

Abstract
Background
There currently is a need for a non-invasive measure of renal fibrosis. We aim to explore whether shear wave elastography (SWE)-derived estimates of tissue stiffness may serve as a non-invasive biomarker that can distinguish normal and abnormal renal parenchymal tissue.
Methods
Participants with CKD (by estimated GFR) and healthy volunteers underwent SWE. Renal elasticity was estimated as Young’s modulus (YM) in kilopascals (kPa). Univariate Wilcoxon rank-sum tests were used.
Results
Twenty-five participants with CKD (median GFR 38 mL/min; quartile 1, quartile 3 28, 42) and 20 healthy controls without CKD underwent SWE performed by a single radiologist. CKD was associated with increased median YM (9.40 [5.55, 22.35] vs. 4.40 [3.68, 5.70] kPa; p = 0.002) and higher median intra-subject inter-measurement estimated YM’s variability (4.27 [2.89, 9.90] vs. 1.51 [1.21, 2.05] kPa; p < 0.001).
Conclusions
SWE-derived estimates of renal stiffness and intra-subject estimated stiffness variability are higher in patients with CKD than in healthy controls. Renal fibrosis is a plausible explanation for the observed difference in YM. Further studies are required to determine the relationship between YM, estimated renal stiffness, and renal fibrosis severity.
Electronic supplementary material
The online version of this article (doi:10.1186/s12882-015-0120-7) contains supplementary material, which is available to authorized users.
Keywords: Chronic kidney disease, Stiffness, Fibrosis, Shear wave elastography, Ultrasound
Background
Chronic kidney disease (CKD) is a major public health challenge [1]. There are currently 19 million adults in the US in early stages of CKD and over 640,000 adults with end stage renal disease (ESRD) [2–4]. Projections suggest that the number of patients who will require dialysis or transplantation for kidney failure will rise to over 2 million people by 2030 [3, 4].
Advanced CKD is associated with increased morbidity and mortality [5]. Therefore, it is important to quantify CKD severity. Currently, CKD is staged based on estimated glomerular filtration rate (eGFR), derived from serum creatinine values in one of several formulas [2]. Limitations of this measure are well documented, including confounding by race, gender, and muscle mass [6].
Intra-renal fibrosis is a final common pathway for all CKD, with fibrosis degree correlated with disease severity [7–9]. Non-focal renal biopsy is the only method in current clinical use for the evaluation of intra-renal fibrosis. However, non-focal renal biopsy has significant disadvantages: (1) it is invasive, with risk of major complications, (2) it is expensive, with costs of greater than $1000 (US) per procedure, and (3) it is subject to sampling error, as the biopsy core/s comprise a small fraction of the renal parenchyma, and highly fibrotic kidneys often have insufficient glomerular tissue on biopsy samples to permit accurate histopathologic diagnosis [10–12].
Shear wave elastography (SWE) is an emerging ultrasound technique that permits the non-invasive measurement of tissue stiffness. SWE uses focused acoustic energy pulses to produce microscopic tissue displacement, which induces perpendicular shear waves that are sonographically tracked as they progress through tissue. Stiffer tissues have been shown to have increased shear wave velocities. Estimates of tissue Young’s modulus (YM), measured in kilopascals [kPa] can be derived from shear wave velocity, where higher values correlate with a higher degree of fibrosis [13, 14]. This technique has been FDA approved for use in liver disease and has high sensitivity and specificity to discriminate between normal and cirrhotic liver [15]. Variations of SWE have been used to study other organs including breast, thyroid, prostate, and renal allografts [16–21]. Prior human and animal studies have shown a correlation between SWE estimates of renal YM and presence of CKD or fibrosis [22, 23].
Shear wave elastography has only been used in two prior studies in native kidneys and has not yet been used to examine a heterogeneous population of CKD in the United States [22, 24]. There are limitations to these prior studies, including lack of non-diseased comparison group [22]. In this pilot study, we aim to explore whether SWE-derived estimates of tissue YM may serve as a non-invasive biomarker that can distinguish normal and abnormal renal parenchymal tissue.
Methods
Patient population
For this cross sectional pilot study, subjects were recruited from the outpatient renal clinic panels at an academic tertiary care center from March 2014 to September 2014. Inclusion criteria for subjects with CKD included: age greater than 18 years, eGFR less than 60 mL/min by the IDMS-traceable, 4-variable MDRD equation [25] or known diagnosis of CKD, and consent to undergo renal ultrasound. Exclusion criteria included body mass index (BMI) greater than 35 kg/m2, pregnancy or nursing status, or any condition that impeded visualization of the kidney by ultrasound. Healthy control subjects were screened for the absence of common medical conditions including CKD (and/or eGFR < 60 mL/min), hypertension, diabetes, and cardiovascular disease. Control subjects were recruited at the study site. Inclusion criteria for healthy subjects included: age greater than 18, BMI less than 35 kg/m2, not pregnant or nursing, and structurally normal kidneys on traditional renal ultrasound. Participants were not included or excluded on the basis of race, gender, or ethnicity. Demographic and medical information was taken from electronic medical record or by interview. Past medical history and etiology of CKD were determined by the participants’ treating providers and were extracted from medical documentation. Lab values were taken from the electronic medical record within one month of undergoing SWE, or if values were unobtainable, a study nurse performed a separate blood draw at the time of SWE. Study data were collected and managed using REDCap electronic data capture tools hosted at the Harvard Clinical and Translational Science Center [26].
