

In Brief
Older adults with type 1 diabetes are at high risk for severe hypoglycemia and may have serious comorbid conditions. Problems with cognition, mobility, dexterity, vision, hearing, depression, and chronic pain interfere with the ability to follow complex insulin regimens. With the development of geriatric syndromes, unpredictable eating, and frailty, treatment regimens must be modified with the goal of minimizing hypoglycemia and severe hyperglycemia and maximizing quality of life.
The incidence and prevalence of diabetes are increasing, with rapid growth in the aging population. Although the majority of this phenomenon is the result of the epidemic of type 2 diabetes, epidemiological data suggest that the incidence of type 1 diabetes is increasing by 2–5% per year worldwide.1–3 As a result of improved diabetes management, an increased proportion of individuals with type 1 diabetes are living into the later decades of life.4
Diabetes care plans for older adults must consider aging-related changes that can affect their functional status and ability to self-manage their disease. Advances in the management of type 1 diabetes after the Diabetes Control and Complications Trial5–7 led to routine use of complex insulin regimens, which may become difficult to follow for older adults. Treatment regimens must be modified to adapt to the changes commonly observed with aging. Addressing the unique issues associated with aging can significantly improve the quality of life of older adults and help avoid unnecessary health care costs.8,9
Type 1 diabetes is commonly diagnosed in childhood, but ∼ 25% of people with type 1 diabetes are diagnosed as adults, some even as late as the ninth decade of life.10 About 10% of adults initially diagnosed with type 2 diabetes are found to have pancreatic autoantibodies associated with type 1 diabetes.11 The clinical characteristics of youth-onset type 1 diabetes and type 1 diabetes with onset in adulthood can differ, with potential consequences concerning management later in life.12 Individuals with detectable C-peptide levels, which are more common early in the course of the disease and with onset of type 1 diabetes in adulthood, have better clinical outcomes and can achieve lower A1C levels with less serious hypoglycemia than those without detectable C-peptide concentrations.13,14 An earlier onset of type 1 diabetes is also associated with a longer burden of disease and more diabetes-related complications in the aging population. Lower quality of life in adults with type 1 diabetes is related to worse glycemic control, the presence of chronic complications such as renal disease, and a history of severe hypoglycemia.15,16 All of these factors are important to consider in individualizing management plans for older adults with type 1 diabetes.
Challenges in the Management of Type 1 Diabetes in Older Adults
There is a paucity of data related to glycemic management and control of type 1 diabetes later in life. The Type 1 Diabetes (T1D) Exchange clinic registry reported characteristics of older adults with type 1 diabetes who are followed in diabetes centers across the United States.17 Of those ages 50 to < 65 years (n = 2,066), mean A1C was 7.7% (27% had an A1C < 7.0%, 46% had an A1C < 7.5%, and 11% had an A1C ≥ 9.0%), and mean self-reported blood glucose testing was 5.5 times daily. Of those ≥ 65 years of age (n = 683), mean A1C was 7.4% (34% had an A1C < 7.0%, 52% had an A1C < 7.5%, and 8% had an A1C ≥ 9.0%) and mean self-reported blood glucose testing was 5.6 times daily. Greater frequency of self-monitoring of blood glucose (SMBG) was associated with lower A1C levels in both those who used an insulin pump and those who administered insulin via injections.18 Diabetic ketoacidosis (DKA) was lower with increasing age and was not associated with duration of diabetes.19 DKA was more likely in those with higher A1C levels and lower socioeconomic status. No relationship was found between DKA and pump versus injection use.
