with that agent (Table 2).
However, should nausea occur, the dose of exenatide QW can be held until nausea improves. The only dose of exenatide QW is 2 mg once weekly.96 Exenatide BID should be initiated at a dose of 5 μg twice daily and taken within 60 minutes before the morning and evening meals. The dose of exenatide BID can be increased to 10 μg twice daily after 1 month based on patient tolerability.97 Liraglutide should be initiated at a dose of 0.6 mg once daily for 1 week and then increased to 1.2 mg once daily.98 If the 1.2 mg dose does not result in acceptable glycemic control, it can be increased to 1.8 mg once daily to achieve glycemic control.
If nausea or vomiting occur during dose escalation of exenatide BID or liraglutide, there are several strategies patients can implement.99–101 First, all patients should be advised to stop eating when they feel full and to eat smaller meals, as well as to avoid high-fat meals. Second, the dose of exenatide BID can be taken closer to mealtime. Third, the time over which the dose of exenatide BID or liraglutide is escalated can be prolonged; this strategy is not applicable to exenatide QW. Alternatively, the dose can be temporarily reduced until the nausea or vomiting subside and then increased.
For patients treated with a combination of metformin and a GLP-1 receptor agonist, lowering the dose of metformin is often effective in reducing nausea. Switching from one GLP-1 receptor agonist to another is also an option because some patients who experienced persistent nausea with exenatide BID were able to tolerate exenatide QW or liraglutide.43,71 Switching to exenatide QW might be another option because this agent is the least likely of the three to cause nausea.37,65
Another alternative is to premedicate with oral antiemetics for up to 1–2 weeks. Combined use of open-label oral metoclopramide 10 mg with ondansetron 8 mg 30 minutes before administration of a single 10-μg dose of exenatide in healthy subjects (n = 120) resulted in a significant reduction in nausea (16.7 vs. 61.7%) and vomiting (6.7 vs. 38.3%) over 1 day compared to patients who received no antiemetic therapy, respectively.102
Cost considerations
The cost of medications continues to be an important issue for patients, especially as insurance plans change and deductibles and copays increase, thereby increasing patients’ out-of-pocket costs. Although discussing costs with patients can be uncomfortable, patients are often relieved to talk about medication costs when discussing treatment options rather than finding out that they cannot afford a given medication when they have the prescription filled. Discussion related to the cost of a medication also provides an opportunity to investigate patients’ insurance and copays, as well as medication assistance programs through manufacturers or government agencies.
Conclusion
Therapies that act on the incretin system have become important treatment options for patients with type 2 diabetes. Differences between GLP-1 receptor agonists and DPP-4 inhibitors, as well differences among the agents in the GLP-1 receptor agonist class, provide important opportunities to individualize therapy in patients over time.
In general, GLP-1 receptor agonists have a major advantage over other secretagogues because they are associated with a low risk of hypoglycemia. These agents are a better choice than DPP-4 inhibitors if greater A1C lowering is needed. Concerns about injections are usually mitigated by a quick demonstration by the medical provider, nurse, or medical assistant. Although the weight loss effect of GLP-1 receptor agonists can help motivate patients to take these medications, this effect is enhanced by positive lifestyle behaviors.
By considering the benefits, limitations, and actual costs to patients and integrating evidence from clinical trials with clinical experience, diabetes care providers can employ GLP-1 receptor agonists and DPP-4 inhibitors effectively to individualize therapy in patients with type 2 diabetes.
ACKNOWLEDGMENTS
Funding for the development of this article was provided by Novo Nordisk to the Primary Care Education Consortium, which provided editorial assistance to the author. The author received no financial compensation for this article. The author independently made the decision to submit this article and is solely responsible for all content.