Shear wave elastography
Shear wave elastography was performed with a curved 2–5 MHz broadband transducer on a two-port Aixplorer ultrasound system (Supersonic Imagine, Paris, France). A single board-certified radiologist (AES) with 13 years of sonography experience performed all SWE scans for this study. Participants were scanned in the typical manner renal sonographic images are obtained clinically, in the position offering the shortest distance to either kidney, typically the left decubitus or supine positions. Body position was not recorded. SWE measurements were obtained in a single region of interest (minimum diameter 6 mm) an area of renal parenchyma at least 1 cm deep of the capsule in the renal cortex, with specific avoidance of renal pyramids as the operator was able. Measurements where obtained where the acoustic window was optimal, typically in the lower renal pole. Distance from the skin to the region of interest was recorded as kidney depth and listed in Table 1 for cases and controls. Eight to twelve readings were taken per subject and a median SWE value was recorded as YM in kPa (Fig. 1). YM was calculated by Aixplorer software under the assumption of target tissue at body temperature using the formula E = ρ x c2, where E is tissue elasticity in kPa, ρ is tissue density in kg/m3 and c is shear wave velocity in m/s [27]. SWE measurements were obtained at end-expiration. All patients had confirmation of absence of hydronephrosis by traditional ultrasound prior to undergoing SWE. In all cases, imaging began with the right kidney. If the kidney was readily accessible SWE measurements were obtained. If the right kidney was deep or the acoustic window was considered suboptimal by the radiologist, SWE measurements were obtained from the left kidney. Eighty eight percent of participants underwent SWE on the right kidney.
Table 1.
Demographic information
| CKD (n = 25) | Control (n = 20) | |
|---|---|---|
| Age (years) | 61 (56, 70) | 34 (29, 49) |
| Male Gender | 16 (64 %) | 5 (25 %) |
| Ethnicitya | ||
| Non-Hispanic | 20 (83 %) | 18 (90 %) |
| Hispanic | 4 (17 %) | 2 (10 %) |
| Race | ||
| White | 20 (80 %) | 15 (75 %) |
| Other | 5 (20 %) | 5 (25 %) |
| Height (cm) | 170.2 (163.0, 177.8) | 165.0 (162.8, 169.0) |
| Weight (kg) | 76.0 (71.0, 88.0) | 65.8 (61.1, 69.0) |
| BMI (kg/m2) | 26.1 (24.8, 28.4) | 23.4 (22.1, 24.0) |
| Kidney Length (cm) b | 10.35 (9.16, 10.95) | 10.47 (10.10, 11.07) |
| Kidney Depth to Region of Interest (cm) | 3.60 (1.64, 5.56) | 3.15 (2.45, 3.85) |
| Hematocritc | 38.2 (33.6, 40.2) | 40.8 (39.6, 41.1) |
| BUN (mg/dL) d | 30 (18, 38) | 13 (11, 15) |
| Creatinine (mg/dL) d | 1.74 (1.42, 2.38) | 0.90 (0.79, 0.96) |
| GFR (mL/min) | 38 (28, 42) | >60 |
| CKD Stage | ||
| CKD Stage 1-2 | 1 (4 %) | |
| CKD Stage 3 | 17 (68 %) | |
| CKD Stage 4 | 5 (20 %) | |
| CKD Stage 5 | 2 (8 %) | |
| Cause of CKD | ||
| Diabetes/Hypertension | 13 (52 %) | |
| IgA Nephropathy | 3 (12 %) | |
| Renovascular Disease | 1 (4 %) | |
| Other Known Diagnosis | 6 (24 %) | |
| Unknown Diagnosis | 2 (8 %) | |
| Other Medical History | ||
| Hypertension | 24 (96 %) | |
| Hyperlipidemia | 18 (72 %) | |
| Diabetes | 7 (28 %) | |
| Gout | 5 (20 %) | |
| Coronary Artery Disease | 5 (20 %) | |
| Congestive Heart Failure | 5 (20 %) | |
| Vascular Disease | 4 (16 %) | |
| Hypothyroidism | 4 (16 %) | |
| Prostatic Hypertrophy | 3 (12 %) |
All continuous variables are given as medians (quartile 1, quartile 3). CKD stage calculated by MDRD equation. a N = 24 for CKD. b N = 23 for CKD and N = 18 for controls. c N = 20 for CKD and N = 9 for controls. d N = 9 for controls
Fig. 1.
