

In Brief
The growing older adult population and its higher incidence of diabetes are creating demands on health care providers to address the special needs of these patients. Because nutrition is essential to the proper treatment and self-management of diabetes, clinicians must develop and adopt various strategies to address some of the common nutritional, lifestyle, and self-management barriers that older adults face. Nutrition assessments of older adults with diabetes should be comprehensive, with attention to each patient’s unique nutritional needs. Constructing a realistic nutrition care plan is essential for success. This article addresses some of the key nutrition-related aspects of diabetes self-care in older adults with diabetes.
Diabetes in Older Adults
Etiology of type 2 diabetes in older adults
The incidence of type 2 diabetes in older adults is attributable to two primary factors: 1) changes in metabolism (e.g., increased insulin resistance and decreased insulin production) and 2) changes in weight and physical activity. The development of glucose intolerance is a recognizable metabolic change that occurs during aging, and some degree of glucose intolerance is normal later in life, even in otherwise healthy people. Studies have reported increases of 5.3 mg/dl in postprandial glucose levels and 1–2 mg/dl in fasting glucose levels for every decade of life after the age of 30 years.1
The etiology of glucose intolerance in older adults is multifaceted. Factors such as slower glucose absorption, altered gluconeogenesis, decreased insulin production, reduced lean body mass, decreased physical activity, and altered digestion all contribute to reduced glucose utilization.2 Alterations in physical activity in older adults are common and often related to physical limitations, conditions such as atherosclerosis, and an increased risk of injury.3 In addition, many people in this age category also have one or more chronic health condition requiring prescription and nonprescription medications that may affect glucose metabolism.1,4
Identifying diabetes and diabetes risk in older adults
Although it is widely known that older adults are a high-risk group, diagnosis of diabetes in this population can be difficult. Despite American Diabetes Association (ADA) recommendations about the importance of routine screening for diabetes in the U.S. adult population,5 diabetes in older adults is often diagnosed after random glucose testing for nonrelated medical conditions or during an inpatient admission.1
Aside from the ADA, few organizations have published specific recommendations for the frequency of diabetes testing in older adults. The ADA recommends screening every 3 years for adults > 45 years of age, but there are no recommendations for increasing the frequency of testing in patients > 65 years of age, despite the expected changes in insulin sensitivity associated with increasing age. Rather, the association’s 2012 consensus report on diabetes in older adults states that the benefit of identifying prediabetes or asymptomatic type 2 diabetes in older adults depends on whether interventions would be effective.6 Additionally, few organizations have ventured to define nutrition screening parameters for older adults. A lack of routine screenings may contribute to nutrition-related and metabolic diagnoses being made during acute hospitalizations.
Older adults may neglect primary care check-ups to see specialists for other conditions; thus, all health care professionals (HCPs) should be educated about the need for diabetes screening in this population. Older adults are also likely to under-report the presence of common diabetes symptoms, contributing to delays in diagnosis. Classic symptoms of diabetes—polyuria, polydipsia, and fatigue—may be masked or inappropriately interpreted as symptoms of aging. Similarly, mild dehydration detected in the elderly may be caused by aging-related changes in the thirst response, lack of proper fluid intake, medications, or hyperglycemia.
As with other symptoms, weight changes are not always detected by older adults who may not weigh themselves regularly because of physical impairment, visual impairment, or a lack of concern regarding their cosmetic appearance. However, weight imbalances, whether under- or over-weight, are predictive of an increasing risk for diabetes in adults 60–79 years of age.7,8 This article addresses some of the nutrition-related issues involved in diabetes treatment and self-care in older adults with diabetes.
Treatment approach to diabetes in older adults
The ADA encourages individualized treatment goals and suggests less intensive targets for those who already have advanced diabetes complications or significant cognitive and physical impairments.9,10 For younger adults, glycemic targets are focused on reducing future complications. However, research suggests that older adults are more likely to develop diabetes-related complications and at a more accelerated rate.4
Typical diabetes treatment plans involving dietary restrictions, increasing physical activity, and pharmaceutical interventions may, in fact, lead to additional health risks in older adults. Hypoglycemia, undesirable weight loss, and falls may contribute to undesirable health outcomes.10,11 Nutrition interventions in this population are especially important in that they may help prevent such risks with a low likelihood of causing additional problems.