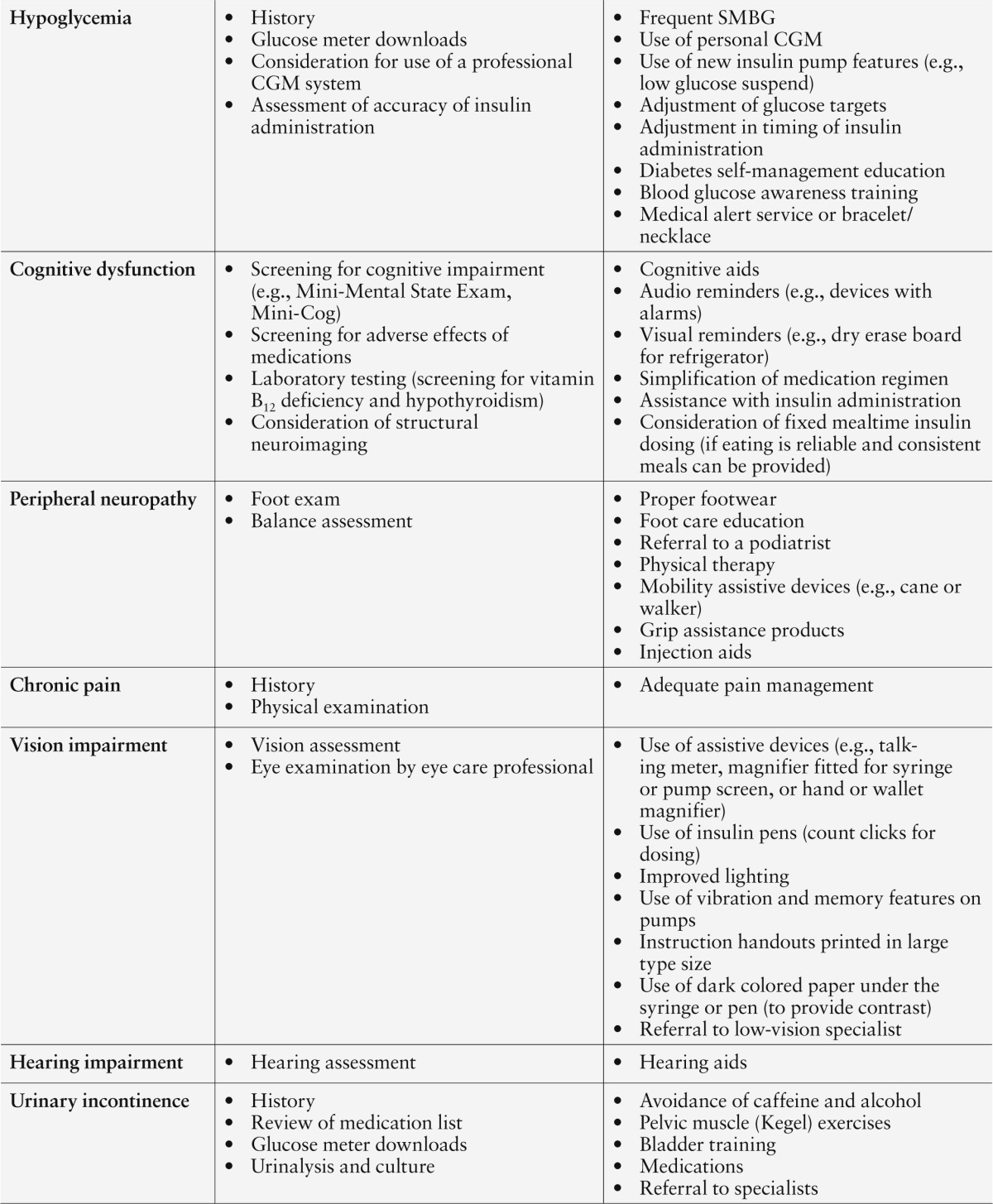
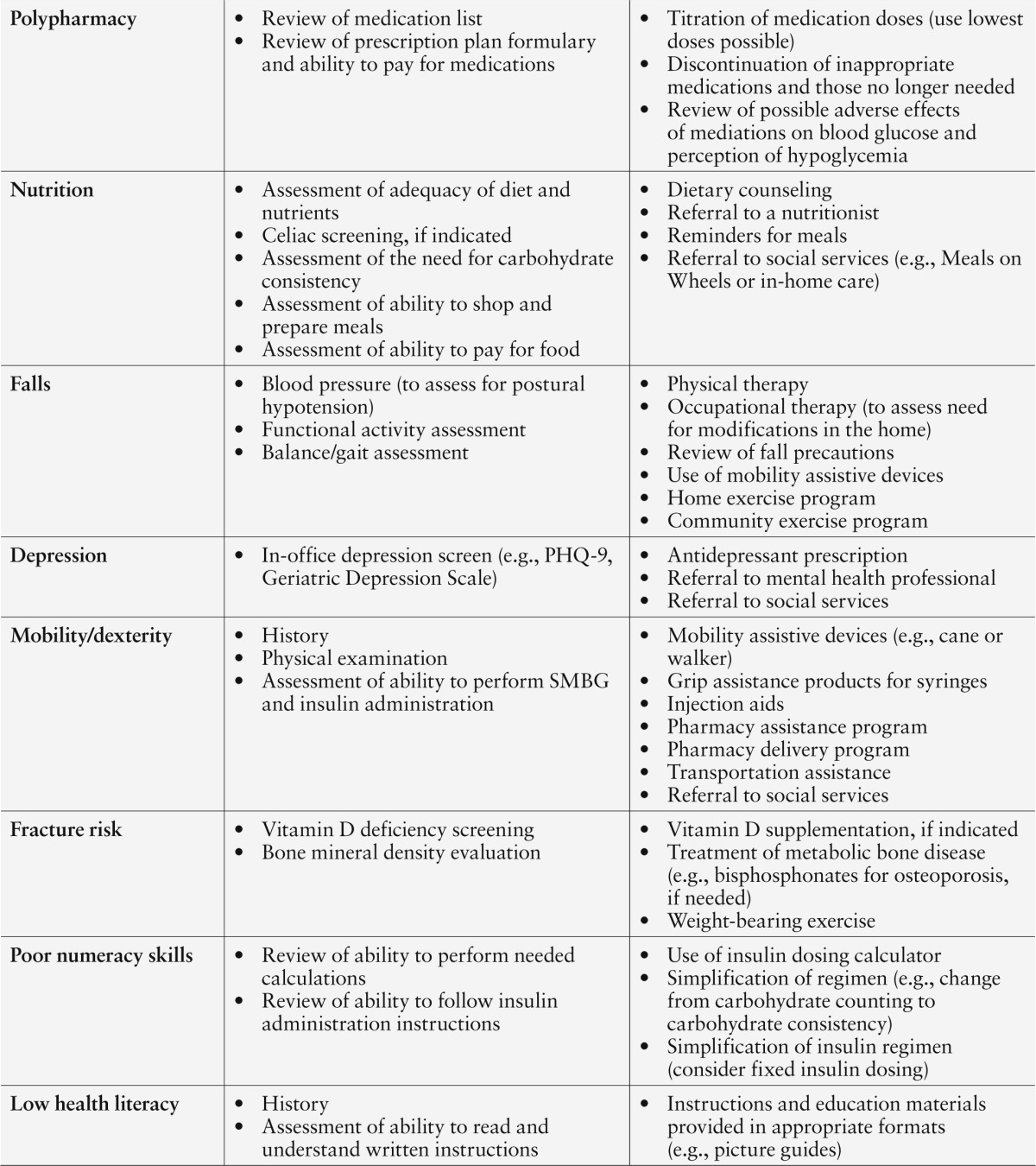
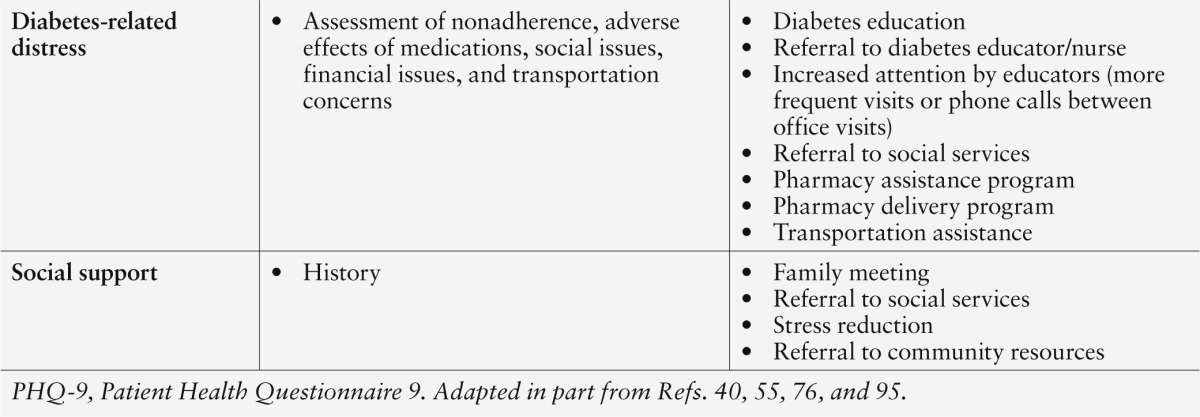
Longstanding diabetes in older adults has been associated with increased risks of severe hypoglycemia, micro- and macrovascular complications, cognitive decline, and physical disabilities. Older adults may also have other medical comorbidities, functional disabilities, erratic food intake, and insufficient social support. Individuals with geriatric syndromes (i.e., chronic pain, urinary incontinence, polypharmacy, cognitive impairment, frequent falls, and depression)20–23 face additional difficulties in performing self-management tasks and lower quality of life. Clinical, functional, and psychosocial factors that should be identified and addressed when developing treatment plans are listed in Table 1 and discussed below. The goal is to minimize hypoglycemia and severe hyperglycemia to preserve quality of life.