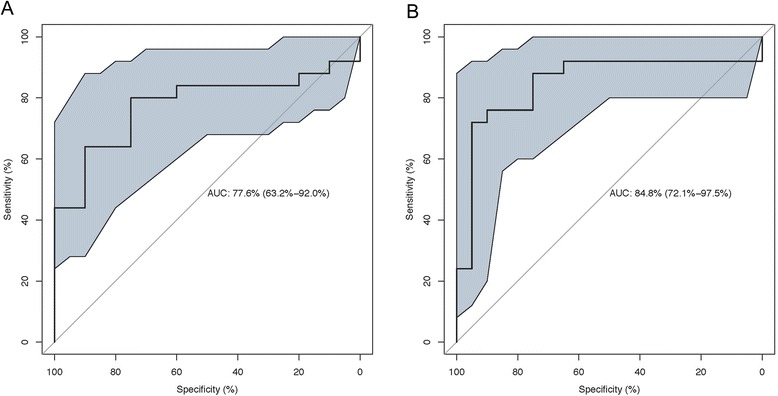
ROC Curves for Detecting Presence of CKD. Panel (a): Median Young’s Modulus (p = 0.018). Panel (b): Intra-subject Variability of Young’s Modulus (p = 0.002). P values were derived from logistic regression
Statistical analysis
The characteristics of the study participants by CKD and control group status were presented using median (quartile 1, quartile 3) or numbers (percentages). The median value for estimated tissue YM was selected due to the non-normality of individual measurements. The main outcome (median estimated tissue YM in kPa) was reported as a continuous variable and was compared between exposure variables using Wilcoxon Rank-Sum tests. Intra-subject variability was examined by comparing difference of individual readings from the median YM for each subject.
The diagnostic performance of SWE for distinguishing normal renal parenchyma from renal parenchyma affected by CKD was assessed using a univariate logistic regression model to construct receiver operating characteristic (ROC) curves. ROC analyses were performed to determine a cut point of SWE that would correctly classify the maximum number of participants based on sensitivity and specificity values. Wald asymptotic 95 % confidence limits are presented for sensitivity and specificity values. Percentile method 95 % confidence intervals for ROC curves were generated with 2000 replicate samples using the pROC package in R version 3.0.2 (Vienna, Austria) [28, 29]. Comparisons of area under the curves were performed by use of a contrast matrix to take differences of the area under the empirical ROC curves. Pearson correlation coefficients were used to assess the association between continuous exposure variables. Stratified analysis of the control and CKD groups were performed to evaluate for potential significant confounders of SWE values. SAS version 9.4 (Cary, NC) was used for all other non-ROC-related statistical analysis. Two-tailed p values of less than 0.05 were deemed statistically significant.
Ethics statement
Written informed consent was obtained from all study participants. All responses and patient/provider information were de-identified except to members of the research team. The Partners Human Research Committee for human subjects approved the study. All clinical investigation was conducted according to the principles expressed in the Declaration of Helsinki.
Results
Twenty-five subjects with CKD (“cases”) and 20 healthy subjects (“controls”) were enrolled. Cases were mostly male (64 %), white race (80 %), and of non-Hispanic origin (83 %). For cases, median GFR was 38 (quartile 1, quartiles 3: 28, 42) mL/min; median Cr was 1.74 (1.42, 2.38) mg/dL (normal range: 0.6-1.50 mg/dL). The majority of cases had CKD stage III or IV (88 %). A sensitivity analysis excluding the single patient with stage I/II CKD did not affect primary outcomes. The most common cause of CKD was diabetes or hypertension (52 %). Controls were mostly female (75 %), white race (75 %), and of non-Hispanic origin (90 %). Median BMI was 26.1 (24.8, 28.4) kg/m2 in cases and 23.4 (22.1, 24.0) kg/m2 in controls. Median age was 61 (56, 70) years for cases and 34 (29, 49) years for controls. Median kidney length was 10.35 (9.16, 10.95) cm in cases and 10.47 (10.10, 11.07) cm in controls (Table 1).
There was a significantly higher median estimated tissue YM for cases compared to controls (p = 0.002): median values were 9.40 (5.55, 22.35) kPa and 4.40 (3.68, 5.70) kPa, respectively (Fig. 2). Using a cutoff of 5.3 kPa for median estimated tissue YM, the area under the ROC curve to distinguish CKD from non-CKD state was 0.78 (95 % CI 0.63-0.92; p = 0.02) with a sensitivity and specificity of 80 % (95 % CI 64 %-96 %) and 75 % (95 % CI 56 %-94 %), respectively (Fig. 3a). Median intra-subject variability of individual estimated YM (distance from the median YM for each subject) was larger in cases compared to controls (3.88 [2.88, 5.13] vs. 1.41 [1.14, 2.13] kPa; p < 0.001). Using a cutoff of 2.8 kPa for intra-subject variability, the area under the ROC curve to distinguish diseased from healthy renal parenchyma was 0.85 (95 % CI 0.72-0.98; p = 0.002) with a sensitivity and specificity of 76 % (95 % CI 55 %-91 %) and 90 % (95 % CI 68 %-99 %), respectively (Fig. 3b). The estimated areas under the ROC curve for distinguishing healthy and diseased renal cortex using median estimated tissue YM or intra-subject variability were not significantly different (p = 0.15).
Fig. 2.