REFERENCES
- 1.Garber AJ, Abrahamson MJ, Barzilay JI, Blonde L, Bloomgarden ZT, Bush MA, Dagogo-Jack S, Davidson MB, Einhorn D, Garvey WT, Grunberger G, Handelsman Y, Hirsch IB, Jellinger PS, McGill JB, Mechanick JI, Rosenblit PD, Umpierrez GE, Davidson MH: American Association of Clinical Endocrinologists’ comprehensive diabetes management algorithm 2013 consensus statement. Endocr Pract 19:1–48, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, Peters AL, Tsapas A, Wender R, Matthews DR: Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 35:1364–1379, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kreymann B, Williams G, Ghatei MA, Bloom SR: Glucagon-like peptide-1 7–36: a physiological incretin in man. Lancet 2:1300–1304, 1987 [DOI] [PubMed] [Google Scholar]
- 4.Fehmann HC, Habener JF: Insulinotropic hormone glucagon-like peptide-1 (7–37) stimulation of proinsulin gene expression and proinsulin biosynthesis in insulinoma beta TC-1 cells. Endocrinology 130:159–166, 1992 [DOI] [PubMed] [Google Scholar]
- 5.Naslund E, Bogefors J, Skogar S, Gryback P, Jacobsson H, Holst JJ, Hellstrom PM: GLP-1 slows solid gastric emptying and inhibits insulin, glucagon, and PYY release in humans. Am J Physiol 277:R910–R916, 1999 [DOI] [PubMed] [Google Scholar]
- 6.Nauck MA, Heimesaat MM, Behle K, Holst JJ, Nauck MS, Ritzel R, Hufner M, Schmiegel WH: Effects of glucagon-like peptide 1 on counterregulatory hormone responses, cognitive functions, and insulin secretion during hyperinsulinemic, stepped hypoglycemic clamp experiments in healthy volunteers. J Clin Endocrinol Metab 87:1239–1246, 2002 [DOI] [PubMed] [Google Scholar]
- 7.Buse JB, Rosenstock J, Sesti G, Schmidt WE, Montanya E, Brett JH, Zychma M, Blonde L: Liraglutide once a day versus exenatide twice a day for type 2 diabetes: a 26-week randomised, parallel-group, multinational, open-label trial (LEAD-6). Lancet 374:39–47, 2009 [DOI] [PubMed] [Google Scholar]
- 8.Karagianis J: Understanding and teaching key concepts and tools of evidence-based medicine: perspectives of a clinician-researcher pharmaceutical physician. Clin Ther 33:B3–B10, 2011 [DOI] [PubMed] [Google Scholar]
- 9.Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS: Evidence-based medicine: what it is and what it isn’t. BMJ 312:71–72, 1996 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Citrome L: Evidence-based medicine: it’s not just about the evidence. Int J Clin Pract 65:634–635, 2011 [DOI] [PubMed] [Google Scholar]
- 11.Groff MW: How to incorporate clinical experience into evidence-based medicine. Clin Neurosurg 56:54–56, 2009 [PubMed] [Google Scholar]
- 12.Morales J: The pharmacologic basis for clinical differences among GLP-1 receptor agonists and DPP-4 inhibitors. Postgrad Med 123:189–201, 2011 [DOI] [PubMed] [Google Scholar]
- 13.Cobble M: Differentiating among incretin-based therapies in the management of patients with type 2 diabetes mellitus. Diabetol Metab Syndr 4:1–14, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Edwards KL, Stapleton M, Weis J, Irons BK: An update in incretin-based therapy: a focus on glucagon-like peptide-1 receptor agonists. Diabetes Technol Ther 14:951–967, 2012 [DOI] [PubMed] [Google Scholar]
- 15.Klonoff DC, Buse JB, Nielsen LL, Guan X, Bowlus CL, Holcombe JH, Wintle ME, Maggs DG: Exenatide effects on diabetes, obesity, cardiovascular risk factors and hepatic biomarkers in patients with type 2 diabetes treated for at least 3 years. Curr Med Res Opin 24:275–286, 2008 [DOI] [PubMed] [Google Scholar]
- 16.Garber A, Henry RR, Ratner R, Hale P, Chang CT, Bode B: Liraglutide, a once-daily human glucagon-like peptide-1 analogue, provides sustained improvements in glycaemic control and weight for 2 years as monotherapy compared with glimepiride in patients with type 2 diabetes. Diabetes Obes Metab 13:348–356, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nauck M, Frid A, Hermansen K, Thomsen AB, During M, Shah N, Tankova T, Mitha I, Matthews DR: Long-term efficacy and safety comparison of liraglutide, glimepiride and placebo, all in combination with metformin in type 2 diabetes: 2-year results from the LEAD-2 study. Diabetes Obes Metab 15:204–212, 2013 [DOI] [PubMed] [Google Scholar]