Nutrition Interventions in Older Adults
Nutrient needs
Regardless of age, the nutrient needs of individual patients must be identified and met when developing a plan for medical nutrition therapy. When appropriate, a registered dietitian (RD) should be consulted to help with designing a plan based on individual needs. In the older adult population, calculated caloric needs may be less accurate using weight-based formulas alone because of the physiological changes (i.e., less lean body mass) associated with aging. The Dietary Guidelines for Americans 201012 suggest estimated caloric levels for sex/age/activity levels rounded to the nearest 200 calories. It is advised that individual caloric needs may be higher than the estimates provided. These guidelines recommend approximately 2,000–2,600 kcal for men ≥ 65 years of age, depending on their activity level, and 1,600–2,000 kcal for women in the same age-group.12
The Institute of Medicine (IOM) provides a comprehensive reference list of nutrient needs for older adults who are 51–70 or > 70 years of age.13 Dietary protein recommendations to reduce sarcopenia and support optimal musculoskeletal health for older adults vary. The current recommended daily allowance for protein for adults is 0.8 g/kg/day, but recommendations have been published advocating 1.0–1.6 g/kg/day and even 25–30 g of high-quality protein per meal for older adults.14
Although older adults experience an aging-related reduction in lean body mass, there are no recommended modifications for the distribution of macronutrients. Therefore, there are no specific adjustments recommended for the caloric distribution for carbohydrate compared to younger adults, and there is a notable lack of research to define recommended fat intake in older adults. Despite this, there is evidence that measures to prevent cardiovascular complications have resulted in a greater reduction in morbidity and mortality than intensive glycemic management in the older-adult population.9 Thus, it would seem prudent to include heart-healthy guidelines within the nutrition plans of older adults with diabetes and thus continue to follow the general recommendations for modified fat intake.
In terms of micronutrient recommendations, intake of vitamin D, vitamin B6, chromium, and iron (for women only) differs from those for younger adults and from those adults > 70 years of age (Table 1).13
Table 1.
Micronutrient Modifications for Older Adults13
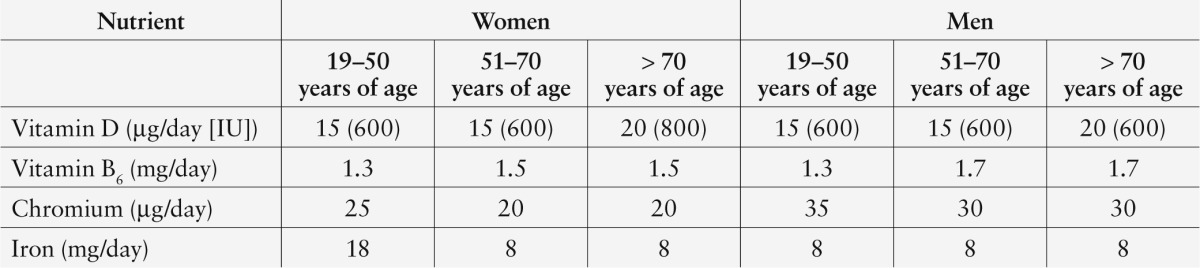
Dietary fiber recommendations are lower for adults > 50 years of age than for younger adults. In some older adults, higher-fiber foods may be avoided because of difficulties with chewing and digestion. If estimated dietary fiber needs (21 g/day for women > 50 years of age and 30 g/day for men > 50 years of age) are not achieved, fiber should be gradually increased to reduce symptoms of intolerance until the goal is met. Intolerance symptoms may present as increased intestinal gas, abdominal bloating, abdominal pain, or diarrhea.
Recommended fluid needs for adult men and women do not vary according to the dietary reference intake (DRI) with increasing age.14 Current DRI recommendations are for ∼ 3.7 l/day for men and 2.7 l/day for women. Fluid intake should be monitored to ensure proper hydration and prevent hyperosmotic nonketotic syndrome because a decreased thirst response is common in older adults. Mobility and toileting issues may also discourage frail adults from seeking out fluids between meals. Adjustments to the meal prescription (e.g., increased fiber intake) and changes in medical condition (e.g., nephropathy) may warrant modifications to fluid recommendations and closer monitoring.
Body weight considerations
One significant difference in nutrition goals for older adults concerns body weight. Although weight loss is typically prescribed for younger adults with diabetes or prediabetes, aggressive weight loss therapies are not recommended in the older adult population. Unintentional weight loss increases morbidity and mortality in older adults.15 Research indicates that weight loss and caloric restriction (a deficit compared to estimated daily metabolic needs) should not be encouraged in older adults with diabetes.8,15–18 The goal in this population is to maintain a reasonable weight, with weight loss being implemented with caution as part of the overall nutrition care plan. Determining the need for weight loss based on estimated body composition charts that are not age-specific is challenging because of the natural reductions in lean body mass in older adults and often lack of an accurate weight history. Additionally, determining weight management needs is not effective when based only on a random office scale weight without a weight history from home. However, mobility, stability, and vision difficulties can be barriers to accurate self-measurement of weight for older adults. Furthermore, commercially available weight charts for older adults may not be evidence-based. Therefore, clinicians should assess the need for weight management based on individual patients and their related comorbidities.
