

Abstract
Introduction
Maintaining adequate nutrition for Head and Neck Cancer (HNC) patients is challenging due to both the malignancy and the rigours of radiation treatment. As yet, health behaviour interventions designed to maintain or improve nutrition in patients with HNC have not been evaluated. The proposed trial builds on promising pilot data, and evaluates the effectiveness of a dietitian-delivered health behaviour intervention to reduce malnutrition in patients with HNC undergoing radiotherapy: Eating As Treatment (EAT).
Methods and analysis
A stepped-wedge cluster randomised design will be used. All recruitment hospitals begin in the control condition providing treatment as usual. In a randomly generated order, oncology staff at each hospital will receive 2 days of training in EAT before switching to the intervention condition. Training will be supplemented by ongoing supervision, coaching and a 2-month booster training provided by the research team. EAT is based on established behaviour change counselling methods, including motivational interviewing, cognitive–behavioural therapy, and incorporates clinical practice change theory. It is designed to improve motivation to eat despite a range of barriers (pain, mucositis, nausea, reduced or no saliva, taste changes and appetite loss), and to provide patients with practical behaviour change strategies. EAT will be delivered by dietitians during their usual consultations. 400 patients with HNC (nasopharynx, hypopharynx, oropharynx, oral cavity or larynx), aged 18+, undergoing radiotherapy (>60 Gy) with curative intent, will be recruited from radiotherapy departments at 5 Australian sites. Assessments will be conducted at 4 time points (first and final week of radiotherapy, 4 and 12 weeks postradiotherapy). The primary outcome will be a nutritional status assessment.
Ethics and dissemination
Ethics approval from all relevant bodies has been granted. Study findings will be disseminated widely through peer-reviewed publications and conference presentations.
Trial registration number
ACTRN12613000320752.
Introduction
Malignancies of the upper aerodigestive tract and its connected structures, known collectively as Head and Neck Cancers (HNC), are the fifth most commonly diagnosed cancers worldwide.1 HNC has a relatively high mortality rate, approaching 50%.2 Malnutrition is a major problem for people with HNC. The prevalence of malnutrition across all patients with cancer in Australia has been reported as between 40% and 80%, with patients with HNC over-represented in this figure.3 The malignancy itself can cause difficulty in eating, fatigue, loss of appetite and weight loss; and treatments for the cancer can compound these problems with mucositis, dry mouth and taste changes.4
Impact of malnutrition
The consequences of malnutrition in patients with cancer include impaired immune function, reduced vitality and reduced resistance to the disease, which lead to an increase in complications due to side effects of the treatment and increased morbidity.5 Further, the effectiveness of the radiotherapy itself is significantly reduced if the patient becomes so malnourished they require a break or early termination of treatment.6 Multiple laboratory and clinical trials have demonstrated that treatment interruption is the strongest predictor of poor radiotherapy outcome,7 and malnutrition is one of the most common reasons for treatment to be interrupted.8 Therefore, it is not surprising that poor nutritional status during treatment has been found to be a strong predictor of mortality in HNC.9 Further, a dose effect of malnutrition has been found, with a greater than 20% weight reduction over the course of treatment resulting in a significant increase in toxicity and mortality during radiation therapy.10 Given the impact of malnutrition on the health of people with HNC and their response to treatment, it is usual practice for patients to consult regularly with a dietitian throughout the course of their treatment.
Mental illness in head and neck cancer
In addition to nutritional difficulties, patients with HNC also exhibit relatively high rates of mental health problems, particularly depression.11 Our recent study found that baseline depression predicted those patients with HNC who were most likely to become malnourished by the end of their treatment.12 Depression was a better predictor than the commonly accepted risk factors for malnutrition: gender, age, presence of a live-in carer, tumour stage, dose of radiation, concurrent chemotherapy or surgery.12 It has also been suggested that the high levels of disfigurement and loss of functioning in HNC may lead to greater levels of anxiety than those found in other cancer populations.13 Furthermore, the risk factors for HNC (smoking and alcohol misuse)14 may be indicative of premorbid depression15 in these patients, and have been linked to worse treatment side effects16–19 and poorer outcomes of radiotherapy.20–23 Despite the high prevalence of mental illness among patients with HNC and the implications for treatment, a recent systematic review reported that no studies have evaluated psychological interventions targeting health behaviours among patients with HNC.24
Compliance problems in head and neck cancer
Patient compliance with dietary advice is essential to achieve positive treatment and health outcomes. A systematic review of nutrition advice in patients with HNC receiving radiotherapy found that dietetic intervention throughout treatment maintained or improved patients' nutritional status.25 Furthermore, nutritional advice has been found to improve a range of patient outcomes during26 and after treatment,27 including treatment completion rates, unplanned hospital visits, length of stay and weight loss.28 However, patients with HNC are often non-compliant with dietary advice. For some, having to return to the hospital for dietetic appointments in addition to their radiotherapy can be an impediment; particularly if the appointments are not viewed as a core component of their cancer treatment. In response, dietitians often lack the specific confidence, skills and time to change the dietary behaviours of patients with HNC, especially if those patients have mental health and/or substance use problems and may not see dietetic care as important.
Eating as treatment
This trial attempts to address the inherent difficulties in intervening with the HNC population including their premorbid mental health, non-engagement and non-compliance with dietary advice. It does this by providing dietitians with training, skills and knowledge to deal with this difficult and often overlooked group. The study builds on previous findings by employing motivational interviewing (MI29), a counselling style shown to be effective among other non-compliant patient groups30 and simple cognitive and behavioural strategies. Dietitians will be trained, supervised and coached in the provision of the intervention known as Eating As Treatment (EAT), guided by an intervention manual (available on request). Dietitians will also receive training in the administration of a brief screening tool for symptoms of depression. In accordance with best practice recommendations, dietitians will be supported to identify patients at risk of psychosocial distress and to work with the HNC team to mobilise appropriate support. A raft of evidence-based practice-change strategies will also be adopted to overcome systemic and other barriers to clinician compliance, thereby maximising the clinical implementation of EAT.
Aims and hypotheses
This trial aims to test the effectiveness of the EAT intervention. EAT is a dietitian-delivered intervention to prevent malnutrition in patients with HNC undergoing radiotherapy at five Australian hospital sites. The primary objective of the trial is to maintain nutrition in patients with HNC undergoing radiotherapy.