Table 1.
Challenges in Older Adults With Type 1 Diabetes
Hypoglycemia risk
Hypoglycemia is a major barrier to achieving optimal glycemic control. It is common in type 1 diabetes and is associated with increased morbidity and mortality and reduced quality of life.19,24–28 Severe hypoglycemia, defined as an episode requiring external assistance for treatment, is of greatest concern because it has been associated with cardiac abnormalities including arrhythmias29 and brain damage.30,31 Hypoglycemia unawareness and poor awareness are major risk factors for severe and recurrent hypoglycemia in type 1 diabetes32 and are of particular concern in the elderly because of their increased risk of falls, cognitive impairments, and cardiovascular disease. With aging and long duration of diabetes, there is impairment of counterregulatory responses to hypoglycemia.33–36 The glycemic threshold at which autonomic symptoms occur and reaction time are also modified by advancing age.33 Confusion, dizziness, falling, weakness, difficulty with communication, and poor coordination and balance may not be recognized as possible symptoms of hypoglycemia.
In the T1D Exchange, 18.6% of participants with diabetes ≥ 40 years of age (n = 758) self-reported having had a seizure or loss of consciousness in the previous 12 months.19 Duration of diabetes was associated with the occurrence of severe hypoglycemia. Severe hypoglycemia was also associated with lower education status and household income, lack of private insurance, and race (greater in non-Hispanic blacks and Hispanics than in non-Hispanic whites). Injection users had more severe hypoglycemia than insulin pump users. Self-reported severe hypoglycemia was lowest in those with mean A1C levels of 7.0–7.5%. In the U.K. Hypoglycaemia Study, there was a 46% prevalence over 12 months of severe hypoglycemia in adults with type 1 diabetes of > 15 years’ duration (mean age 53 years, A1C 7.8%).37 Severe hypoglycemia in type 1 diabetes is more common in the presence of nephropathy, neuropathy, and depression and with the use of nonselective β-blockers and alcohol.27,38 Insulin dosing needs to be reduced with advancing renal insufficiency. Fear of hypoglycemia is another obstacle to optimizing glycemic control in older adults.39
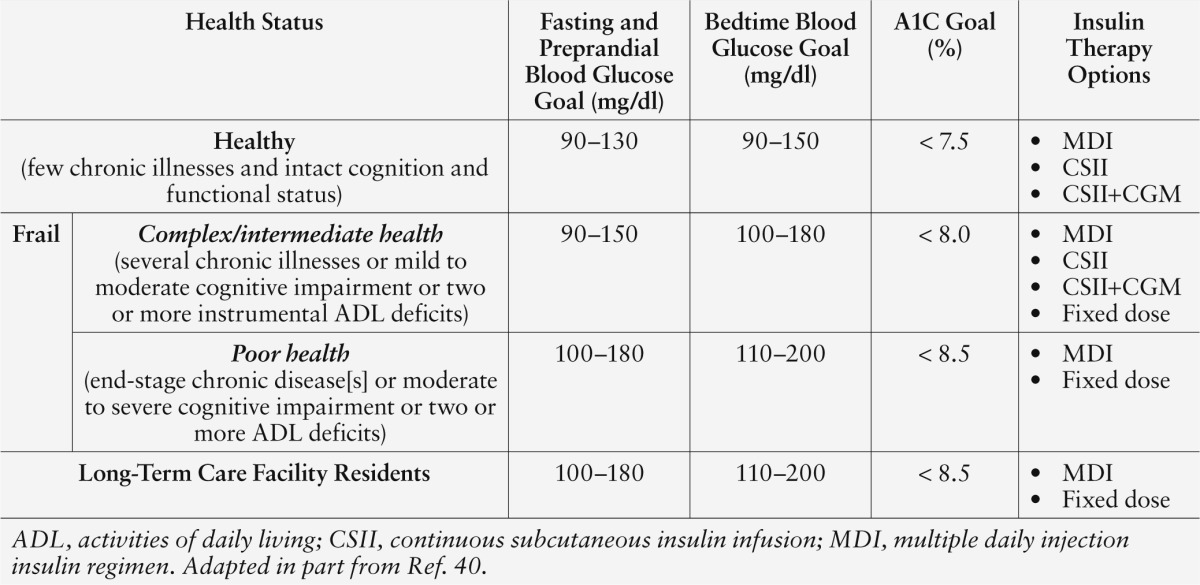
The association of increased incidence of severe hypoglycemia with intensive glycemic control in older adults19,40–43 has generated controversy regarding glycemic targets in this population.19,40–48 Higher A1C goals are recommended for older adults with multiple comorbidities, disabilities, or a history of recurrent hypoglycemia (Table 2). These flexible targets, however, may not be sufficient to significantly reduce hypoglycemia, as observed in a recent study of adults ≥ 69 years of age with an A1C > 8%.45 During 72 hours of continuous glucose monitoring (CGM), 65% experienced hypoglycemia at least once. In the T1D Exchange, high rates of severe hypoglycemia were reported in adults with an A1C > 7.5% and > 40 years’ duration of diabetes.19 Technological advances leading to closed-loop insulin delivery systems will be needed to fully address this problem.