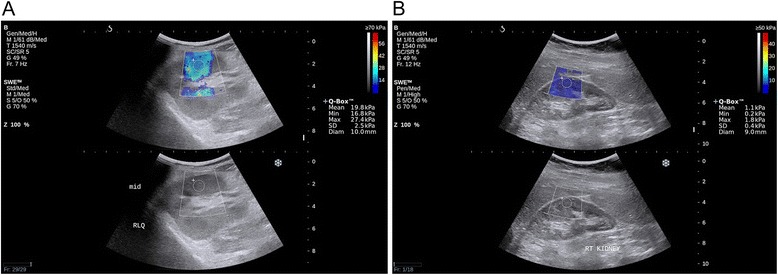
Representative Images of Shear Wave Elastography. Panel (a): right kidney of a subject with CKD. Panel (b): right kidney of a control subject
Fig. 3.
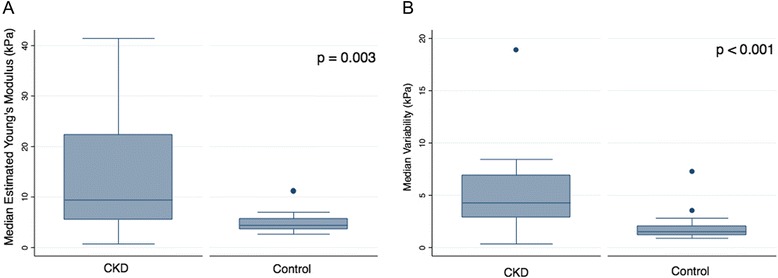
Median Estimated Young’s Modulus in CKD versus Controls (Panel a). Median Variability in Intra-subject SWE Readings in CKD and Controls (Panel b)
Among controls, only race was significantly associated with estimated tissue YM (p = 0.01). Among cases, estimated tissue YM was associated with female gender (p = 0.03), kidney depth (p = 0.02), height (p = 0.04), weight (p = 0.001), and BMI (p = 0.045). There was no correlation between estimated tissue YM and age or kidney length in either group (Table 2). For stratified analysis, potential confounders were dichotomized into high versus low values at their respective medians. Among cases, kidney depth was the only potential confounder that had significantly different values: 5.5 kPa [IQR 12.1] with kidney depth greater than or equal to 3.6 cm versus 12.3 kPa [IQR 18.0] with kidney depth less than 3.6 cm; p = 0.02. In the control group, BMI was the only potential confounder that had significantly different values: 5.1 kPa [IQR 2.5] with BMI greater than or equal to 23 kg/m2 versus 3.9 kPa [IQR 1.1] with BMI less than 23 kg/m2; p = 0.01 (Additional fie 1: Table S1).
Table 2.
Evaluation of Potential Influences on SWE in CKD and Control Groups
| Factors | CKD | Control | ||
|---|---|---|---|---|
| r | P value | r | P value | |
| Age | 0.370 | 0.07 | 0.325 | 0.16 |
| Height | −0.423 | 0.04 | −0.235 | 0.31 |
| Weight | −0.556 | 0.004 | 0.033 | 0.90 |
| BMI | −0.404 | 0.045 | 0.251 | 0.29 |
| Kidney Length | −0.257 | 0.24 | −0.238 | 0.34 |
| Kidney Depth | −0.525 | 0.007 | −0.336 | 0.15 |
| Hematocrita | −0.014 | 0.95 | −0.447 | 0.23 |
| Creatinine | −0.123 | 0.56 | ||
| eGFR | −0.018 | 0.93 | ||
| BUN | −0.084 | 0.69 | ||
| Young’s modulus | Young’s modulus | |||
| Race | 0.58 | 0.01 | ||
| White | 10.70 (5.08, 24.85) | 4.85 (4.30, 6,85) | ||
| Other | 7.60 (7.50, 10.50) | 3.10 (2.70, 3.90) | ||
| Gender | 0.04 | 0.15 | ||
| Male | 6.60 (4.10, 12.33) | 3.55 (3.10, 4.20) | ||
| Female | 22.35 (9.40, 25.80) | 4.50 (3.90, 6.20) | ||
| Ethnicity | 0.87 | 0.20 | ||
| Non-Hispanic | 10.70 (5.78, 23.13) | 4.35 (3.55, 4.90) | ||
| Hispanic | 5.58 (4.50, 8.05) | 6.03 (5.20, 6.85) | ||
Correlation coefficient (r) given for continuous variables. Median Young’s modulus (quartile 1, quartile 3) in kPa given for categorical variables. Abbreviations: BMI (body mass index), eGFR (estimated glomerular filtration rate), BUN (blood urea nitrogen). a N = 9 for controls
Discussion
Our results suggest estimated tissue YM can be used to non-invasively distinguish renal tissue affected by CKD from normal renal tissue, even when kidney size does not differentiate the two conditions. Of the two prior human studies examining SWE in native kidneys, one also reported a correlation between estimated tissue YM and presence of CKD [24]. The second study, of Chinese subjects primarily with early stage CKD, was designed to look for differences between CKD subgroups and did not include healthy patients as a comparator [22]. Except for stage V, neither of these studies detected a correlation between estimated tissue YM and CKD stage. This is unsurprising; the relatively small number of subjects in these studies suggests they were insufficiently powered to do so. The potential of SWE to detect diffuse renal disease is clinically relevant, as conventional B mode sonography is well known to be insensitive for the detection of diffuse renal disease, and is presently used primarily for the exclusion of hydronephrosis [30].