Nutrition Goals and Care Planning for Older Adults
Nutrition goals
Nutrition goals for older adults with diabetes are aimed at meeting macro- and micronutrient needs, achieving adequate hydration, and maintaining a reasonable weight. Older adults’ glycemic goals may be modified from those of younger adults; therefore, a liberalization of diet restrictions may be possible. It is important to meet macro- and micronutrient needs to avoid problems such as impaired immune functioning, anemia, and osteoporosis in the older adult population. Use of supplements, protein, or calorie boosters may be necessary at times to help these patients maintain weight, prevent hypoglycemia, and correct nutrient deficits. Clinical data that can be helpful in determining nutrition care planning for this population include albumin, hemoglobin, and transferrin measurements.6
Care planning
Individualization is the recognized standard approach when developing a medical nutrition care plan for any patient. This is even more important for older adults because of the physiological, cognitive, and lifestyle changes that often occur in the later stages of the lifespan. Additional educational and treatment barriers may be present and are important to address to support quality of life.8
Food habits are established early in life and are created through a variety of influences. Geographical, cultural, ethnic, religious, financial, and psychosocial factors all contribute to patients’ food preferences. For older adults with long-established behaviors, nutrition recommendations that restrict food selections or longstanding food practices may be immediately rejected. Eating food also may be one of the biggest pleasures in the daily routine of older adults. Clinicians should therefore create nutrition care plans that do not drastically alter established habits. Follow-up sessions allow for reinforcement of positive lifestyle changes, provision of additional education, and modification of the nutrition plan as needed.
Nutrition care plans may be implemented using a variety of approaches from a simple plate method to more advanced methods such as carbohydrate counting or calculating insulin-to-carbohydrate ratios. Barriers to adherence may include dementia, physical impairments, depression, financial and transportation restrictions, and the existence of other medical complications.18 To overcome such barriers, patients may require assistance for food acquisition, food preparation, and adequate intake. There is no strong evidence demonstrating that the approach of eating small, frequent meals offers any advantage over other approaches in this population. Instead, individualized management strategies should be employed to meet individual patients’ needs.
Mealtimes may be the most variable in this population because of depression, social isolation, sleep abnormalities, lack of a daily schedule, and poor appetite. About 29% of all older adults live alone, and ∼ 50% of older women live alone, according to 2011 U.S. Census reports.19 Social isolation may impair access to food sources and appetite and limit variety in food intake. Social issues can become significant barriers if not addressed when developing nutrition care plans. Referrals to meal delivery services, food assistance programs, group eating centers, and other social services may be necessary to achieve even the most basic goal of eating on a regular schedule.
Nutrition Assessment of Older Adults
Older adults with diabetes should undergo a comprehensive nutrition assessment to identify potential barriers to the care plan. Many older adults are challenged when trying to select proper food choices because of the existence of multiple nutrition recommendations for health conditions and guidelines for medication efficacy. They may feel overwhelmed with recommendations. Physical and mental condition, medication use, and overall health status can change suddenly and frequently during the course of a year in older adults. Nutrition care plans need to be reassessed regularly and should be modified based on changes in patients’ health status or lifestyle.
Food history
Obtaining a detailed and accurate food intake history may not be accomplished easily for patients with cognitive dysfunction or memory disorders.14,16,20 Cognitive decline and accelerated aging may be more significant in individuals with diabetes, with or without good glycemic control.14,16,21 Food intake recall data indicate that only one-third of older adults meet the goal of consuming five servings of fruits and vegetables per day, and one-half drink milk only once per day.17
Obtaining a food intake history may be facilitated by asking questions about food frequency rather than meal recall. Food pictures arranged in an album may be a useful memory stimulator. Family members can assist with the food history by bringing in photos of a patient’s actual plates of food at the home table. Photos taken before and after meals can also help to quantify the amounts of food actually consumed. An individual’s weekly grocery receipts showing itemized food purchases are another convenient source of data when gathering intake information.
Physiological changes
Changes in physiology that occur naturally in aging may affect nutritional status and glycemic control (Table 2). Because of age-related changes in the gastrointestinal tract, older adults may experience symptoms of dysphagia, anorexia, indigestion, and satiety issues or have bowel disturbances more frequently than younger adults.22 These symptoms may be acute or chronic and warrant interventions.
Table 2.