Table 2.
Glycemic Management of Type 1 Diabetes in Older Adults
Chronic pain
Chronic pain can lead to difficulty with self-care in older adults and can contribute to glycemic variability. Pain medications can also cause confusion and reduce coordination. Additionally, chronic pain is associated with higher health care costs in older adults because of increased falls and fractures, slow rehabilitation, depression, and decreased socialization.8 It is important to assess pain in older patients at every medical visit and provide adequate treatment.
Vision and hearing impairment
Visual and auditory impairments affect the ability to perform self-care tasks and are related to aging, as well as vascular and neurological damage from diabetes.49–51 Acute reversible changes in vision can result from serious hypoglycemia (e.g., central scotoma and reduced contrast sensitivity52) and hyperglycemia (e.g., blurry vision). Poor vision may be a barrier to accurate insulin administration, increasing the risk of hypoglycemia and falls. Hearing loss may contribute to a patient’s inability to fully understand instructions from providers. Hearing and vision impairment can also limit social interaction and independence and have untoward psychosocial effects (e.g., isolation, fatigue, avoidance, depression, and negativism). Such impairments should be identified and addressed during diabetes education and training, and management plans should be modified as needed. Magnifiers, “talking” glucose meters, insulin pens, and written instructions provided in large type sizes can be helpful.
Comorbid medical conditions
Older adults with multiple comorbidities, including geriatric syndromes, may experience a failure-to-thrive pattern of decline. Coexisting chronic medical conditions such as hypertension, chronic kidney disease, heart failure, chronic lung disease, musculoskeletal conditions, cancer, and history of stroke require particular attention. These comorbidities can have profound impacts on functional status and quality of life20,21 and affect insulin requirements and self-care abilities. Older adults with type 1 diabetes may require frequent adjustments in insulin dosing, especially during acute illnesses, to decrease the likelihood of dehydration, DKA, hypoglycemia, and poor wound healing.
Urinary incontinence
Incontinence is common in older women with type 1 diabetes and has a greater prevalence than neuropathy, retinopathy, and nephropathy.53 Women with diabetes are more likely than those without it to experience severe, symptomatic incontinence and urinary tract infections.54 Urinary incontinence can inhibit socialization, interfere with daily activities, and contribute to increased falls, depression, and lower quality of life. Because hyperglycemia worsens incontinence, bladder infections, and vaginal candidiasis, achieving satisfactory glycemic control to avoid glucose-induced polyuria and nocturia is recommended.
Polypharmacy issues
Polypharmacy, which is common in diabetes, predisposes older adults to drug-to-drug interactions and adverse drug effects caused by altered drug disposition from age-related changes in drug metabolism.40,50 Seniors are more sensitive to many medications, may require lower doses, and may be more prone to side effects affecting brain function, physical functioning, balance, and food intake. Careful selection of medications that have a strong benefit-to-risk ratio, prescription of the lowest doses possible, consideration of renal function, and discontinuation of medications that are no longer needed or are causing undue adverse events are all important.55 Patients and their caretakers should be educated to recognize, respond to, and report possible side effects.
Nutrition concerns
Medical nutrition therapy is an essential component of diabetes care. Mealtime insulin dosing is designed primarily to match the carbohydrate content of meals, but inconsistent food intake is common in older adults, and numeracy skills are often lacking. This can be responsible for wide glycemic fluctuations. Older adults with diabetes can also develop micronutrient deficiencies from declining caloric intake with aging. Tooth loss and dental disease, inability to shop for groceries or prepare or consume meals, depression, swallowing difficulties, and polypharmacy can lead to undernutrition. Weight loss, whether intentional or unintentional, may contribute to nutritional deficits, worsen sarcopenia, and reduce bone health.56–58
Dietary counseling is recommended. Fortified foods and nutritional supplements can be used. Older adults may find community resources such as Meals on Wheels or meals served at local senior centers beneficial. In the presence of poor and unpredictable food intake, consideration should be given to administering rapid-acting insulin immediately after meals instead of before so lower doses can be given if less food is consumed.