In our study, we make two important assumptions: (1) we assumed CKD would alter tissue stiffness in a way that could be detected by SWE. We considered this biologically plausible, as renal parenchymal fibrosis and inflammation are known to occur in CKD, and fibrosis is known to alter tissue SWE estimates of tissue stiffness in other organs [16–19]. Our study did not include patients who underwent contemporaneous kidney biopsy, so we did not directly measure the relationship between histologic measures of fibrosis and renal stiffness. Since inflammation, fibrosis, and renal perfusion abnormalities all contribute to the clinical CKD syndrome, it is unlikely that histologic measures of renal fibrosis alone would have been an appropriate reference standard.
The majority of prior studies examining variations of SWE technology and renal fibrosis are in renal transplants, and support a positive correlation between SWE estimates of renal stiffness and pathologic fibrosis or eGFR, [19–21, 24, 31, 32] though at least two studies (including one examining native kidneys) did not find a significant correlation [22, 33]. Potential explanations for this include SWE technology variation, type II error owing to small sample sizes, incorrect estimation of fibrosis by biopsy, which is known to be an imperfect reference standard, [34] operator variability, or a true lack of correlation.
A second assumption is that CKD is the cause of tissue stiffness, rather than other potential confounders. Our study identified associations between estimated renal tissue YM and race, gender, kidney depth height, weight, and BMI, albeit not in both case and control groups. Prior studies of renal SWE have identified several potential confounders, including bladder pressure, [23] renal blood flow, [23] BMI, [21] kidney depth, [21] surrounding fluid accumulation, [21] and age [24]. With the exception of BMI and kidney depth, none of these factors appear across multiple studies, suggesting these potential confounding effects may be small or inconsistent. In a large study of healthy subjects undergoing SWE, there was no difference in renal cortex readings between men and women [35]. The effect of potential confounders, such as gender and renal blood flow, remains a potential area of future study for SWE.
When considering these assumptions, it is relevant to note that tissue YM, similar to other physical properties of tissue, such as weight, viscosity, radiodensity, and acoustic impedance, represents bulk tissue properties, and is therefore representative of composite endpoints produced by tissue content, structure, and microenvironment. It is probable that additional situation-specific tissue microenvironment factors, such as inflammation, may confound SWE estimates of tissue YM. This is known to be the case in liver disease, where hepatic inflammation has been shown to increase tissue stiffness estimates [36]. Despite this, the clinical utility of elastography for liver fibrosis staging is now well established, and SWE is used clinically to differentiate early and advanced liver fibrosis without biopsy [15]. We anticipate SWE may similarly have great utility in diffuse renal disease as it has the potential both to reduce biopsy use, and to permit repeated non-invasive direct estimates of renal parenchymal disease severity. Ultimately, such a tool could potentially be used to track renal fibrosis progression and permit therapy individualization in a manner that is presently not possible.
Our study supports prior evidence that the relationship between SWE estimates of tissue YM and renal fibrosis severity may not be as robust as that seen in liver disease. For example, the area under ROC curve for estimates of YM has been reported to be as high as 0.98 in liver disease [15] versus 0.78 in our study and 0.75 in Guo et al. [24]. There are several potential reasons for this, including: (1) greater kidney depth from the skin surface compared with the liver; (2) the more rounded renal shape, which may cause refraction of acoustic displacement pulses with greater variation in renal parenchymal shear wave generation; and (3) larger variability in the reference standards used for the quantitation of renal fibrosis than in the relatively simpler liver fibrosis staging METAVIR classification.
We showed increased variability in individual SWE readings in the CKD group. There are two potential reasons for this: (1) SWE may be less precise in stiffer tissue. A larger standard deviation and range of readings in subgroups with advanced fibrosis were observed in prior liver and kidney studies supporting this notion [15, 19]. (2) Alternatively, there is an intriguing possibility that renal parenchymal fibrosis results in true increased heterogeneity of the tissue YM. If validated, tissue stiffness heterogeneity could prove a valuable biomarker of fibrosis severity, and add additional explanatory power to this new technology. Interestingly, the area under the ROC curve for variability of measurement was better compared to the estimation of YM itself, though this was not statistically significant, and the two predictors together did not create a statistically significant combined model. Other factors, such as probe type, tissue depth, and operator technique are still being explored as explanations of variability in measurements for this new technology [37–39]. Regardless of the reason for measurement variation, it is clear that judicious selection of clinical outcomes and sample size will be necessary in future studies to supply sufficient power. Studies targeted at fibrosis staging dichotomized at clinically relevant cut-offs may be more likely to be productive than attempts to establish a linear relationship between fibrosis stage and tissue stiffness.