It is hypothesised that patients with HNC receiving the EAT intervention will have lower malnutrition scores, as measured by the Patient-Generated—Subjective Global Assessment (PG-SGA), at post-treatment and follow-up, compared with patients in the control condition (receiving usual care).
Secondary hypotheses are that, relative to control patients, intervention patients will have higher rates of treatment completion, fewer unplanned hospital visits, shorter lengths of stay, lower depression, higher quality of life and more quality adjusted life years.
Methods and analysis
Trial design
The present study utilises a stepped-wedge, cluster-randomised controlled design. In a stepped-wedge design, all recruitment sites (hospitals) begin in the control condition and then move to the intervention condition in a randomised order (figure 1). This design was chosen because the intervention involves training dietitians and changing their practice, a simple, randomised trial would require the dietitians to ignore the intervention principles and skills they have learned when treating control patients, making the likelihood for contamination very high. Therefore, a cluster-randomised design was necessary. A standard, parallel, cluster-randomised trial would require a large number of hospitals that treat high numbers of patients with HNC. The low number of radiotherapy departments in Australia treating high numbers of patients with HNC meant that this option was also not possible. A stepped-wedge, cluster-randomised, controlled trial provides the same level of evidence as a standard, parallel, cluster-randomised controlled trial31 using fewer sites, while reducing the potential for contamination.
Figure 1.
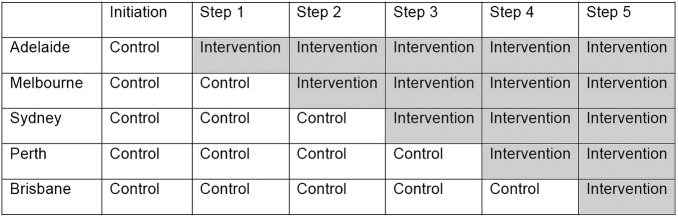
Progression of intervention roll-out in a stepped-wedge model.
Recruitment
Sites were recruited through the Trans-Tasman Radiation Oncology Group (TROG) who invited members from large radiotherapy departments within Australian hospitals to put their sites forward as potential clusters. Participants will be recruited from six of these large radiotherapy departments located in Adelaide, South Australia; Melbourne, Victoria; Sydney, New South Wales; Perth, Western Australia; and Brisbane, Queensland. There are two hospitals in Brisbane that share a dietetic department. So, although patients are recruited from two different hospitals, they will be treated as one progression step in the stepped wedge, and move to the intervention period at the same time. This equates to a total of five wedge steps.
Prior to study commencement, the order in which hospitals receive training (thereby the duration of control and intervention periods) was randomised by an independent statistician using a uniform random number generator in STATA. The randomised order was Adelaide, Melbourne, Sydney, Perth and Brisbane.
Participants
Inclusion criteria
Patients eligible for inclusion will meet the following criteria:
Aged 18 years or older.
Pathologically confirmed diagnosis of HNC, that is, cancer involving the nasopharynx, oropharynx, oral cavity, larynx, or hypopharynx, requiring definitive or postoperative radiotherapy with curative intent (chemoradiation (including neoadjuvant and adjuvant chemotherapy) permitted).
Regional nodal irradiation included in PTV1 (as a minimum ipsilateral levels II-III), and receiving a prescribed dose of at least 60 Gy.
Available for follow-up for at least 6 months poststudy initiation.
Capacity to provide written informed consent.
Exclusion criteria
Inability to communicate in English.
Presence of organic brain diseases (impairing ability to complete questionnaires satisfactorily).
Likely insignificant oral or pharyngeal mucositis as a complication of radiotherapy treatment (patients with T1/T2 glottic carcinoma undergoing small-field radiotherapy or T1/T2 tonsil cancer undergoing unilateral treatment).
Recruitment
Approximately one participant per week per hospital will be expected to be enrolled in the study. It is estimated that at this rate, recruitment will run for approximately 22 months.
Treatment
Control
During the control phase, each hospital will be instructed to deliver treatment as usual, making no changes to any part of their clinical care.
Intervention
Training
When a hospital moves from control to intervention, researchers will travel to the hospital to provide training. This will be delivered in a 2-day workshop followed by a day in which a booster training session is delivered, followed by the researchers accompanying dietitians during their usual consultations to help them integrate into their clinical practice what they have learned. The researchers will return 2 months later to refresh EAT intervention skills, problem-solve clinical concerns, and troubleshoot any practice change issues that may have arisen. During the intervention phase, dietitians will participate in regular supervision with one of the researchers (clinical psychologist, AKB). Where possible, individual supervision via telephone will occur fortnightly for the first 2 months post-training, and regular written feedback will be provided. Group supervision will be introduced during the 2-month ‘booster’ visit. Group supervision will then occur monthly, thereafter, via skype/teleconference/videoconference. Supervision will be used to discuss clinical issues, problem-solve, and provide skills-based feedback. Common themes, barriers and solutions discussed during supervision will be distributed (eg, email/discussion board) to participating dietitians across all hospitals.
Eating as treatment
The intervention is named EAT, to emphasise that maintaining adequate nutrition during radiotherapy is an integral part of cancer treatment and not merely an adjunct to survival. In order for patients with HNC to eat, they must overcome significant barriers of pain, oral disfigurement, mucositis, nausea, reduced or no saliva, taste changes and severe loss of appetite, in addition to the premorbid complications of high rates of smoking, alcohol misuse, mental health problems and poor levels of self-care.
The content of the intervention is a distillation of behaviour change strategies of MI and cognitive–behavioural therapy (CBT), developed specifically for patients with HNC undergoing radiotherapy, and targeting behaviours around nutrition. The intervention was successfully piloted by a clinical psychologist,12 and has been refined for delivery by dietitians in the clinical setting, alongside their standard dietetic consultations with patients with HNC. The refined training was piloted with dietitians at the Calvary Mater Newcastle, who found the training acceptable, feasible and useful.
Although the training is standardised, the intervention itself is not highly structured, as it has been demonstrated that MI studies that do not have a structured manual produce almost double the effect size of those that are highly manualised.32 Instead, training in EAT uses simply worded principles to guide the dietitian (figure 2), reminding them to integrate the skills they have learned in training into their normal clinical practice.
Figure 2.

Principles prompt and conversation guide for Eating as Treatment.