- 18.Chacra AR, Tan GH, Ravichandran S, List J, Chen R: Safety and efficacy of saxagliptin in combination with submaximal sulphonylurea versus up-titrated sulphonylurea over 76 weeks. Diab Vasc Dis Res 8:150–159, 2011 [DOI] [PubMed] [Google Scholar]
- 19.Pfutzner A, Paz-Pacheco E, Allen E, Frederich R, Chen R: Initial combination therapy with saxagliptin and metformin provides sustained glycaemic control and is well tolerated for up to 76 weeks. Diabetes Obes Metab 13:567–576, 2011 [DOI] [PubMed] [Google Scholar]
- 20.Gallwitz B, Rosenstock J, Rauch T, Bhattacharya S, Patel S, von Eynatten M, Dugi KA, Woerle HJ: 2-year efficacy and safety of linagliptin compared with glimepiride in patients with type 2 diabetes inadequately controlled on metformin: a randomised, double-blind, non-inferiority trial. Lancet 380:475–483, 2012 [DOI] [PubMed] [Google Scholar]
- 21.Inzucchi S, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, Peters AL, Tsapas A, Wender R, Matthews DR: Management of hyperglycemia in type 2 diabetes: a patient-centered approach: supplementary data [article online]. Diabetes Care. Electronically published; 19 April 2012 (doi:10.2337/dc12–0413/-/DC1) [Google Scholar]
- 22.DeFronzo RA, Ratner RE, Han J, Kim DD, Fineman MS, Baron AD: Effects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in metformin-treated patients with type 2 diabetes. Diabetes Care 28:1092–1100, 2005 [DOI] [PubMed] [Google Scholar]
- 23.Garber A, Henry R, Ratner R, Garcia-Hernandez PA, Rodriguez-Pattzi H, Olvera-Alvarez I, Hale PM, Zdravkovic M, Bode B: Liraglutide versus glimepiride monotherapy for type 2 diabetes (LEAD-3 Mono): a randomised, 52-week, phase III, double-blind, parallel-treatment trial. Lancet 373:473–481, 2009 [DOI] [PubMed] [Google Scholar]
- 24.Nauck M, Frid A, Hermansen K, Shah NS, Tankova T, Mitha IH, Zdravkovic M, During M, Matthews DR: Efficacy and safety comparison of liraglutide, glimepiride, and placebo, all in combination with metformin, in type 2 diabetes: the LEAD (liraglutide effect and action in diabetes)-2 study. Diabetes Care 32:84–90, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Russell-Jones D, Cuddihy RM, Hanefeld M, Kumar A, Gonzalez JG, Chan M, Wolka AM, Boardman MK: Efficacy and safety of exenatide once weekly versus metformin, pioglitazone, and sitagliptin used as monotherapy in drug-naive patients with type 2 diabetes (DURATION-4): a 26-week double-blind study. Diabetes Care 35:252–258, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Nelson P, Poon T, Guan X, Schnabel C, Wintle M, Fineman M: The incretin mimetic exenatide as a monotherapy in patients with type 2 diabetes. Diabetes Technol Ther 9:317–326, 2007 [DOI] [PubMed] [Google Scholar]
- 27.Moretto TJ, Milton DR, Ridge TD, Macconell LA, Okerson T, Wolka AM, Brodows RG: Efficacy and tolerability of exenatide monotherapy over 24 weeks in antidiabetic drug-naive patients with type 2 diabetes: a randomized, double-blind, placebo-controlled, parallel-group study. Clin Ther 30:1448–1460, 2008 [DOI] [PubMed] [Google Scholar]
- 28.Vilsboll T, Zdravkovic M, Le Thi T, Krarup T, Schmitz O, Courreges JP, Verhoeven R, Buganova I, Madsbad S: Liraglutide, a long-acting human glucagon-like peptide-1 analog, given as monotherapy significantly improves glycemic control and lowers body weight without risk of hypoglycemia in patients with type 2 diabetes. Diabetes Care 30:1608–1610, 2007 [DOI] [PubMed] [Google Scholar]
- 29.Taylor K, Gurney K, Han J, Pencek R, Walsh B, Trautmann M: Exenatide once weekly treatment maintained improvements in glycemic control and weight loss over 2 years. BMC Endocr Disord 11:1–9, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Raz I, Hanefeld M, Xu L, Caria C, Williams-Herman D, Khatami H: Efficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy in patients with type 2 diabetes mellitus. Diabetologia 49:2564–2571, 2006 [DOI] [PubMed] [Google Scholar]