One should interpret these results within the context of the limitations of our study: (1) as expected for a pilot study, we were only able to capture a small cross section of the large and heterogeneous CKD population. Half of CKD subjects had diabetic or hypertensive kidney disease, though it is not known if the disease process driving CKD has an independent effect on YM. (2) We were not able to control for all factors described as potential confounders in prior studies. Most notably, we had no measure of renal blood flow, which was out of the scope of this study. Only one subject had known renal vascular disease, and excluding this subject did not affect our conclusions. Kidney depth may have also influenced shear wave readings, which could not be controlled for in this pilot study. (3) Age has been identified as a confounder of YM in prior studies. The median age of the cases was greater than that of the controls in our study, which may have biased the stiffness estimates upward in our case cohort. However, one prior study, [24] advancing age was moderately inversely correlated with renal stiffness. This suggests that the observed higher renal stiffness in the cases was not due to relatively higher age in this group. (4) We also used the known imperfect reference standard of eGFR to estimate CKD severity, and did not have renal biopsy data available to quantify fibrosis histologically. (5) We did not measure inter-observation variance given all SWE studies were performed by a single radiologist. Despite these limitations, we believe our pilot study shows the potential of SWE to expand the role of ultrasound in CKD beyond the exclusion of hydronephrosis to the non-invasive and cost-effective staging of diffuse renal disease.
Conclusions
SWE-derived estimates of renal stiffness and intra-subject estimated stiffness variability are higher in patients with CKD than in healthy controls. Renal fibrosis is a plausible explanation for the observed difference in YM. Shear wave elastography may be a low-cost way to provide additional diagnostic information in CKD. Further studies are required to determine the relationship between YM, estimated renal stiffness, and renal fibrosis severity.
Acknowledgements
The authors would like to thank the Thadhani Lab for their feedback on the study design and data analysis. ASA is supported by NIH grant 5T32DK007540-29. HYL is supported in part by NIH grant RO1 DK 069533 and RO1 071837.
Abbreviations
- CKD
Chronic kidney disease
- ESRD
End stage renal disease
- eGFR
Estimated glomerular filtration rate
- SWE
Shear wave elastography
- YM
Young’s modulus
- kPa
Kilopascals
- BMI
Body mass index
- ROC
Receiver operating curves
Additional file
Table S1. Stratified analysis of potential confounders in CKD and Control Groups. (DOC 54 kb)
Footnotes
Competing interests
AES has received research equipment support from Supersonic Imagine, maker of the Aixplorer ultrasound machine. RIT is a consultant to Fresenius Medical Care North America, a dialysis provider.
Authors’ contributions
AES, WWW, JLB, RIT, HYL contributed to study design. AES, QZ, MD, AA contributed to ultrasonography and interpretation of imaging. DAS, CAT, SD contributed to subject recruitment and database management. ASA and AES were the primary writers of the manuscript. ASA and JW contributed to analysis and statistics. All authors read and approved the final version of this manuscript.
Contributor Information
Anthony E. Samir, Email: ASAMIR@mgh.harvard.edu
Andrew S. Allegretti, Phone: 617-724-8018, Email: AALLEGRETTI@partners.org
Qingli Zhu, Email: QZHU@mgh.harvard.edu.
Manish Dhyani, Email: Dhyani.Manish@mgh.harvard.edu.
Arash Anvari, Email: AANVARI@PARTNERS.ORG.
Dorothy A. Sullivan, Email: DSULLIVAN18@mgh.harvard.edu
Caitlin A. Trottier, Email: caittrot@bu.edu
Sarah Dougherty, Email: SDOUGHERTY@MGH.HARVARD.EDU.
Winfred W. Williams, Email: WWWILLIAMS@mgh.harvard.edu
Jodie L. Babitt, Email: Babitt.Jodie@mgh.harvard.edu
Julia Wenger, Email: JWENGER1@partners.org.