The first principle refers to the MI interactional style in which clinicians are empathic, collaborative and elicit motivation for change from the patients themselves.29 This principle refers both to the importance of allowing the patient reinforce their own reasons for change (change talk), as well as avoiding pushing the patient into creating arguments not to change (sustain talk). These skills will be used to elicit motivation to change eating behaviour and to help generate concrete behavioural goals.
There are no specific ‘scripts' in EAT. However, there is one specific conversation that dietitians will be trained to hold with patients, referred to as Eat To Live. Using MI skills, dietitians will elicit patients' reasons for having radiotherapy. Although patients’ reasons will be many and varied, ultimately, a core reason for undergoing the rigours of radiotherapy will have some element of wanting to live (palliative treatment is an exclusion criterion). We can be confident that this is the case, as they are attending radiotherapy every day for 5–7 weeks, despite sometimes quite severe side effects. Dietitians then offer an invitation to explain the correlation between malnutrition during radiotherapy and poorer outcomes. It is important that this information is delivered as a description of the HNC population rather than becoming accusatory of the patient's behaviour personally, thus keeping to the first principle. The dietitian then deploys variance by inviting the patient to reflect on their continued attendance at radiotherapy and their concurrent nutritional behaviours that may not be enhancing the likelihood of meeting the core goal of living. As always, deploying variance requires a good rapport and genuineness for it not to seem accusatory and confrontational. From this point, the dietitian attempts to convert the motivation elicited into concrete dietary behavioural changes by asking the patient what they feel are the next step.
The remaining three principles in EAT will be operationalised in a nutritional planner that the dietitian and patient work on collaboratively. Together, they generate a weekly grid of nutritional behaviours, such as eating breakfast, conducting oral care of ulcers, or drinking a meal replacement supplement. When the patient is happy with the plan, both they and the dietitian sign it, and the dietitian takes a copy and they agree to review it the following week. The patient then ticks each behaviour as they complete it each day. This process makes the behaviours more likely through self-generation,29 self-monitoring,33 having a concrete meal plan,34 tailoring,35 achievability,36 reinforcement and accountability;37 all of which are CBT strategies that have been successful in nutritional behaviour change trials.38
Implementation of EAT
The intervention was developed to integrate with the Evidence Based Practice Guidelines for the Nutritional Management of Adult Patients with Head and Neck Cancer.39 While EAT is predominately a style of interaction, in order to maximise potential benefit for patients, it requires that (1) patients receive frequent contact with dietitians to enable sufficient exposure to the intervention; (2) ongoing dietitian's use of a validated nutrition assessment tool to enable the dietitian to present a patient's non-compliance with dietetic advice in a standard, objective, but non-confrontational way and that (3) patients at risk of depression be offered psychosocial support to reduce the risk that depressive symptoms do not hinder patient motivation and capacity to engage with dietitians or action nutritional plans agreed with dietitians during consultation. As such, during the intervention phase, sites receive a range of supportive clinical practice change strategies to facilitate the delivery of the EAT intervention in addition to the provision and/or maintenance of clinical practice guidelines recommendations regarding the frequency of dietitian contact during and after radiotherapy, the use of a validated nutritional assessment tool to assess and monitor nutritional adequacy of patients, and the screening and referral of patients at risk for psychosocial support. Specifically, the research team will provide sites with the following evidence-based, clinical practice change support strategies (box 1).
Box 1. Best practice clinical guidelines for patients with head and neck cancer.
Best practice clinical guidelines for patients with head and neck cancer recommend:
≥125 kJ/kg/day and 1.2 g protein/kg/day
Use of a validated nutritional assessment tool
Dietetic consults weekly, then fortnightly
Screening and referral for distress
Executive support and endorsement
Senior trial investigators will solicit the support and endorsement of executive staff from each site for the implementation of the EAT intervention and dietetic clinical guidelines.40–42 These trial investigators include clinical psychologists, an implementation scientist, and an expert opinion leader in the field of head and neck dietetic care, and author of the Evidence-based practice guidelines for the nutritional management of adult patients with head and neck cancer.39 Specifically, these members of the research team will meet via teleconference with the department head of dietetics and the principal investigator from the radiotherapy department at each participating site 2 weeks prior to training (described below). These executive site staff will be asked to demonstrate leadership and support for the EAT intervention and clinical guidelines, for example, by communicating their support for the clinical practice change and expectations of staff at the training workshops and throughout the intervention phase of the trial. These staff will also be asked to take responsibility for addressing any barriers to change arising at the executive level.
Provision of staff training
The workshop and booster session (described previously) will seek to enhance staff knowledge, skills and attitudes toward the EAT intervention and the best practice dietetic guidelines, and address barriers to such care provision identified in the literature. Specific to depression-screening recommendations, dietitians will be trained in a method used to screen for symptoms of depression using the Patient Health Questionnaire-2 (PHQ-2).43 The PHQ-2 consists of two key screening items from the larger PHQ-9 and has been shown to have good psychometric properties (ROC AUC=0.084) in a radiotherapy outpatients population.44 It asks the participant to rate the frequency of two major depressive episode criteria over the last 2 weeks from 0 to 3. This provides the clinician with an indication of whether the patient may be at risk of experiencing clinically significant symptoms of depression. Training will combine didactic and interactive components including opportunities for discussion, role play and facilitator-provided feedback. This approach is consistent with recommendations for effective training that facilitates learning.45 46
Academic detailing
Clinical psychologists from the research team will attend the radiotherapy department dietetic clinics to ‘shadow’ dietitians for 1 day following both the 2-day training workshop and the booster training session (2 months after initial training). The research staff will be guided in this process by the use of a checklist that clearly defines the educational and behavioural objectives of the EAT intervention and clinical guidelines. The clinical psychologists will (1) reinforce the essential messages using active dietitian participation, (2) informally assess intervention implementation, (3) help resolve implementation barriers and assist with the integration of systems changes specific to that clinic to support best practice dietetic intervention, (4) provide advice, feedback, support and positive reinforcement of improved practices to dietitians regarding patient care and (5) set explicit targets and develop an action plan with dietitians.47–49
Systems and prompts
To facilitate patient attendance for dietetic treatment, services will be encouraged to schedule outpatient appointments adjacent to radiotherapy appointments. Integrating dietetic management into radiotherapy in this way helps to position dietetic intervention and counselling as an integral part of cancer care for both the patients and the department staff. Dietitians will be asked to schedule patient consultations according to the recommendations of the clinical guidelines (weekly during radiotherapy, fortnightly for 6 weeks post-treatment, and ‘as required’ thereafter). Dietitians will be asked to record dietetic consultations in patient medical records. Consistent with recommendations for effective implementation of clinical guidelines into routine practice, the medical records of participating patients will include a coloured printed prompt, placed by research staff, to remind and guide dietitians in the key components of the EAT intervention. The PG-SGA and PHQ-2 will also be included in trial patients’ records to facilitate standardised nutrition assessment and depression screening as recommended by the clinical guidelines.50 For services without existing referral pathways for psychosocial support for patients with cancer, the research team will work with the dietitians and radiation oncologist at each site to collaboratively develop a referral policy for those patients screened as at risk for depression.