- 31.Aschner P, Kipnes MS, Lunceford JK, Sanchez M, Mickel C, Williams-Herman DE: Effect of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy on glycemic control in patients with type 2 diabetes. Diabetes Care 29:2632–2637, 2006 [DOI] [PubMed] [Google Scholar]
- 32.Rosenstock J, Aguilar-Salinas C, Klein E, Nepal S, List J, Chen R: Effect of saxagliptin monotherapy in treatment-naive patients with type 2 diabetes. Curr Med Res Opin 25:2401–2411, 2009 [DOI] [PubMed] [Google Scholar]
- 33.Rosenstock J, Sankoh S, List JF: Glucose-lowering activity of the dipeptidyl peptidase-4 inhibitor saxagliptin in drug-naive patients with type 2 diabetes. Diabetes Obes Metab 10:376–386, 2008 [DOI] [PubMed] [Google Scholar]
- 34.Del Prato S, Barnett AH, Huisman H, Neubacher D, Woerle HJ, Dugi KA: Effect of linagliptin monotherapy on glycaemic control and markers of beta-cell function in patients with inadequately controlled type 2 diabetes: a randomized controlled trial. Diabetes Obes Metab 13:258–267, 2011 [DOI] [PubMed] [Google Scholar]
- 35.Holst JJ, Deacon CF: Glucagon-like peptide-1 mediates the therapeutic actions of DPP-IV inhibitors. Diabetologia 48:612–615, 2005 [DOI] [PubMed] [Google Scholar]
- 36.Herman GA, Bergman A, Stevens C, Kotey P, Yi B, Zhao P, Dietrich B, Golor G, Schrodter A, Keymeulen B, Lasseter KC, Kipnes MS, Snyder K, Hilliard D, Tanen M, Cilissen C, De Smet M, de Lepeleire I, Van Dyck K, Wang AQ, Zeng W, Davies MJ, Tanaka W, Holst JJ, Deacon CF, Gottesdiener KM, Wagner JA: Effect of single oral doses of sitagliptin, a dipeptidyl peptidase-4 inhibitor, on incretin and plasma glucose levels after an oral glucose tolerance test in patients with type 2 diabetes. J Clin Endocrinol Metab 91:4612–4619, 2006 [DOI] [PubMed] [Google Scholar]
- 37.Drucker DJ, Buse JB, Taylor K, Kendall DM, Trautmann M, Zhuang D, Porter L: Exenatide once weekly versus twice daily for the treatment of type 2 diabetes: a randomised, open-label, non-inferiority study. Lancet 372:1240–1250, 2008 [DOI] [PubMed] [Google Scholar]
- 38.Delgado-Aros S, Kim DY, Burton DD, Thomforde GM, Stephens D, Brinkmann BH, Vella A, Camilleri M: Effect of GLP-1 on gastric volume, emptying, maximum volume ingested, and postprandial symptoms in humans. Am J Physiol Gastrointest Liver Physiol 282:G424–G431, 2002 [DOI] [PubMed] [Google Scholar]
- 39.DeFronzo RA, Okerson T, Viswanathan P, Guan X, Holcombe JH, MacConell L: Effects of exenatide versus sitagliptin on postprandial glucose, insulin and glucagon secretion, gastric emptying, and caloric intake: a randomized, cross-over study. Curr Med Res Opin 24:2943–2952, 2008 [DOI] [PubMed] [Google Scholar]
- 40.Arnolds S, Dellweg S, Clair J, Dain MP, Nauck MA, Rave K, Kapitza C: Further improvement in postprandial glucose control with addition of exenatide or sitagliptin to combination therapy with insulin glargine and metformin: a proof-of-concept study. Diabetes Care 33:1509–1515, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Pratley RE, Nauck M, Bailey T, Montanya E, Cuddihy R, Filetti S, Thomsen AB, Sondergaard RE, Davies M: Liraglutide versus sitagliptin for patients with type 2 diabetes who did not have adequate glycaemic control with metformin: a 26-week, randomised, parallel-group, open-label trial. Lancet 375:1447–1456, 2010 [DOI] [PubMed] [Google Scholar]
- 42.Bergenstal RM, Wysham C, MacConell L, Malloy J, Walsh B, Yan P, Wilhelm K, Malone J, Porter LE: Efficacy and safety of exenatide once weekly versus sitagliptin or pioglitazone as an adjunct to metformin for treatment of type 2 diabetes (DURATION-2): a randomised trial. Lancet 376:431–439, 2010 [DOI] [PubMed] [Google Scholar]