Physiological Changes Relevant to Nutrition Care in Older Adults
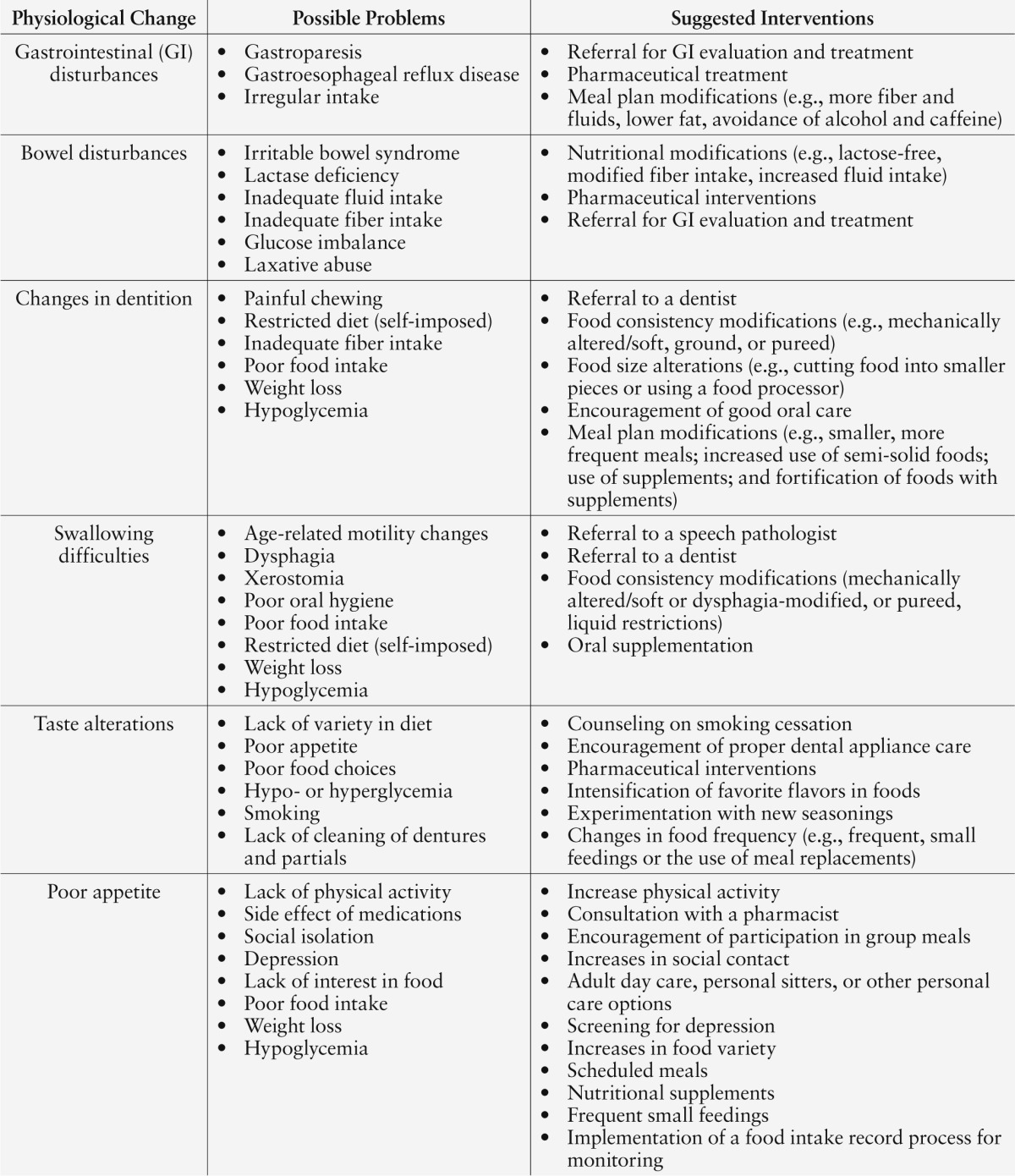
Swallowing disorders may be a result of aging, degenerative neurological disease, or mechanical issues.23 One study reported that ∼ 23% of individuals ≥ 65 years of age are edentulous.22 Additionally, individuals may not regularly wear dental appliances even if they have them, and this can contribute to swallowing difficulties and increased oral cavity sensitivity, resulting in impaired food intake and hypoglycemia. Decreased saliva product (xerostomia) as a result of aging or as a side effect from a medication can also inhibit natural swallowing. Clinicians should inquire about dentition and swallowing abilities when investigating causes for poor food intake, especially when poor intake results in hypoglycemia. Referrals to other HCPs such as dentists, otolaryngologists, and speech pathologists may be more appropriate than adjustments in medications or the nutrition care plan to reduce hypoglycemia and improve glycemic control.
The immune systems of older adults may be impaired because of medical conditions, medical treatments, or natural aging. This places older adults at higher risk for contracting food-borne illnesses. Sometimes, older adults on limited incomes are hesitant to discard food (e.g., food with spoilage or that has been in the refrigerator too long) in an effort to be thrifty. For these reasons, general food safety should be reviewed periodically. The U.S. Department of Agriculture Food Safety and Inspection Service website provides fact sheets and online resources for counseling on these issues.24
Dementia is another significant barrier to self-care for older adults suffering from neurological or cognitive changes. The interrelationship between diabetes and dementia is not well understood. One recent study suggested that the presence of diabetes, as well as poor diabetes control, are associated with worse cognitive function and greater decline.21 Dementia may precipitate behaviors such as skipping meals, selecting poor food choices, and making other diabetes-management errors. Interventions such as meal delivery services, group meals, and assistance from caregivers can be coordinated. Individuals with even mild dementia may need simplified menus and recipes as part of their nutrition counseling.
Medication history
Polypharmacy is common in the older adult population. Clinicians should regularly check for potential food/drug interactions, especially for medications affecting appetite or causing dry mouth. When appropriate, a pharmacist can be consulted to assist with such medication reviews. Review of medication history and meal timing and frequency should be conducted regularly because changes to prescription regimens may require updated planning to coordinate meals and medication doses.