Performance audit and feedback
Patient medical records and audio recorded patient consultations will be audited regularly by study personnel to assess the provision of the EAT intervention behavioural change techniques and care consistent with the clinical guidelines. Consistent with recommendations for effective feedback and monitoring, feedback regarding site performance data relative to agreed benchmarks will be provided in written and verbal forms at multiple timepoints.48 49 The expert opinion leader in HNC nutritional management and the behavioural scientist from the research team will have regular phone meetings every 3–4 months with the head of the dietetics departments of the intervention sites to provide information about the current level of care provided by staff, relative to best practice guidelines and the EAT intervention. Reports providing aggregated data will be provided to the head of dietetics at each site prior to these calls at 3–4 month intervals after training. With permission of the head of dietetics, these reports will also be sent to site dietetic staff. During these calls, the expert opinion leader will review performance feedback using these reports, identify opportunities for improvement, assist with problem solving, agree on the goals for the next month including performance benchmarks, and set an action plan.48 The head of dietetics at the intervention site will be encouraged to implement strategies to improve care when it is found to be inconsistent with the EAT intervention components.
Additional support and feedback for the intervention will be provided as part of academic detailing, and through ongoing formal and informal supervision, with a clinical psychologist assisting with the implementation, barriers and maintenance of the system change. As part of these regular meetings, audio tapes of dietetic consultations with trial patients will be discussed. Those clinicians not meeting benchmarks will be encouraged to discuss potential impediments with the clinical psychologist during supervision.
Provision of tools and resources
Given identified barriers to implementation of clinical guidelines including lack of information and clinical uncertainty,50 51 services and staff will have access to well presented, user friendly EAT intervention manuals and print resources, nutrition assessment tools, depression-screening procedures and psychosocial referral options that will be provided during training, so as to facilitate discussion and practice.40 41 52 They will also have access to regular phone and videoconferences with the clinical psychologist and project manager to discuss barriers and solutions to implementation. Barriers to intervention implementation and any necessary resources required for training will be discussed during a teleconference with sites 2 weeks prior to training.
Treatment verification and delivery
Dietitians will be required to audio-record treatment sessions with participants and to use a monitoring form to document the number and frequency of their dietetic consultations.
A random selection of audio tapes pretraining and post-training, will be reviewed by two independent assessors for fidelity to the EAT manual. Fidelity will be assessed using the Behaviour Change Counselling Index,53 54 a standardised, evidence-based checklist for assessing behaviour change counselling skills. Following the EAT training, additional items will be added to assess the presence of specific components of the EAT intervention.
Assessments
Assessments of primary and secondary outcomes and covariates will be conducted by an independent research officer during the first and last weeks of radiotherapy (typically 6 weeks apart) and follow-up will occur 4 and 12 weeks after the completion of radiotherapy (table 1). As part of routine treatment, the Common Terminology Criteria for Adverse Events,55 mucositis (oral, pharyngeal and laryngeal) and dysphagia assessments will also be performed by the radiation oncologist.
Table 1.
Schedule of assessment measures
| First week of radiotherapy | Last week of radiotherapy | Four weeks after | Twelve weeks after | |
|---|---|---|---|---|
| Primary outcome | ||||
| Nutritional status assessment: PG-SGA | ✓ | ✓ | ✓ | ✓ |
| Secondary outcomes | ||||
| Depression: PHQ-9 | ✓ | ✓ | ✓ | ✓ |
| Quality of life: EORTC | ✓ | ✓ | ✓ | ✓ |
| Quality adjusted life years: EORTC | ✓ | ✓ | ✓ | ✓ |
| Covariates | ||||
| Therapeutic alliance: dietitian ARM-5 (clinician) |
✓ | ✓ | ✓ | |
| Therapeutic alliance: client ARM-5 (client) |
✓ | ✓ | ✓ | |
| Nicotine dependence: FTND | ✓ | ✓ | ✓ | |
| Alcohol dependence: AUDIT | ✓ | |||
| Alcohol use: AUDIT-consumption | ✓ | ✓ | ✓ | |
| Smoking: biochemical validation expired carbon monoxide |
✓ | ✓ | ✓ | |
| Dysphagia: Australian standard of food texture | ✓ | ✓ | ✓ | ✓ |
| Chart audit | ✓ | ✓ | ||
ARM-5, Agnew Relationship Measure—Five Item Version; AUDIT, The Alcohol Use Disorders Identification Test; EORTC, European Organisation for Research and Treatment of Cancer; FTND, The Fagerstrom Test for Nicotine Dependence; PG-SGA, Patient Generated Subjective Global Assessment; PHQ-9, The Patient Health Questionnaire 9.
Primary outcome: nutritional status
The PG-SGA56 57 is considered the gold standard in oncology nutrition. The assessment examines known prognostic indicators of nutrition such as weight change, dietary intake, gastrointestinal symptoms, changes in functional capacity, nutritional intake, metabolic stress, subcutaneous fat, muscle wasting, disease and treatment. It consists of a self-report questionnaire and clinical assessment conducted by a member of the study team. Higher scores reflect a higher risk of malnutrition.
Secondary outcomes
Depression: The PHQ-943 is a self-administered nine-item questionnaire that assesses depression. Participants are asked to rate (on a scale of 0–3) the frequency of various Major Depressive Episode criteria over the previous 2 weeks. It provides two pieces of information; whether the patient is likely to meet criteria for a major depressive episode, and a measure of the severity of the depression from 0 to 27.