- 43.Buse JB, Sesti G, Schmidt WE, Montanya E, Chang CT, Xu Y, Blonde L, Rosenstock J: Switching to once-daily liraglutide from twice-daily exenatide further improves glycemic control in patients with type 2 diabetes using oral agents. Diabetes Care 33:1300–1303, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Blonde L, Klein EJ, Han J, Zhang B, Mac SM, Poon TH, Taylor KL, Trautmann ME, Kim DD, Kendall DM: Interim analysis of the effects of exenatide treatment on A1C, weight and cardiovascular risk factors over 82 weeks in 314 overweight patients with type 2 diabetes. Diabetes Obes Metab 8:436–447, 2006 [DOI] [PubMed] [Google Scholar]
- 45.Zinman B, Hoogwerf BJ, Garcia SD, Milton DR, Giaconia JM, Kim DD, Trautmann ME, Brodows RG: The effect of adding exenatide to a thiazolidinedione in suboptimally controlled type 2 diabetes: a randomized trial. Ann Intern Med 146:477–485, 2007 [DOI] [PubMed] [Google Scholar]
- 46.Russell-Jones D, Vaag A, Schmitz O, Sethi BK, Lalic N, Antic S, Zdravkovic M, Ravn GM, Simo R: Liraglutide vs insulin glargine and placebo in combination with metformin and sulfonylurea therapy in type 2 diabetes mellitus (LEAD-5 met+SU): a randomised controlled trial. Diabetologia 52:2046–2055, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Zinman B, Gerich J, Buse JB, Lewin A, Schwartz S, Raskin P, Hale PM, Zdravkovic M, Blonde L: Efficacy and safety of the human glucagon-like peptide-1 analog liraglutide in combination with metformin and thiazolidinedione in patients with type 2 diabetes (LEAD-4 Met+TZD). Diabetes Care 32:1224–1230, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Nauck MA, Duran S, Kim D, Johns D, Northrup J, Festa A, Brodows R, Trautmann M: A comparison of twice-daily exenatide and biphasic insulin aspart in patients with type 2 diabetes who were suboptimally controlled with sulfonylurea and metformin: a non-inferiority study. Diabetologia 50:259–267, 2007 [DOI] [PubMed] [Google Scholar]
- 49.Taskinen MR, Rosenstock J, Tamminen I, Kubiak R, Patel S, Dugi KA, Woerle HJ: Safety and efficacy of linagliptin as add-on therapy to metformin in patients with type 2 diabetes: a randomized, double-blind, placebo-controlled study. Diabetes Obes Metab 13:65–74, 2011 [DOI] [PubMed] [Google Scholar]
- 50.Yanai H, Adachi H, Hamasaki H, Masui Y, Yoshikawa R, Moriyama S, Mishima S, Sako A: Effects of 6-month sitagliptin treatment on glucose and lipid metabolism, blood pressure, body weight and renal function in type 2 diabetic patients: a chart-based analysis. J Clin Med Res 4:251–258, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Ogawa S, Ishiki M, Nako K, Okamura M, Senda M, Mori T, Ito S: Sitagliptin, a dipeptidyl peptidase-4 inhibitor, decreases systolic blood pressure in Japanese hypertensive patients with type 2 diabetes. Tohoku J Exp Med 223:133–135, 2011 [DOI] [PubMed] [Google Scholar]
- 52.Scott R, Wu M, Sanchez M, Stein P: Efficacy and tolerability of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy over 12 weeks in patients with type 2 diabetes. Int J Clin Pract 61:171–180, 2007 [DOI] [PubMed] [Google Scholar]
- 53.Hollander P, Li J, Allen E, Chen R: Saxagliptin added to a thiazolidinedione improves glycemic control in patients with type 2 diabetes and inadequate control on thiazolidinedione alone. J Clin Endocrinol Metab 94:4810–4819, 2009 [DOI] [PubMed] [Google Scholar]
- 54.Butler PC, Elashoff M, Elashoff R, Gale EA: A critical analysis of the clinical use of incretin-based therapies: are the GLP-1 therapies safe? Diabetes Care 36:2118–2125, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Nauck MA: A critical analysis of the clinical use of incretin-based therapies: the benefits by far outweigh the potential risks. Diabetes Care 36:2126–2132, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.U.S. Food and Drug Administration: Tradjenta NDA Approval [article online], 2011. Available from http://www.accessdata.fda.gov/drugsatfda_docs/appletter/2011/201280s000ltr.pdf. Accessed 22 August 2013.