Ravi I. Thadhani, Email: RTHADHANI@mgh.harvard.edu
Herbert Y. Lin, Phone: 617-726-5661, Email: Lin.Herbert@mgh.harvard.edu
References
- 1.Anonymous Kidney Disease Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:1–150. doi: 10.1038/kisup.2012.73. [DOI] [Google Scholar]
- 2.Stevens PE, Levin A, Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013;158(11):825–30. doi: 10.7326/0003-4819-158-11-201306040-00007. [DOI] [PubMed] [Google Scholar]
- 3.Collins AJ, Foley RN, Herzog C, Chavers BM, Gilbertson D, Ishani A, et al. Excerpts from the US Renal Data System 2009 Annual Data Report. Am J Kidney Dis. 2010;55(1 Suppl 1):S1–420. doi: 10.1053/j.ajkd.2009.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Coresh J, Byrd-Holt D, Astor BC, Briggs JP, Eggers PW, Lacher DA, et al. Chronic kidney disease awareness, prevalence, and trends among U.S. adults, 1999 to 2000. J Am Soc Nephrol. 2005;16(1):180–188. doi: 10.1681/ASN.2004070539. [DOI] [PubMed] [Google Scholar]
- 5.Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–305. doi: 10.1056/NEJMoa041031. [DOI] [PubMed] [Google Scholar]
- 6.Rule AD, Rodeheffer RJ, Larson TS, Burnett JC, Jr, Cosio FG, Turner ST, et al. Limitations of estimating glomerular filtration rate from serum creatinine in the general population. Mayo Clin Proc. 2006;81(11):1427–34. doi: 10.4065/81.11.1427. [DOI] [PubMed] [Google Scholar]
- 7.Bohle A, Mackensen-Haen S, von Gise H. Significance of tubulointerstitial changes in the renal cortex for the excretory function and concentration ability of the kidney: a morphometric contribution. Am J Nephrol. 1987;7(6):421–33. doi: 10.1159/000167514. [DOI] [PubMed] [Google Scholar]
- 8.Eddy AA. Experimental insights into the tubulointerstitial disease accompanying primary glomerular lesions. J Am Soc Nephrol. 1994;5(6):1273–87. doi: 10.1681/ASN.V561273. [DOI] [PubMed] [Google Scholar]
- 9.Hewitson TD. Fibrosis in the kidney: is a problem shared a problem halved? Fibrogenesis Tissue Repair. 2012;5(Suppl 1 Proceedings of Fibroproliferative disorders: from biochemical analysis to targeted therapiesPetro E Petrides and David Brenner):S14. doi: 10.1186/1755-1536-5-S1-S14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Farris AB, Colvin RB. Renal interstitial fibrosis: mechanisms and evaluation. Curr Opin Nephrol Hypertens. 2012;21(3):289–300. doi: 10.1097/MNH.0b013e3283521cfa. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Whittier WL, Korbet SM. Timing of complications in percutaneous renal biopsy. J Am Soc Nephrol. 2004;15(1):142–7. doi: 10.1097/01.ASN.0000102472.37947.14. [DOI] [PubMed] [Google Scholar]
- 12.Maripuri S, Penson DF, Ikizler TA, Cavanaugh KL. Outpatient versus inpatient observation after percutaneous native kidney biopsy: a cost minimization study. Am J Nephrol. 2011;34(1):64–70. doi: 10.1159/000328901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Urban MW, Chen S, Fatemi M. A review of Shearwave Dispersion Ultrasound Vibrometry (SDUV) and its Applications. Curr Med Imaging Rev. 2012;8(1):27–36. doi: 10.2174/157340512799220625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kotlyar DS, Blonski W, Rustgi VK. Noninvasive monitoring of hepatitis C fibrosis progression. Clin Liver Dis. 2008;12(3):557–71. doi: 10.1016/j.cld.2008.03.006. [DOI] [PubMed] [Google Scholar]
- 15.Chen S, Sanchez W, Callstrom MR, Gorman B, Lewis JT, Sanderson SO, et al. Assessment of liver viscoelasticity by using shear waves induced by ultrasound radiation force. Radiology. 2013;266(3):964–70. doi: 10.1148/radiol.12120837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zheng XZ, Ji P, Mao HW, Zhang XY, Xia EH, Xing-Gu, et al. A novel approach to assessing changes in prostate stiffness with age using virtual touch tissue quantification. J Ultrasound Med. 2011;30(3):387–90. doi: 10.7863/jum.2011.30.3.387. [DOI] [PubMed] [Google Scholar]
- 17.Bai M, Du L, Gu J, Li F, Jia X. Virtual touch tissue quantification using acoustic radiation force impulse technology: initial clinical experience with solid breast masses. J Ultrasound Med. 2012;31(2):289–94. doi: 10.7863/jum.2012.31.2.289. [DOI] [PubMed] [Google Scholar]
- 18.Zhang YF, Xu HX, He Y, Liu C, Guo LH, Liu LN, et al. Virtual touch tissue quantification of acoustic radiation force impulse: a new ultrasound elastic imaging in the diagnosis of thyroid nodules. PLoS One. 2012;7(11) doi: 10.1371/journal.pone.0049094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Arndt R, Schmidt S, Loddenkemper C, Grunbaum M, Zidek W, van der Giet M, et al. Noninvasive evaluation of renal allograft fibrosis by transient elastography--a pilot study. Transpl Int. 2010;23(9):871–7. doi: 10.1111/j.1432-2277.2010.01057.x. [DOI] [PubMed] [Google Scholar]
- 20.Grenier N, Poulain S, Lepreux S, Gennisson JL, Dallaudiere B, Lebras Y, et al. Quantitative elastography of renal transplants using supersonic shear imaging: a pilot study. Eur Radiol. 2012;22(10):2138–46. doi: 10.1007/s00330-012-2471-9. [DOI] [PubMed] [Google Scholar]