Quality of Life: The European Organisation for Research and Treatment of Cancer Core Quality of Life Questionnaire (EORTC QLQ-C30) is a psychometrically validated58 30-item self-report questionnaire designed to measure quality of life in patients with cancer. The EORTC QLQ-C30 consists of five functional scales (physical, role, cognitive, emotional and social), three symptom scales (fatigue, pain and nausea and vomiting), a global health status scale, and six single items assessing the perceived financial impact of the disease and additional symptoms commonly reported by patients with cancer (dyspnoea, loss of appetite, insomnia, constipation and diarrhoea). Scale and individual item scores range 0–100. Higher scores reflect a higher response level—high functional scores indicate a high/healthy level of functioning; higher symptom scores reflecting higher symptomatology/problems; higher scores on individual items reflect stronger endorsement/experience of that item. The EORTC QLQ-C30 can also be used to generate quality adjusted life years for economic analyses.59 60
Other variables
Therapeutic alliance: This is measured by the Agnew Relationship Measure—Five Item Version—Patient Rated (ARM-561). This short questionnaire has been developed as a mechanism for assessing therapeutic alliance within busy clinical settings.61 The ARM5 comprises a single ‘core alliance’ domain consisting of items from the ARM bond, partnership and confidence domains. The ARM5 consists of a series of statements on parallel forms rated by clients and clinicians using a seven-point Likert scale anchored ‘strongly disagree’, ‘moderately disagree’, ‘slightly disagree’, ‘neutral’, ‘slightly agree’, ‘moderately agree’ and ‘strongly agree’. Clinicians and clients are asked to rate items ‘thinking about today's meeting’. An overall ‘core alliance’ scale is derived by calculating the mean of the five items, with higher scores reflecting stronger therapeutic alliance.
Nicotine dependence: The Fagerstrom Test for Nicotine Dependence62 is a six-item, reliable and valid self-report questionnaire designed to assess the strength of nicotine dependence. Item scores are summed to produce a total score, with higher scores indicating higher levels of nicotine dependence (0–2=very low; 3–4=low; 5=medium; 6–7=high; 8–10=very high dependence).
Expired carbon monoxide (CO) will provide biochemical verification of smoking status. Recent evidence suggests that as many as 30% of patients with HNC may misrepresent their tobacco use during treatment. The Micro 11 Smokerlyser will be used to assess breath levels of CO, with a level <10 ppm signifying abstinence from smoking.63
The Alcohol Use Disorders Identification Test (AUDIT64) is a ten item self-report measure developed by WHO to identify harmful patterns of alcohol use over the preceding 1 year (including harmful use, hazardous use and dependence). Items are summed to produce a total score, with scores over 8 indicating harmful or hazardous alcohol use, as well as possible alcohol dependence. Inspection of individual items can be used to further identify the nature of alcohol-related problems. Scores above zero on items 1–3 can signify risky or hazardous use; on items 4–6 (especially weekly or daily symptoms), scores above zero are indicative of the presence or incipience of alcohol dependence, while endorsement of items 7–10 demonstrates that alcohol-related harm is already occurring.65
The AUDIT-Consumption64 consists of the first three items of the AUDIT (frequency of use, typical consumption and frequency of six or more standard drinks), and provides an index of alcohol use. This brief questionnaire is a reliable indicator of heavy drinking and also demonstrates adequate sensitivity and specificity for detecting active alcohol abuse and dependence.64 It will be employed to detect changes in quantity and/or type of alcohol consumed across the 18 weeks of the trial, with reference to a 2-month time frame.
Dysphagia: The research officer will conduct a secondary assessment of dysphagia as it relates to nutrition using the Australian standard of food texture. The assessor will record the participant's ability to swallow to a standard level: unmodified (regular), texture A (soft), texture B (minced moist), texture C (smooth pureed), and to drink water without coughing or choking.
Chart review
Outcome and covariate data (table 2) will also be collected by a member of the study team during chart reviews conducted during the first week of radiotherapy and at 12-week follow-up.
Table 2.
Outcome and covariate data extracted during chart reviews
| Week one | Twelve weeks follow-up |
|---|---|
| Tumour site | Delivered radiotherapy dose, fractionation, start date, finish date and total treatment time |
| Tumour stage | Treatment interruption |
| Concurrent chemotherapy | Unplanned hospital visits and length of stay |
| Concurrent surgery | Tumour response |
| Proposed RT dose, fractionation and treatment time | Whether PHQ-2 follow-up was documented |
| Prophylactic PEG/nasogastric tube feeding placement and date inserted | Number and frequency of dietetic consults |
| Whether PHQ-2 screening was documented | Whether PG-SGA/formal nutritional assessment was documented in the final week of treatment and the score |
| Whether PG-SGA/formal nutritional assessment was documented in the first week of treatment and the score | Complications with PEG/date of removal of PEG if removed |
| Whether a PEG or nasogastric tube feeding was used for alimentation during treatment or post treatment and date inserted and removed | |
| The dates and dosage of all medications/treatments received as part of another clinical trial |
PEG, Percutaneous endoscopic gastrostomy; PG-SGA, Patient Generated Subjective Global Assessment; PHQ-2, The Patient Health Questionnaire 2; RT, radiotherapy.
Chart audit
A chart audit will also be conducted on those patients who met the three key screening criteria but were not enrolled in the study. A summary of the following variables will be generated to allow for any recruitment or drop-out bias to be controlled for in analysis: standard demographics; tumour site, stage and response; proposed and delivered concurrent chemotherapy; concurrent surgery; number and frequency of dietetic consults; unplanned hospital visits, length of stay; prescribed and delivered radiotherapy dose, fractionation, treatment time and treatment interruption(s); whether a percutaneous endoscopic gastrostomy or nasogastric tube was used prophylactically, or for alimentation during treatment or post-treatment; and mortality data.
Sample size
The target sample size for this trial will be 400 (approximately 80 participants per recruitment hospital). This sample size calculation was based on a t test using the Harvard Biostatistics Massachusetts General Hospital Biostatistics Power and Sample Size Calculator, providing 80% probability that the study will detect a treatment difference at a two-sided 0.05 significance level with a minimum important difference of two units on the PG-SGA, assuming the SD is 7.