- 57.Parks M, Rosebraugh C: Weighing risks and benefits of liraglutide: the FDA’s review of a new antidiabetic therapy. N Engl J Med 362:774–777, 2010 [DOI] [PubMed] [Google Scholar]
- 58.U.S. Food and Drug Administration: Byetta NDA approval. Supplemental approval [article online], 2009. Available from http://www.accessdata.fda.gov/drugs atfda_docs/appletter/2009/021773s009s011s017s018s022s025021919ltr.pdf. Accessed 22 August 2013.
- 59.U.S. Food and Drug Administration: Bydureon NDA approval [article online], 2012. Available from http://www.accessdata.fda.gov/drugsatfda_docs/appletter/2012/022200s000ltr.pdf. Accessed 22 August 2013.
- 60.U.S. Food and Drug Administration: Victoza NDA approval [article online], 2010. Available from http://www.accessdata.fda.gov/drugsatfda_docs/appletter/2010/022341s000ltr.pdf. Accessed 22 August 2013.
- 61.U.S. Food and Drug Administration: Januvia Supplement approval [article online], 2010. Available from http://www.accessdata.fda.gov/drugsatfda_docs/appletter/2010/021995s010s011s012s014ltr.pdf. Accessed 22 August 2013.
- 62.Drucker DJ, Sherman SI, Bergenstal RM, Buse JB: The safety of incretin-based therapies: review of the scientific evidence. J Clin Endocrinol Metab 96:2027–2031, 2011 [DOI] [PubMed] [Google Scholar]
- 63.Knudsen LB, Madsen LW, Andersen S, Almholt K, de Boer AS, Drucker DJ, Gotfredsen C, Egerod FL, Hegelund AC, Jacobsen H, Jacobsen SD, Moses AC, Molck AM, Nielsen HS, Nowak J, Solberg H, Thi TD, Zdravkovic M: Glucagon-like peptide-1 receptor agonists activate rodent thyroid C-cells causing calcitonin release and C-cell proliferation. Endocrinology 151:1473–1486, 2010 [DOI] [PubMed] [Google Scholar]
- 64.U.S. Food and Drug Administration: Onglyza NDA approval [article online], 2009. Available from http://www.accessdata.fda.gov/drugsatfda_docs/appletter/2009/022350s000ltr.pdf. Accessed 22 August 2013.
- 65.Buse JB, Nauck M, Forst T, Sheu WH, Shenouda SK, Heilmann CR, Hoogwerf BJ, Gao A, Boardman MK, Fineman M, Porter L, Schernthaner G: Exenatide once weekly versus liraglutide once daily in patients with type 2 diabetes (DURATION-6): a randomised, open-label study. Lancet 381:117–124, 2013 [DOI] [PubMed] [Google Scholar]
- 66.Gallwitz B, Vaag A, Falahati A, Madsbad S: Adding liraglutide to oral antidiabetic drug therapy: onset of treatment effects over time. Int J Clin Pract 64:267–276, 2010 [DOI] [PubMed] [Google Scholar]
- 67.Iwamoto K, Nasu R, Yamamura A, Kothare PA, Mace K, Wolka AM, Linnebjerg H: Safety, tolerability, pharmacokinetics, and pharmacodynamics of exenatide once weekly in Japanese patients with type 2 diabetes. Endocr J 56:951–962, 2009 [DOI] [PubMed] [Google Scholar]
- 68.Buse JB, Henry RR, Han J, Kim DD, Fineman MS, Baron AD: Effects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes. Diabetes Care 27:2628–2635, 2004 [DOI] [PubMed] [Google Scholar]
- 69.Marre M, Shaw J, Brandle M, Bebakar WM, Kamaruddin NA, Strand J, Zdravkovic M, Le Thi TD, Colagiuri S: Liraglutide, a once-daily human GLP-1 analogue, added to a sulphonylurea over 26 weeks produces greater improvements in glycaemic and weight control compared with adding rosiglitazone or placebo in subjects with type 2 diabetes (LEAD-1 SU). Diabet Med 26:268–278, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Blevins T, Pullman J, Malloy J, Yan P, Taylor K, Schulteis C, Trautmann M, Porter L: DURATION-5: exenatide once weekly resulted in greater improvements in glycemic control compared with exenatide twice daily in patients with type 2 diabetes. J Clin Endocrinol Metab 96:1301–1310, 2011 [DOI] [PubMed] [Google Scholar]