Food insecurity
Financial barriers may impede some older adults’ ability to acquire healthful foods and may limit their self-care. Markers of possible food insecurity include a lack of food in the home, frequent hypoglycemia, substitution of habitual foods, weight loss, and residence in known food deserts (geographical areas in which affordable healthful foods are not readily available).25 Patients with such issues may require referral to social services, food assistance programs, food banks, and free community meal programs.
Federal programs such as the Older Americans Act (Title III), Supplemental Nutrition Assistance Program, and Senior Farmer’s Market Nutrition Programs are available.25 Directories for such services can be found online. HCPs may need to encourage and assist older adults in exploring their eligibility and submitting applications.13
Food budget strategies can be shared with individuals to help reduce the cost of nutritious foods. Individuals with limited access to large grocery stories or with limited food variety may benefit from taking multivitamin/mineral supplements. Education about how to take medications according to the timing of meals rather than the specific time of day may reduce hypoglycemia in food-insecure patients.
Food preparation challenges
Older adults may need adaptive cooking utensils and feeding devices to aid their self-sufficiency in food preparation. Older adults with dexterity or visual problems are at greater risk for kitchen injuries such as cuts and burns during cooking. Adaptive cooking utensils such as kitchen tools with built-up handles or supportive grips can aid patients with tremors, neuropathy, arthritis, or poor hand strength. Knife gloves and cutting boards with rubber grips may help to prevent injuries. Adaptive equipment for those with vision and hearing impairments is also available and can be located online, through catalogs, or with the help of a trained occupational therapist.
It may be helpful to recommend that older adults with dexterity impairments use convenience produce such as prepackaged cut lettuce, sliced carrots, and shredded cabbage to reduce the need for manual food preparation. Heavy use of convenience and frozen foods may be necessary to maintain a patient’s independence. These should be used with the recognition that many of these products have high amounts of sodium or contain less fiber than whole foods prepared at home. Clinicians should provide guidance about the best available options and allow the use of convenience foods if it is necessary to help patients maintain their independence.
Additional Nutrition Considerations
Hypoglycemia prevention
Physical activity. Physical activity can improve insulin sensitivity, aid in weight maintenance, and increase the lean body mass of older adults with diabetes, and all of these benefits can further the success of nutrition care. Older adults may also see improvements in their appetite, agility, and stability, as well as improved glucose control, from physical activity.
Patients should be educated about properly timing exercise in relation to meals, snacks, and medication schedules to prevent hypoglycemia. Sudden changes in mobility (e.g., from illness or injury) can also result in glycemic excursions. Encourage individuals to keep their health care team informed so they can make adjustments to medication and meal routines during significant changes in physical activity or other unusual circumstances.
Pattern management. Setting a frequency of self-monitoring of blood glucose (SMBG) in older adults should be done based on comparison of current readings to the target range and consideration of patients’ physical and mental capabilities, dietary habits, treatment plan, financial status, and risk for hypo- and hyperglycemia. Glucose meters with large display screens, large strips, and voice features are available to facilitate patients’ independence. Because glucose monitoring provides information essential to diabetes management, caregivers and family members may need to assist patients who cannot perform SMBG on their own.
Older adults who lack support or live alone should be routinely educated about the signs and symptoms of hypo- and hyperglycemia.25 Because elderly patients often are incapable of self-treating hypoglycemia,25,26 patients should be reminded regularly about how to access treatments or assistance if needed.
Pre- and postmeal tagging (i.e., adding pertinent comments to blood glucose records to explain the circumstances causing or actions taken in response to the measured values) can provide clinicians with valuable information about the food/carbohydrate impact on glycemic control.15 In the future, more widespread use of continuous glucose monitoring (CGM) systems in special populations such as older adults may provide clinicians with detailed information about patients’ glycemic responses to food when regular SMBG is not achieved. CGM may be especially useful for those with impaired cognition and physical abilities.
Meal timing. Skipped meals, irregular timing of meals, poor appetite, and inadequate intake are common causes of hypoglycemia in older adults. Hypoglycemia episodes can lead to falls or the need for emergency medical care and are feared by many older adults with diabetes. Skipped meals may be precipitated by financial barriers, cognitive changes, or social isolation. Older adults who live alone may have a lack of interest in cooking.
Senior group meals and meal delivery services may be helpful to help patients maintain interest in and regularity of meals. Timing medications to mealtimes rather than specific times of day and using medications with a shorter half-life can reduce the risks of glycemic excursions when food intake is irregular.27
General health and safety
Older adults are more vulnerable to viruses, which can also affect their food intake. Clinicians should counsel patients on appropriate sick-day management, including guidance on food intake to avoid hypoglycemia. Providing patients with a printed or pictorial list of foods to have on hand during illness, poor weather conditions, or other emergencies is another strategy to help patients maintain proper food intake and therefore glucose balance during these situations.
Diabetes self-management abilities
As noted above, a recent study suggested that the presence of diabetes itself or poor glycemic control may affect cognitive function in older adults.21 Daily self-management tasks, including routine meal planning, are demanding, and clinicians should not underestimate this burden on their older adult patients.