Statistical analysis
The primary outcome of nutritional status as measured by the PG-SGA will be analysed using a Generalised Linear Mixed Model to take account of the repeated measurements on subjects over time (assessment moment). The model will include the cluster-level variables of intervention (pre and post) and hospital. Individual-level variables in the model will be baseline nutritional status as measured by the PG-SGA, calendar time, assessment moment, as well as tumour site and tumour stage. A random effect for individual will be included in the model as well as a random effect for assessment moment, as the variation in PG-SGA is likely to be much greater at the assessment moment during the patient’s treatment phase. Finally, an interaction term for intervention by assessment moment will be included in the model to allow the treatment effect to vary over time.
Registration
The trial is registered with the Australian New Zealand Clinical Trials Registry with the number ACTRN12613000320752.
Discussion
The present study is significant in that it addresses the issue of malnutrition during radiotherapy, a major risk factor for morbidity and mortality in patients with HNC. Although mucosal cancers of the head and neck have traditionally accounted for approximately 3%2 of all cancer diagnoses, the frequency of this diagnosis has increased exponentially in recent years. Radiotherapy plays a major role in the management of these patients, often in association with surgery or chemotherapy. This is the first study to evaluate a dietitian-delivered behaviour change intervention (EAT) based on MI and CBT to maintain or improve nutritional status among patients with HNC. The results of the proposed trial are expected to make a significant contribution to dietetic clinical practice, the training of future oncology dietitians, and ultimately, to reducing the mortality of patients with HNC.
Importantly, this study brings together existing research, clinical experience and promising pilot data collected by the research team. It is a collaboration between investigators internationally recognised in their respective fields of oncology, psychiatry, dietetics, health behaviour and systems change, working towards better outcomes for this challenging and often overlooked cancer population.
Acknowledgments
The authors would like to acknowledge the support of The Trans Tasman Radiation Oncology Group (TROG) and The Calvary Mater Newcastle Nutrition and Dietetics Department.
Footnotes
Contributors: Development of the manuscript was led by BB. The intervention was developed and piloted by BB, AB, GC and CW. Funding was secured by BB, AB, JB, CW, LW and GC. Trial design refinement and sample size calculation were determined by PM and BB. Clinical practice change elements were integrated into the trial by KM, SH and LW. The trial will be coordinated by AB. All authors approved the final version of the manuscript.
Funding: National Health and Medical Research Council (APP1021018; 2011/3654).
Competing interests: None declared.
Patient consent: Obtained.
Ethics approval: The study protocol has received approval from the Hunter New England Human Research Ethics Committee (HREC) of Hunter New England Health (HREC/12/HNE/108; HNEHREC: 12/04/18/4.06). Approval has also been received from the following committees: Central Adelaide Local Health Network (HREC/13/RAH/75; SSA/13/RAH/102); Sir Charles Gairdner Group HREC (2012-136); Peter MacCallum Cancer Centre Ethics (SSA/13/PMCC/19); Western Sydney Local Health District Research Governance (SSA/13/WMEAD/110); Metro South Hospital and Health Service (SSA/13/QPAH/240 and SSA/13/QPAH/241).
Provenance and peer review: Not commissioned; peer reviewed for ethical and funding approval prior to submission.
References
- 1.Ferlay J, Shin HR, Bray F et al. . GLOBOCAN 2008 v2.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 10 [Internet]. 02-Jan-2010. [Online]. http://globocan.iarc.fr/ (accessed 2 Jan 2013).
- 2.Tracey E, Kerr T, Dobrovic A et al. . Cancer in NSW: incidence and moratility report 2008. Sydney: cancerinstitute.org.au, 2008. [Google Scholar]
- 3.Kruizenga HM, Wierdsma NJ, Van Bokhorst M et al. . Screening of nutritional status in The Netherlands. Clin Nutr 2003;22:147–52. 10.1054/clnu.2002.0611 [DOI] [PubMed] [Google Scholar]
- 4.Lees J. Incidence of weight loss in head and neck cancer patients on commencing radiotherapy treatment at a regional oncology centre. Eur J Cancer Care 1999;8:133–6. 10.1046/j.1365-2354.1999.00156.x [DOI] [PubMed] [Google Scholar]
- 5.Larsson M, Hedelin B, Johansson I et al. . Eating problems and weight loss for patients with head and neck cancer: a chart review from diagnosis until one year after treatment. Cancer Nurs 2005;28:425–35. 10.1097/00002820-200511000-00004 [DOI] [PubMed] [Google Scholar]
- 6.Fesinmeyer MD, Mehta V, Blough D et al. . Effect of radiotherapy interruptions on survival in medicare enrollees with local and regional head-and-neck cancer. Int J Radiat Oncol Biol Phys 2010;78:675–81. 10.1016/j.ijrobp.2009.08.004 [DOI] [PubMed] [Google Scholar]
- 7.O'Connor P. The impact of missed fractions in head and neck radiotherapy and how they can be minimised. Radiography 2013;19:343–46. [Google Scholar]
- 8.Murphy BA. Clinical and economic consequences of mucositis induced by chemotherapy and/or radiation therapy. J Support Oncol 2007;5(10 Suppl 5):1–9. [PubMed] [Google Scholar]
- 9.van Leeuwen PA, Kuik DJ, Klop WM et al. . The impact of nutritional status on the prognoses of patients with advanced head and neck cancer. Cancer 1999;86:519–27. [DOI] [PubMed] [Google Scholar]
- 10.Colasanto JM, Prasad P, Nash MA et al. . Nutritional support of patients undergoing radiation therapy for head and neck cancer. Oncology (Williston Park) 2005;19:371–9; discussion 380–2–387. [PubMed] [Google Scholar]
- 11.de Graeff A, de Leeuw RJ, Ros WJ,et al. . A prospective study on quality of life of laryngeal cancer patients treated with radiotherapy. Head Neck 1999;21:291–6. [DOI] [PubMed] [Google Scholar]