Cognitive impairment
Unlike other chronic conditions, diabetes management involves performing multiple complex self-care tasks, including frequent SMBG and appropriate adjustment and self-administration of insulin multiple times daily. Cognitive dysfunction, which can vary in magnitude from subtle deficits to overt dementia, affects the ability of older adults with type 1 diabetes to self-manage their disease.59
Although vascular disease in type 1 diabetes has been associated with brain damage, glycemic control also appears to play a role in cognitive performance.31 Hyperglycemia has been linked with an increased number of mental subtraction errors, decreased attention, impaired speed of information processing, impaired working memory, and loss of inhibition and focus.60–62 Hypoglycemia affects immediate memory, working memory, visual-motor skills, visual-spatial skills, and global cognitive function.62,63 Studies have reported decline in cognitive function with repeated episodes of hypoglycemia.31
When impaired cognition becomes evident, screening for alcohol use, thyroid dysfunction, and vitamin B12 deficiency should be considered. Older adults may not display typical signs and symptoms of hypothyroidism, and there is an increased risk of autoimmune thyroid disease in type 1 diabetes. Recognition of cognitive deficits, assistance from family members or caretakers, simplification of treatment regimens, and use of cognitive aids can all be helpful for older patients with type 1 diabetes.
Physical disability
Physical disabilities are common in older adults with diabetes and predict future decline in health status and reduction in quality of life.64,65 More than half of older individuals with diabetes have peripheral neuropathy,66 which, along with comorbid conditions such as arthritis and vascular disease, increases the risk of functional impairment from muscle atrophy, balance and gait problems, postural instability, and falls. These conditions can interfere with the ability to keep medical appointments and perform activities of daily living.
Physical inactivity
Physical activity is an important component of diabetes care. Even light-intensity physical activity has been associated with self-reported improvements in physical health and psychosocial well-being.67 Physical therapy can improve the balance and overall functional status of older adults. Supervised home- and community-based exercise programs should be encouraged. To avoid hypoglycemia during or after increased physical activity, insulin dosing at the previous meal should be reduced or omitted or a carbohydrate snack should be given just before exercise. Basal insulin dosing may need to be lowered with regular daily physical activity.
Falls and fractures
Fall risk should be assessed periodically in older adults.68 Neuropathy, vision loss, sarcopenia, and gait and balance problems are all risk factors for falls and subsequent fractures.69,70 Older women with diabetes are at high risk for hip and proximal humeral fractures, which are associated with substantial mortality and morbidity.71
Fall prevention should be reviewed with all older adults with type 1 diabetes.68 Physical therapy and balance improvement exercises should be encouraged, and mobility aids should be used when needed. Daily calcium intake (diet plus supplements) should be 1,000–1,200 mg, and vitamin D intake should be 800–1,000 IU.72 Additional vitamin D supplements may be needed when deficiency is documented. The National Osteoporosis Foundation recommends bone mineral density studies to evaluate for osteoporosis in women > 65 years of age or postmenopausal with risk factors, in men > 70 years of age or 50–69 years of age with risk factors, and in the presence of compression fracture.72
Depression risk
Adults with diabetes have a high prevalence of depression.73 In the T1D Exchange, depressive symptoms (Patient Health Questionnaire-8 scores ≥ 10) were reported in 12% of those 50 to < 65 years of age (n = 1,032) and 6.2% of those ≥ 65 years of age (n = 406), with no difference between insulin injection and pump users.38 Those with depression had more severe hypoglycemia, higher A1C levels, more self-reported missed insulin doses, and more DKA.38
Untreated depression not only negatively affects self-care, medication adherence, and lifestyle choices, but also can be responsible for anorexia, nausea, constipation, and loss of appetite.38,74 It may also result in disinterest or inability to prepare meals. Alterations in food intake can contribute to fluctuations in glucose levels and increase the risk of hypo- and hyperglycemia. Depression screening at regular intervals can help identify older adults who may benefit from antidepression treatment.