Clinicians may consider and be influenced by older patients’ degree of frailty, lifestyle, and life expectancy when developing their therapeutic approach,26 and liberalized diets may be considered in such patients, especially those for whom maintaining independence is a higher priority than diabetes management.28 However, it would be inappropriate to stereotype all older adults as being passive regarding their self-care or incapable of achieving good control.29 Instead, it may be the case that older adults face a greater self-care load than when they were younger, creating more challenges for daily decision making and execution of management tasks. Clinicians may need to modify their education and problem-solving approaches for older adults, recognizing potentially additional barriers to basic daily care and health management tasks.
Poor health literacy disproportionally affects older adults, resulting in increased mortality, poor health outcomes, and higher hospitalization rates.30 Educational strategies to overcome insufficient health literacy include limiting topics during instruction, keeping information relevant and practical, simplifying complex tasks, and using the teach-back method.29,30 Older adults may need additional instruction time when learning nutritional concepts such as carbohydrate counting, portion sizes, insulin-to-carbohydrate ratios, and label reading.
To help overcome learning barriers caused by vision, hearing, or dexterity impairments, educators should have a wide variety of nutrition educational materials available.4 Role playing, label reading, menu selection demonstrations, and menu writing can prove to be valuable activities during the nutrition education process.4,31 Culturally diverse and age-appropriate materials will also enhance the learning experience.29
Depression in older adults with diabetes
The relationship between depression and diabetes has been well documented, with estimates of depression occurring twice as frequently in those with diabetes.32 Depression is also more common in older than in younger adults.
Depression can lead to decreased independence, poor self-care, under- or overeating, and substance abuse.33 For these reasons, the risk for and possible presence of depression should be considered part of comprehensive nutrition assessments. Various depression assessment tools are available for use with older adults, including the Geriatric Depression Scale34 and the Patient Health Questionnaire 9.35 Additionally, clinicians should consider the potential effect of antidepressant therapies on patients’ appetite and nutrition.
Alcohol use
Alcohol abuse occurs in ∼ 15% of adults > 60 years of age, and the rate of alcohol abuse increases with age.36 The impact of alcohol use and abuse on nutrition should be considered a part of nutrition assessments.
Nutrition Care of Institutionalized Older Adults With Diabetes
The inability to perform adequate daily self-care or an acute or chronic medical condition could warrant admission to a care facility for short- or longer-term care. RDs in these facilities or in post-discharge medical services (e.g., home health services) should be engaged early in the admission process to help coordinate the nutrition care of patients with diabetes. New medications, restrictions on food intake (e.g., NPO status or liquid diets), or interventions should be balanced with a suitable nutrition care plan to avoid glycemic variances.
In the hospital setting, glycemic management is still the primary goal of the nutrition plan for patients with diabetes; additional goals include integrating the treatment of other medical conditions and providing adequate calories.36,37 There are varied approaches to meal delivery or menu composition for hospitalized patients, including generally recommended consistent-carbohydrate meal plans37 or, for patients with impaired nutritional status, possible oral supplemental nutrition or other specialized nutritional support. The type and amount of carbohydrate content, whether from a meal tray or from nutritional support, should be synchronized with diabetes medication delivery to avoid glucose fluctuations.17,38 Successful coordination of diabetes medications and nutritional support requires good communication between caregivers and support services.
The development of protocols and order sets may help with consistency of care delivery and hyperglycemia prevention. Hyperglycemia commonly occurs in hospitals as a result of medical conditions, but also because of changes in patients’ usual eating habits and food choices, bedside food gifts, modifications to medications (e.g., by mouth or intravenous delivery), lack of coordination in the timing of meals and medications, and use of nutrition supplementation or nutritional support therapy. Close monitoring of daily nutrition intake and a multidisciplinary team approach is beneficial.38
In comparison to hospitals, the focus shifts in long-term care facilities to prevention of hypoglycemia and malnutrition.39,40 A review of the literature on diabetes care in nursing homes reveals reports on many approaches to dietary management, including regular, nonrestricted diets; no-concentrated-sweets plans; and controlled dietary plans.37–40 Long-term care facilities may improve the care of frail older adults with diabetes by designing and implementing specific diabetes nutrition practice guidelines for different conditions (e.g., acute illness and enteral feeding).
Summary
Older adults can be successful with a therapeutic diabetes nutrition care plan despite the physiological and cognitive changes of aging and various lifestyle barriers. Efforts must be made to perform comprehensive nutrition assessments on older adults with diabetes to develop individualized and appropriate nutrition care plans based on patients’ individual circumstances and on the priorities and special needs of this population.6,31
Assessments should not be limited to biometric and medical parameters, but should also include many issues such as patients’ financial stability, social status, lifestyle, cognitive abilities, motivation, and ability to provide self-care. Extra time will need to be devoted to patient assessment visits to ensure that these issues are given adequate consideration. Referral to or consultation with an RD experienced in working with older adults with diabetes will aid in coordinating the important nutritional aspects of diabetes management for older adults in various environments and care settings. Additional sessions with the RD may be required to address ongoing educational needs and modify the nutrition care plan as needed to achieve established goals.