- 12.Britton B, Clover K, Bateman L et al. . Baseline depression predicts malnutrition in head and neck cancer patients undergoing radiotherapy. Support Care Cancer 2012;20:335–42. 10.1007/s00520-011-1087-y [DOI] [PubMed] [Google Scholar]
- 13.Dropkin MJ. Anxiety, coping strategies, and coping behaviors in patients undergoing head and neck cancer surgery. Cancer Nurs 2001;24:143–8. 10.1097/00002820-200104000-00010 [DOI] [PubMed] [Google Scholar]
- 14.De Boer MF, McCormick LK, Pruyn JF et al. . Physical and psychosocial correlates of head and neck cancer: a review of the literature. Otolaryngol Head Neck Surg 1999;120:427–36. 10.1016/S0194-5998(99)70287-1 [DOI] [PubMed] [Google Scholar]
- 15.Degenhardt L, Hall W, Lynskey M. Alcohol, cannabis and tobacco use among Australians: a comparison of their associations with other drug use and use disorders, affective and anxiety disorders, and psychosis. Addiction 2001;96:1603–14. 10.1046/j.1360-0443.2001.961116037.x [DOI] [PubMed] [Google Scholar]
- 16.Browman GP, Wong G, Hodson I. Influence of cigarette smoking on the efficacy of radiation therapy in head and neck cancer. N Engl J Med 1993;328:159–63. 10.1056/NEJM199301213280302 [DOI] [PubMed] [Google Scholar]
- 17.Rugg T, Saunders MI, Dische S. Smoking and mucosal reactions to radiotherapy. Br J Radiol 2014;63:554–6. 10.1259/0007-1285-63-751-554 [DOI] [PubMed] [Google Scholar]
- 18.Porock D, Nikoletti S, Cameron F. The relationship between factors that impair wound healing and the severity of acute radiation skin and mucosal toxicities in head and neck cancer. Cancer Nurs 2004;27:71 10.1097/00002820-200401000-00009 [DOI] [PubMed] [Google Scholar]
- 19.Gritz ER. Smoking and smoking cessation in cancer patients. Addiction 1991;86:549–54. 10.1111/j.1360-0443.1991.tb01806.x [DOI] [PubMed] [Google Scholar]
- 20.Duffy SA, Ronis DL, McLean S et al. . Pretreatment Health Behaviors Predict Survival Among Patients With Head and Neck Squamous Cell Carcinoma. J Clin Oncol 2009;27:1969–75. 10.1200/JCO.2008.18.2188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Duffy SA, Terrell JE, Valenstein M et al. . Effect of smoking, alcohol, and depression on the quality of life of head and neck cancer patients. Gen Hosp Psychiatry 2002;24:140–7. 10.1016/S0163-8343(02)00180-9 [DOI] [PubMed] [Google Scholar]
- 22.Jerjes W, Upile T, Radhi H et al. . The effect of tobacco and alcohol and their reduction/cessation on mortality in oral cancer patients: short communication. Head Neck Oncol 2012;4:6 10.1186/1758-3284-4-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chen AM, Chen LM, Vaughan A et al. . Tobacco smoking during radiation therapy for head-and-neck cancer is associated with unfavorable outcome. Int J Radiat Oncol Biol Phys 2011;79:414–19. 10.1016/j.ijrobp.2009.10.050 [DOI] [PubMed] [Google Scholar]
- 24.Luckett T, Britton B, Clover K et al. . Evidence for interventions to improve psychological outcomes in people with head and neck cancer: a systematic review of the literature. Support Care Cancer 2011;19:871–81. 10.1007/s00520-011-1119-7 [DOI] [PubMed] [Google Scholar]
- 25.Garg S, Yoo J, Winquist E. Nutritional support for head and neck cancer patients receiving radiotherapy: a systematic review. Support Care Cancer 2010;18:667–77. 10.1007/s00520-009-0686-3 [DOI] [PubMed] [Google Scholar]
- 26.Isenring EA, Capra S, Bauer JD. Nutrition intervention is beneficial in oncology outpatients receiving radiotherapy to the gastrointestinal or head and neck area. Br J Cancer 2004;91:447–52. 10.1038/sj.bjc.6601962 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ravasco P, Monteiro-Grillo I, Vidal PM et al. . Cancer: disease and nutrition are key determinants of patients’ quality of life. Int J Radiat Oncol Biol Phys 2004;12:246–52. [DOI] [PubMed] [Google Scholar]
- 28.Odelli C, Burgess D, Bateman L et al. . Nutrition support improves patient outcomes, treatment tolerance and admission characteristics in oesophageal cancer. Clin Oncol 2005;17:639–45. 10.1016/j.clon.2005.03.015 [DOI] [PubMed] [Google Scholar]
- 29.Miller WR, Rollnick S. Motivational Interviewing. 3rd edn. New York: Guilford Publication, 2012. [Google Scholar]
- 30.Baker A, Lee NK, Claire M et al. . Brief cognitive behavioural interventions for regular amphetamine users: a step in the right direction. J Am Diet Assoc 2005;100:367–78. [DOI] [PubMed] [Google Scholar]
- 31.Hussey MA, Hughes JP. Design and analysis of stepped wedge cluster randomized trials. Contemporary Clinical Trials 2007;28:182–91. [DOI] [PubMed] [Google Scholar]
- 32.Hettema JE, Miller WR. Hettema: A meta-analysis of motivational interviewing…—Google Scholar. Alcoholism- 2004.
- 33.Tate DF, Jackvony EH, Wing RR. Effects of internet behavioral counseling on weight loss in adults at risk for type 2 diabetes: a randomized trial. JAMA 2003;289:1833–6. 10.1001/jama.289.14.1833 [DOI] [PubMed] [Google Scholar]
- 34.Wing R, Jeffrey R, Burton L et al. . Food provision vs structured meal plans in the behavioral treatment of obesity. Int J Obes Relat Metab Disord 1996;20:56–62. [PubMed] [Google Scholar]
- 35.Clark M, Hampson SE, Avery L et al. . Effects of a tailored lifestyle self-management intervention in patients with Type 2 diabetes. Br J Health Psychol 2004;9:365–79. 10.1348/1359107041557066 [DOI] [PubMed] [Google Scholar]
- 36.Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 1977;84:191–215. 10.1037/0033-295X.84.2.191 [DOI] [PubMed] [Google Scholar]
- 37.Beck JS. Cognitive behavior therapy. 2nd edn. Guilford Press, 2011. [Google Scholar]
- 38.Spahn JM, Reeves RS, Keim KS et al. . State of the evidence regarding behavior change theories and strategies in nutrition counseling to facilitate health and food behavior change. J Am Diet Assoc 2010;110:879–91. 10.1016/j.jada.2010.03.021 [DOI] [PubMed] [Google Scholar]
- 39.Findlay M, Bauer J, Brown T. Head and Neck Guideline Steering Committee. In: Head and Neck Guideline Steering Committee. Evidence-based practice guidelines for the nutritional management of adult patients with head and neck cancer. httpwiki.cancer.org.auaustraliawikiindex.phpoldid, 10-Sep-2014. [Online]. http://wiki.cancer.org.au/australia/COSA:Head_and_neck_cancer_nutrition_guidelines (accessed 10 Sep 2014).