Diabetes-related distress
In older adults with a long duration of type 1 diabetes, acute and chronic complications, as well as other causes of stress, are common. Effective coping and social support can help improve adherence, glycemic control, and quality of life.75 Interventions, including diabetes-related education, frequent contact with the diabetes care team, pharmacy delivery programs, transportation assistance, and other social services can help reduce diabetes-related distress.76
Guidelines for Managing Type 1 Diabetes in Older Adults
There has been little research examining the best treatment approaches for older adults with type 1 diabetes. The American Diabetes Association (ADA) and the American Geriatrics Society (AGS) recommend a collaborative and integrated team approach to treating older patients with diabetes, using a variety of strategies to assess and address age-specific barriers and provide individualized treatment plans and education to patients and their partners or caretakers.40 Treatment aims include establishing acceptable glycemic control and minimizing the risk for acute complications (i.e., hypoglycemia and serious hyperglycemia).40 These guidelines are primarily directed toward older people with type 2 diabetes. In the absence of guidelines specifically for older individuals with type 1 diabetes, these general principles are used. A framework is provided for consideration of glycemic goals (Table 2) and treatment goals for blood pressure and dyslipidemia (Table 3) in older adults based on health status and comorbidities.
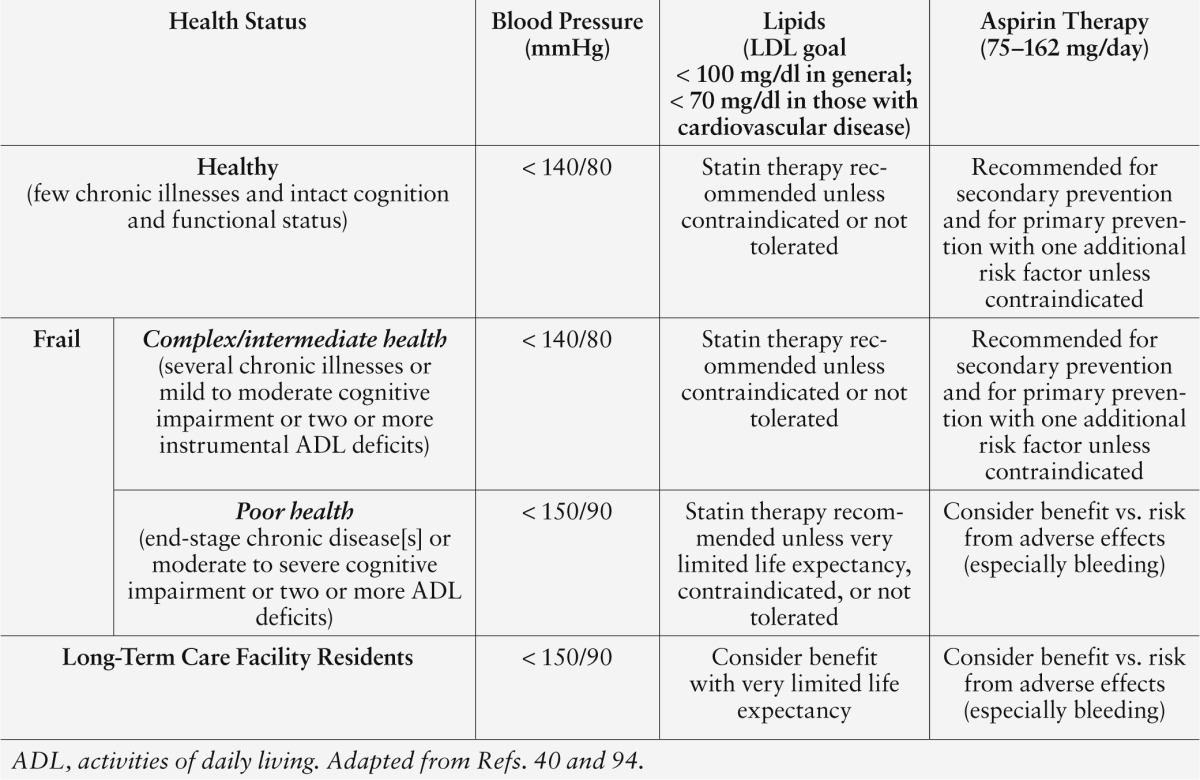
Table 3.
Management of Cardiovascular Risk Factors in Older Adults With Type 1 Diabetes
Healthy, independently functioning older adults should be treated more aggressively than those who are frail or who have multiple comorbid conditions and disabilities associated with a limited life expectancy. For healthy older individuals with few coexisting chronic illnesses who are able to self-manage their diabetes, an A1C goal of < 7.5% is recommended.