- 71.Buse JB, Drucker DJ, Taylor KL, Kim T, Walsh B, Hu H, Wilhelm K, Trautmann M, Shen LZ, Porter LE: DURATION-1: exenatide once weekly produces sustained glycemic control and weight loss over 52 weeks. Diabetes Care 33:1255–1261, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Zinman B, Schmidt WE, Moses A, Lund N, Gough S: Achieving a clinically relevant composite outcome of an HbA1c of < 7% without weight gain or hypoglycaemia in type 2 diabetes: a meta-analysis of the liraglutide clinical trial programme. Diabetes Obes Metab 14:77–82, 2012 [DOI] [PubMed] [Google Scholar]
- 73.Niswender K, Pi-Sunyer X, Buse J, Jensen KH, Toft AD, Russell-Jones D, Zinman B: Weight change with liraglutide and comparator therapies: an analysis of seven phase 3 trials from the liraglutide diabetes development programme. Diabetes Obes Metab 15:42–54, 2013 [DOI] [PubMed] [Google Scholar]
- 74.Gutzwiller JP, Goke B, Drewe J, Hildebrand P, Ketterer S, Handschin D, Winterhalder R, Conen D, Beglinger C: Glucagon-like peptide-1: a potent regulator of food intake in humans. Gut 44:81–86, 1999 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Gutzwiller JP, Drewe J, Goke B, Schmidt H, Rohrer B, Lareida J, Beglinger C: Glucagon-like peptide-1 promotes satiety and reduces food intake in patients with diabetes mellitus type 2. Am J Physiol 276:R1541–R1544, 1999 [DOI] [PubMed] [Google Scholar]
- 76.Zander M, Madsbad S, Madsen JL, Holst JJ: Effect of 6-week course of glucagon-like peptide 1 on glycaemic control, insulin sensitivity, and beta-cell function in type 2 diabetes: a parallel-group study. Lancet 359:824–830, 2002 [DOI] [PubMed] [Google Scholar]
- 77.American Diabetes Association : Standards of medical care in diabetes—2013. Diabetes Care 36 (Suppl. 1):S11–S66, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Kendall DM, Riddle MC, Rosenstock J, Zhuang D, Kim DD, Fineman MS, Baron AD: Effects of exenatide (exendin-4) on glycemic control over 30 weeks in patients with type 2 diabetes treated with metformin and a sulfonylurea. Diabetes Care 28:1083–1091, 2005 [DOI] [PubMed] [Google Scholar]
- 79.Funnell MM, Anderson RM: Empowerment and self-management of diabetes. Clinical Diabetes 22:123–127, 2004 [Google Scholar]
- 80.Brunton SA: Improving medication adherence in chronic disease management. J Fam Pract 60:S1–S8, 2011 [PubMed] [Google Scholar]
- 81.Nadkarni A, Kucukarslan SN, Bagozzi RP, Yates JF, Erickson SR: Examining determinants of self management behaviors in patients with diabetes: an application of the Theoretical Model of Effortful Decision Making and Enactment. Patient Educ Couns 85:148–153, 2011 [DOI] [PubMed] [Google Scholar]
- 82.Funnell MM: Physician-patient communication in diabetes care: focus on injectables. J Fam Pract 60:S29–S31, 2011 [PubMed] [Google Scholar]
- 83.Funnell MM: Overcoming barriers to the initiation of insulin therapy. Clinical Diabetes 25:36–38, 2007 [Google Scholar]
- 84.Lind M, Jendle J, Torffvit O, Lager I: Glucagon-like peptide 1 (GLP-1) analogue combined with insulin reduces HbA1c and weight with low risk of hypoglycemia and high treatment satisfaction. Prim Care Diabetes 6:41–46, 2012 [DOI] [PubMed] [Google Scholar]
- 85.Jose B, Tahrani AA, Piya MK, Barnett AH: Exenatide once weekly: clinical outcomes and patient satisfaction. Patient Prefer Adherence 4:313–324, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Best JH, Boye KS, Rubin RR, Cao D, Kim TH, Peyrot M: Improved treatment satisfaction and weight-related quality of life with exenatide once weekly or twice daily. Diabet Med 26:722–728, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Hermansen K, Kolotkin RL, Hammer M, Zdravkovic M, Matthews D: Patient-reported outcomes in patients with type 2 diabetes treated with liraglutide or glimepiride, both as add-on to metformin. Prim Care Diabetes 4:113–117, 2010 [DOI] [PubMed] [Google Scholar]