When patients’ nutritional needs are not being met, clinicians should consider strategies to resolve barriers to nutrition plan adherence, including medical factors contributing to poor appetite or intake, food insecurity issues, lack of support and social contact, and inability to prepare meals. When necessary, clinicians should also consider patients’ possible need for nutrition supplementation or a more liberalized meal plan. Diabetes management, including the nutrition care plan, should be individualized to address patients’ unique medical, cultural, financial, and social circumstances, regardless of their age. Clinicians may need to take a more active role in resolving barriers and facilitating solutions to improve self-care in older adults because of the characteristics of and common problems facing these patients.
Older adults may have rapidly changing circumstances (e.g., changes in mobility, financial situation, or health status or the loss of a spouse). Therefore, clinicians should reevaluatetheir self-care through regular follow-up contact. Because nutrition self-management is a daily expectation and is crucial to overall blood glucose control, this area in particular will require periodic reassessment and adjustment.
Although the older adult population has a higher percentage of diabetes than any other age-group, there is little published nutrition-related research involving older adults with diabetes. Additional research is needed to provide HCPs with evidence-based recommendations regarding nutrition care, medication management, and other aspects of diabetes care for this growing patient population. The 2012 American Diabetes Association consensus report on older adults with diabetes has helped to focus attention on this special population.6 As new recommendations emerge, clinicians are encouraged to maintain a realistic perspective when developing diabetes care plans for older adults. Optimal nutrition care plans, as well as overall diabetes management plans, should delineate attainable goals that will result in desirable medical outcomes without negatively affecting patients’ quality of life or hindering their established lifestyle.
References
- 1.Soriano R: Fundamentals of Geriatric Medicine. New York, Springer, 2007 [Google Scholar]
- 2.Garnder DG, Shoback D: Greenspan’s Basic and Clinical Endocrinology. 8th ed. New York, McGraw Hill, 2007 [Google Scholar]
- 3.Shepherd RJ, Aoyagi Y: Objective monitoring of physical activity in older adults: clinical and practical implications. Phys Ther Rev 15:170–182, 2010 [Google Scholar]
- 4.Mooradian AD, McLaughlin S, Boyer CC, Winter J: Diabetes care for older adults. Diabetes Spectrum 12:70–77, 1999 [Google Scholar]
- 5.American Diabetes Association : Screening for type 2 diabetes. Diabetes Care 27 (Suppl.1):S11–S14, 2004 [DOI] [PubMed] [Google Scholar]
- 6.American Diabetes Association : Consensus report: diabetes in older adults. Diabetes Care 35:2650–2664, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sarienchi T, Iso H, Fujiko I, Fukasawa N, Ota H, Muto T: Underweight as a predicator of diabetes in older adults. Diabetes Care 31:583–584, 2008 [DOI] [PubMed] [Google Scholar]
- 8.Odegard PS, Setter SM, Neumiller JJ: Considerations for the pharmaceutical treatment of diabetes in older adults. Diabetes Spectrum 20:239–247, 2007 [Google Scholar]
- 9.American Diabetes Association : Standards of medical care in diabetes – 2011. Diabetes Care 24 (Suppl. 1):S11–S61, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lee SJ, Eng C: Goals of glycemic control in frail older patients with diabetes. JAMA 305:1350–1351, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Schwartz AV, Vittinghoff E, Sellmeyer DE, Feingold KR, de Rekeneire N, Strotmeyer ES, Shorr RI, Vinik AI, Odden MC, Park SW, Faulkner KA, Harris TB; Health, Aging, and Body Composition Study Group: Diabetes-related complications, glycemic control, and falls in older adults. Diabetes Care 31:391–396, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.U.S. Department of Agriculture and U. S Department of Health and Human Services: Dietary Guidelines for Americans, 2010. 7th ed. Washington, D.C, U.S. Government Printing Office, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Institute of Medicine : Dietary Reference Intakes (DRIs): estimated average requirements. Available from http://iom.edu/Activities/Nutrition/SummaryDRIs/∼/media/Files/Activity%20Files/Nutrition/DRIs/New%20Material/5DRI%20Values%20SummaryTables%2014.pdf. Accessed 30 October 2012
- 14.Academy of Nutrition and Dietetics : Food and nutrition for older adults: promoting health and wellness. J Acad Nutr Diet 112:1255–1277, 2012 [DOI] [PubMed] [Google Scholar]