- 40.Bero LA, Grilli R, Grimshaw JM et al. . Getting research findings into practice: closing the gap between research and practice: an overview of systematic reviews of interventions to promote the implementation of research findings. BMJ 1998;317:465 10.1136/bmj.317.7156.465 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Rohrbach LA. Type II translation: transporting prevention interventions from research to real-world settings. Eval Health Prof 2006;29:302–33. 10.1177/0163278706290408 [DOI] [PubMed] [Google Scholar]
- 42.Damschroder LJ, Aron DC, Keith RE et al. . Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci 2009;4:50 10.1186/1748-5908-4-50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatric Annals 2002;32:1–7. 10.3928/0048-5713-20020901-06 [DOI] [Google Scholar]
- 44.Small W, Pugh S, Wagner L et al. . RTOG 0841: two-item questionnaire effectively screens for depression in cancer patients receiving radiation therapy. Int J Radiat Oncol Biol Phys 87(2):S2. [Google Scholar]
- 45.Read CW, Kleiner BH. Which training methods are effective? Manag Dev Rev 1996;9:24–9. 10.1108/09622519610111781 [DOI] [Google Scholar]
- 46.O'Brien MT, Freemantle N, Oxman AD et al. . Continuing education meetings and workshops: effects on professional practice and health care outcomes (Cochrane review). J Contin Educ Health Prof 2005;21:187–8. [Google Scholar]
- 47.Soumerai SB. Principles of educational outreach (‘academic detailing’) to improve clinical decision making. JAMA 1990;263:549–56. 10.1001/jama.1990.03440040088034 [DOI] [PubMed] [Google Scholar]
- 48.Ivers N, Jamtvedt G, Flottorp S et al. . Audit and feedback: effects on professional practice and healthcare outcomes. Chichester, UK: John Wiley & Sons, Ltd, 1996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Alvero AM, Bucklin BR, Austin J. An objective review of the effectiveness and essential characteristics of performance feedback in organizational settings (1985–1998). J Organ Behav Manag 2001;21:3–29. [Google Scholar]
- 50.Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet 2003;362:1225–30. 10.1016/S0140-6736(03)14546-1 [DOI] [PubMed] [Google Scholar]
- 51.Turner J, Zapart S, Pedersen K et al. . Clinical practice guidelines for the psychosocial care of adults with cancer. Psychooncology 2005;14:159–73. 10.1002/pon.897 [DOI] [PubMed] [Google Scholar]
- 52.Giguère A, Légaré F, Grimshaw J et al. . Printed educational materials: effects on professional practice and healthcare outcomes. Chichester, UK: John Wiley & Sons, Ltd, 1996. [Google Scholar]
- 53.Lane C, Huws-Thomas M, Hood K et al. . Measuring adaptations of motivational interviewing: the development and validation of the behavior change counseling index (BECCI). Patient Educ Couns 2005;56:166–73. 10.1016/j.pec.2004.01.003 [DOI] [PubMed] [Google Scholar]
- 54.Lane C. The Behaviour Change Counselling Index (BECCI), Manual for Coding Behaviour Change Counselling, 2002.
- 55.Hong YS, Kim TW. Chemotherapy for Colorectal Cancer. J Korean Med Assoc 2010;53:582 10.5124/jkma.2010.53.7.582 [DOI] [Google Scholar]
- 56.Ottery FD. Definition of standardized nutritional assessment and interventional pathways in oncology. Nutrition (Burbank, Los Angeles County, Calif) 1996;12:S15–19. 10.1016/0899-9007(95)00067-4 [DOI] [PubMed] [Google Scholar]
- 57.Bauer J, Capra S, Ferguson M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur J Clin Nutr 2002;56:779–85. 10.1038/sj.ejcn.1601412 [DOI] [PubMed] [Google Scholar]
- 58.Bjordal K, Hammerlid E, Ahlner-Elmqvist M et al. , for the European Organization for Research, and T. O. C. Q. O. L. S. Group. Quality of life in head and neck cancer patients: validation of the European organization for research and treatment of cancer quality of life questionnaire-H&N35. J Clin Oncol 1999;17:1008. [DOI] [PubMed] [Google Scholar]
- 59.King M, Costa D, Aaronson NK et al. . PCN98 The Development of an Internationally-Valid Cancer-Specific Multi-Attribute Utility Instrument (MAUI) From the Eortc Core Health-Related Quality of Life (HRQOL) Questionnaire, QLQ-C30. Value Health 2012;15:A225 10.1016/j.jval.2012.03.1215 [DOI] [Google Scholar]
- 60.Rowen D, Brazier J, Young T et al. . Deriving a preference-based measure for cancer using the EORTC QLQ-C30. Value Health 2011;145721–731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Cahill J, Stiles WB, Barkham M et al. . Two short forms of the Agnew Relationship Measure: the ARM-5 and ARM-12. Psychother Res 2012;22:241–55. 10.1080/10503307.2011.643253 [DOI] [PubMed] [Google Scholar]
- 62.Heatherton TF, Kozlowski LT, Frecker RC et al. . The Fagerström Test for Nicotine Dependence: a revision of the Fagerstrom Tolerance Questionnaire. Addiction 1991;86:1119–27. 10.1111/j.1360-0443.1991.tb01879.x [DOI] [PubMed] [Google Scholar]
- 63.Benowitz NL, Jacob P, Hall S et al. . Biochemical verification of tobacco use and cessation. Nicotine Tob Res 2002;4:149–59. 10.1080/14622200210123581 [DOI] [PubMed] [Google Scholar]
- 64.Bush K, Kivlahan DR, McDonell MB et al. . The AUDIT Alcohol Consumption Questions (AUDIT-C): an effective brief screening test for problem drinking. Arch Intern Med 1998;158:1789–95. 10.1001/archinte.158.16.1789 [DOI] [PubMed] [Google Scholar]
- 65.Babor T, Higgins-Biddle J. The alcohol use disorders identification test. World Health Organisation, 2001. [Google Scholar]