- 88.Hill-Briggs F, Lazo M, Peyrot M, Doswell A, Chang YT, Hill MN, Levine D, Wang NY, Brancati FL: Effect of problem-solving-based diabetes self-management training on diabetes control in a low income patient sample. J Gen Intern Med 26:972–978, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Levinson W, Gorawara-Bhat R, Lamb J: A study of patient clues and physician responses in primary care and surgical settings. JAMA 284:1021–1027, 2000 [DOI] [PubMed] [Google Scholar]
- 90.Haas L, Maryniuk M, Beck J, Cox CE, Duker P, Edwards L, Fisher EB, Hanson L, Kent D, Kolb L, McLaughlin S, Orzeck E, Piette JD, Rhinehart AS, Rothman R, Sklaroff S, Tomky D, Youssef G: National standards for diabetes self-management education and support. Diabetes Care 36 (Suppl. 1):S100–S108, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Brega AG, Ang A, Vega W, Jiang L, Beals J, Mitchell CM, Moore K, Manson SM, Acton KJ, Roubideaux Y: Mechanisms underlying the relationship between health literacy and glycemic control in American Indians and Alaska Natives. Patient Educ Couns 88:61–68, 2012 [DOI] [PubMed] [Google Scholar]
- 92.Rothman R, Malone R, Bryant B, Horlen C, Dewalt D, Pignone M: The relationship between literacy and glycemic control in a diabetes disease-management program. Diabetes Educ 30:263–273, 2004 [DOI] [PubMed] [Google Scholar]
- 93.Ishikawa H, Yano E: The relationship of patient participation and diabetes outcomes for patients with high vs. low health literacy. Patient Educ Couns 84:393–397, 2011 [DOI] [PubMed] [Google Scholar]
- 94.Fineman MS, Mace KF, Diamant M, Darsow T, Cirincione BB, Booker Porter TK, Kinninger LA, Trautmann ME: Clinical relevance of anti-exenatide antibodies: safety, efficacy and cross-reactivity with long-term treatment. Diabetes Obes Metab 14:546–554, 2012 [DOI] [PubMed] [Google Scholar]
- 95.Buse JB, Garber A, Rosenstock J, Schmidt WE, Brett JH, Videbaek N, Holst J, Nauck M: Liraglutide treatment is associated with a low frequency and magnitude of antibody formation with no apparent impact on glycemic response or increased frequency of adverse events: results from the Liraglutide Effect and Action in Diabetes (LEAD) trials. J Clin Endocrinol Metab 96:1695–1702, 2011 [DOI] [PubMed] [Google Scholar]
- 96.Amylin Pharmaceuticals : Bydureon package insert. San Diego, Calif., Amylin Pharmaceuticals, February 2013 [Google Scholar]
- 97.Amylin Pharmaceuticals : Byetta package insert. San Diego, Calif., Amylin Pharmaceuticals, December 2011 [Google Scholar]
- 98.Novo Nordisk : Victoza package insert. Princeton, N.J., Novo Nordisk, April 2013 [Google Scholar]
- 99.Cobble ME: How to implement incretin therapy. J Fam Pract 57:S26–S31, 2008 [PubMed] [Google Scholar]
- 100.Freeman JS: Optimizing outcomes for GLP-1 agonists. J Am Osteopath Assoc 111:eS15–eS20, 2011 [PubMed] [Google Scholar]
- 101.Unger JR, Parkin CG: Glucagon-like peptide-1 (GLP-1) receptor agonists: differentiating the new medications. Diabetes Ther 2:29–39, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Ellero C, Han J, Bhavsar S, Cirincione BB, Deyoung MB, Gray AL, Yushmanova I, Anderson PW: Prophylactic use of anti-emetic medications reduced nausea and vomiting associated with exenatide treatment: a retrospective analysis of an open-label, parallel-group, single-dose study in healthy subjects. Diabet Med 27:1168–1173, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]