- 15.Suhl E, Bunsignore P: Diabetes self-management education for older adults: general principles and practical application. Diabetes Spectrum 19:234–240, 2006 [Google Scholar]
- 16.Terrio L: Self-sufficient diabetes management: maintaining independence in older adults. On the Cutting Edge 30:14–19, 2009 [Google Scholar]
- 17.Johnson MA, Park S, Penn D, McClellan JW, Brown K, Alder A: Nutrition issues for older adults. Available from http://ncsu.edu/ffci/publications/2008/v13-n3-2008-winter/johnson-park-penn-mcclelland-brown-adler.php. Accessed 1 July 2012
- 18.U.S. Department of Health and Human Services Administration on Aging : A profile of older Americans: 2011. Available from www.aoa.gov/AoAroot/Aging_Statistics/Profile/2011/docs/2011profile.pdf. Accessed 11 November 2013
- 19.American Association of Diabetes Educators : Special considerations in the management and education of older persons with diabetes. Diabetes Educ 35 (Suppl. 3):60S–63S, 2009 [Google Scholar]
- 20.Stanley K: Assessing the nutritional needs of the geriatric patient with diabetes. Diabetes Educ 24:29–37, 1998 [DOI] [PubMed] [Google Scholar]
- 21.Yaffe K, Falvey C, Hamilton N, Schwartz AV, Simonsick EM, Satterfield S, Cauley JA, Posano C, Launer LJ, Strotmeyer ES, Harris TB: Diabetes, glucose control and 9-year cognitive decline among older adults without dementia. Arch Neurol 69:1170–1175, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Niedert KC, Dorner B: Nutrition Care of the Older Adult. 2nd ed. Chicago, American Dietetic Association, 2004 [Google Scholar]
- 23.Sutin DG: Diabetes mellitus in older adults: time for an overtreatment quality indication. J Am Geriatr Soc 58:2244–2245, 2010 [DOI] [PubMed] [Google Scholar]
- 24.USDA Food Safety and Inspection Service homepage http://www.fsis.usda.gov/wps/portal/fsis/topics. Accessed 23 September 2013.
- 25.Lopez A, Seligman HK: Clinical management of food insecure individuals with diabetes. Diabetes Spectrum 25:14–18, 2012 [Google Scholar]
- 26.Sinclair AJ: Special considerations in older adults with diabetes: meeting the challenge. Diabetes Spectrum 19:229–233, 2006 [Google Scholar]
- 27.McCulloch DK, Munshi M: Treatment of type 2 diabetes in the elderly patient [article online]. Available from http://www.uptodate.com/contents/treatment-of-type-2-diabetes-mellitus-in-the-elderly-patient. Accessed 23 May 2012
- 28.Mooradian AD, Chehade JM: Diabetes mellitus in older adults. Am J Ther 19:145–159, 2012 [DOI] [PubMed] [Google Scholar]
- 29.Falvo D: Barriers to effective patient teaching with older adults. In Effective Patient Education. 4th ed. Jones and Barlett Publishers, 2011, p. 297–323. Also available from http://www.R2library.com/marc_frame.aspx?ResourceID=2361. Accessed 5 July 2012 [Google Scholar]
- 30.Speros CI: More than words: promoting health literacy in older adults. Online J Nurs 14:manuscript 5, 2009 [Google Scholar]
- 31.Stanley K: Nutrition therapy for older adults with diabetes. In American Diabetes Association Guide to Nutrition Therapy for Diabetes. 2nd ed. Franz MJ, Evert AB, Eds. Alexandria, Va., American Diabetes Association, 2012, p 169–180 [Google Scholar]
- 32.Anderson RJ, Freedland KE, Clouse RE, Lustman PJ: The prevalence of comorbid depression in adults with diabetes. Diabetes Care 24:1069–1078, 2001 [DOI] [PubMed] [Google Scholar]
- 33.Trief PM: Depression in elderly diabetes patients. Diabetes Spectrum 20:71–75, 2007 [Google Scholar]
- 34.Sheikh JL, Yesavage JA: Geriatric Depression Scale: recent evidence and development of a shorter version. Clin Gerontol 5:165–173, 1986 [Google Scholar]
- 35.Kroenke K, Spitzer RL: The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann 32:1–7, 2002 [Google Scholar]
- 36.Blow FC, Barry KL: Use and misuse of alcohol among older women, 2003. Available at http://pubs.niaaa.nih.gov/publications/arh26-4/308-315.htm. Accessed 11 November 2013 [PMC free article] [PubMed]
- 37.Swift CS: Nutrition therapy for the hospitalized and long-term care patient with diabetes. In American Diabetes Association Guide to Nutrition Therapy for Diabetes. 2nd ed. Franz MJ, Evert AB, Eds. Alexandria, Va, American Diabetes Association, 2012, p. 229–245 [Google Scholar]
- 38.American Diabetes Association : Translation of the diabetes nutrition recommendations for health care institutions. Diabetes Care 26 (Suppl. 1):S70–S72, 2003 [DOI] [PubMed] [Google Scholar]
- 39.Garcia TJ, Brown SA: Diabetes management in the nursing home: a systematic review of the literature. Diabetes Educ 37:167–187, 2011 [DOI] [PubMed] [Google Scholar]
- 40.American Association of Clinical Endocrinologists and American Diabetes Association : American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care 32:1119–1131, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]