- 21.Sommerer C, Scharf M, Seitz C, Millonig G, Seitz HK, Zeier M, et al. Assessment of renal allograft fibrosis by transient elastography. Transpl Int. 2013;26(5):545–51. doi: 10.1111/tri.12073. [DOI] [PubMed] [Google Scholar]
- 22.Wang L, Xia P, Lv K, Han J, Dai Q, Li XM, et al. Assessment of renal tissue elasticity by acoustic radiation force impulse quantification with histopathological correlation: preliminary experience in chronic kidney disease. Eur Radiol. 2014;24(7):1694–9. doi: 10.1007/s00330-014-3162-5. [DOI] [PubMed] [Google Scholar]
- 23.Gennisson JL, Grenier N, Combe C, Tanter M. Supersonic shear wave elastography of in vivo pig kidney: influence of blood pressure, urinary pressure and tissue anisotropy. Ultrasound Med Biol. 2012;38(9):1559–67. doi: 10.1016/j.ultrasmedbio.2012.04.013. [DOI] [PubMed] [Google Scholar]
- 24.Guo LH, Xu HX, Fu HJ, Peng A, Zhang YF, Liu LN. Acoustic radiation force impulse imaging for noninvasive evaluation of renal parenchyma elasticity: preliminary findings. PLoS One. 2013;8(7) doi: 10.1371/journal.pone.0068925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145(4):247–54. doi: 10.7326/0003-4819-145-4-200608150-00004. [DOI] [PubMed] [Google Scholar]
- 26.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ferraioli G, Tinelli C, Dal Bello B, Zicchetti M, Filice G, Filice C, et al. Accuracy of real-time shear wave elastography for assessing liver fibrosis in chronic hepatitis C: a pilot study. Hepatology. 2012;56(6):2125–33. doi: 10.1002/hep.25936. [DOI] [PubMed] [Google Scholar]
- 28.Robin X, Turck N, Hainard A, Tiberti N, Lisacek F, Sanchez JC, et al. pROC: an open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinformatics. 2011;12:77. doi: 10.1186/1471-2105-12-77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Carpenter J, Bithell J. Bootstrap confidence intervals: when, which, what? A practical guide for medical statisticians. Stat Med. 2000;19(9):1141–64. doi: 10.1002/(SICI)1097-0258(20000515)19:9<1141::AID-SIM479>3.0.CO;2-F. [DOI] [PubMed] [Google Scholar]
- 30.O'Neill WC. B-mode sonography in acute renal failure. Nephron Clin Pract. 2006;103(2):c19–23. doi: 10.1159/000090604. [DOI] [PubMed] [Google Scholar]
- 31.Stock KF, Klein BS, Vo Cong MT, Sarkar O, Romisch M, Regenbogen C, et al. ARFI-based tissue elasticity quantification in comparison to histology for the diagnosis of renal transplant fibrosis. Clin Hemorheol Microcirc. 2010;46(2–3):139–48. doi: 10.3233/CH-2010-1340. [DOI] [PubMed] [Google Scholar]
- 32.He WY, Jin YJ, Wang WP, Li CL, Ji ZB, Yang C. Tissue elasticity quantification by acoustic radiation force impulse for the assessment of renal allograft function. Ultrasound Med Biol. 2014;40(2):322–9. doi: 10.1016/j.ultrasmedbio.2013.10.003. [DOI] [PubMed] [Google Scholar]
- 33.Syversveen T, Brabrand K, Midtvedt K, Strom EH, Hartmann A, Jakobsen JA, et al. Assessment of renal allograft fibrosis by acoustic radiation force impulse quantification—a pilot study. Transpl Int. 2011;24(1):100–5. doi: 10.1111/j.1432-2277.2010.01165.x. [DOI] [PubMed] [Google Scholar]
- 34.Farris AB, Adams CD, Brousaides N, Della Pelle PA, Collins AB, Moradi E, et al. Morphometric and visual evaluation of fibrosis in renal biopsies. J Am Soc Nephrol. 2011;22(1):176–86. doi: 10.1681/ASN.2009091005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Arda K, Ciledag N, Aktas E, Aribas BK, Kose K. Quantitative assessment of normal soft-tissue elasticity using shear-wave ultrasound elastography. AJR Am J Roentgenol. 2011;197(3):532–6. doi: 10.2214/AJR.10.5449. [DOI] [PubMed] [Google Scholar]
- 36.Sagir A, Erhardt A, Schmitt M, Haussinger D. Transient elastography is unreliable for detection of cirrhosis in patients with acute liver damage. Hepatology. 2008;47(2):592–5. doi: 10.1002/hep.22056. [DOI] [PubMed] [Google Scholar]
- 37.Chang S, Kim MJ, Kim J, Lee MJ. Variability of shear wave velocity using different frequencies in acoustic radiation force impulse (ARFI) elastography: a phantom and normal liver study. Ultraschall Med. 2013;34(3):260–5. doi: 10.1055/s-0032-1313008. [DOI] [PubMed] [Google Scholar]
- 38.Potthoff A, Attia D, Pischke S, Kirschner J, Mederacke I, Wedemeyer H, et al. Influence of different frequencies and insertion depths on the diagnostic accuracy of liver elastography by acoustic radiation force impulse imaging (ARFI) Eur J Radiol. 2013;82(8):1207–12. doi: 10.1016/j.ejrad.2013.02.011. [DOI] [PubMed] [Google Scholar]
- 39.Ozkan F, Yavuz YC, Inci MF, Altunoluk B, Ozcan N, Yuksel M, et al. Interobserver variability of ultrasound elastography in transplant kidneys: correlations with clinical-Doppler parameters. Ultrasound Med Biol. 2013;39(1):4–9. doi: 10.1016/j.ultrasmedbio.2012.09.013. [DOI] [PubMed] [Google Scholar]