Frailty is defined as the presence of three of five of the following: low grip strength, low energy, slowed walking speed, low physical activity, and unintentional weight loss.77 Frail older adults have reduced life expectancy and increased risk of hypoglycemia and are either unable to perform or have difficulty performing self-care tasks. The goal A1C for frail older adults with poor health status due to end-stage chronic disease or high levels of physical and cognitive disability who are living at home is < 8.5%. Lower goals can be considered in the absence of hypoglycemia and if they can be achieved without undue burden.
Older adults with complex or intermediate health status have multiple chronic illnesses; have mild to moderate cognitive impairment or dependency in more than two instrumental activities of daily living; and are susceptible to hypoglycemia. Complex insulin regimens may become difficult for them to follow. An individualized approach to managing type 1 diabetes becomes crucial in this population, with consideration of an A1C goal of < 8.0% (Table 2).40
Frequent SMBG is important to guide insulin therapy and detect and avoid hypoglycemia. Insulin regimens should be simplified according to patients’ preferences. The need for diabetes education should be periodically assessed. Family members and caretakers should participate in education, training, and follow-up. They should be reminded that basal insulin should not be discontinued during inter-current illness or during periods of poor oral intake because this could lead to DKA. With serious hyperglycemia, attention is needed in monitoring hydration and electrolyte status, and abnormalities should be carefully treated. Physical activity should be encouraged to help maintain functionality, and regular screening for barriers to adequate management of type 1 diabetes should be followed with appropriate intervention.
Continued surveillance of diabetes-related disabilities should be a priority, along with interventions to reduce disability. Periodic comprehensive geriatric assessments should be carried out to identify functional and cognitive decline, as well as psychosocial concerns. Frequent communication with the diabetes care team and use of community resources can be helpful.76
Insulin therapy
Insulin therapy is required in type 1 diabetes to prevent serious hyperglycemia and DKA. Insulin treatment strategies and delivery approaches must be individualized and will differ between healthy older adults and those with frailty and limited life expectancy.
Multiple daily injection (MDI) insulin regimen. This regimen combines basal insulin coverage 24 hours/day and bolus insulin with meals. The basal insulin is commonly once-daily insulin glargine or once- or twice-daily insulin detemir. Insulin detemir, particularly in low doses, may not be effective for 24 hours and may need to be given twice daily. Insulin detemir may be associated with less hypoglycemia than insulin glargine.78–80 Rapid-acting insulin is usually given before or with meals and snacks. To achieve good glycemic control, prandial insulin dosing should take into account the premeal blood glucose level and anticipated carbohydrate intake and activity. If food intake is uncertain, rapid-acting prandial insulin can be given immediately after the meal so the dose can be adjusted based on actual intake.
Many healthy adults use insulin-to-carbohydrate ratios and correction factors to calculate their mealtime doses. This approach becomes more difficult with aging and the development of geriatric syndromes. Older individuals with these syndromes may require the assistance of their partner or caretaker. An alternative approach relies on fixed meal dosing and an eating plan that provides consistent carbohydrates at each meal and consistent timing of meals. To avoid hypoglycemia, correction dosing should be prescribed with great caution in the presence of frailty and used only to correct for serious hyperglycemia. Frail individuals also have a high risk of acute illness and hospitalization and may require frequent insulin dose adjustments with changes in their overall health status. Periodically, a diabetes educator should evaluate the ability of older individuals or their caretaker to perform the necessary tasks to properly administer insulin.
Some older patients use NPH insulin twice daily and regular insulin before breakfast and dinner (and at lunch if the morning NPH effect is insufficient to cover lunch) because the cost of these insulin formulations is less than that of insulin analogs. Because of the increased risk for hypoglycemia with these insulin preparations, snacks may be needed mid-morning, mid-afternoon, and at bedtime to avoid hypoglycemia. Glucose levels should be checked in the middle of the night to rule out nocturnal hypoglycemia. Administering NPH insulin at bedtime (instead of before dinner) can be helpful in reducing nighttime hypoglycemia.
Continuous subcutaneous insulin infusion (CSII). Insulin pump therapy is commonly used in adults with type 1 diabetes and has been associated with less hypoglycemia and better quality of life than MDI regimens.81 There are few data concerning the use of CSII in older adults. With aging, the use of CSII may become difficult. Pump therapy can be continued as long as individuals are capable of properly using a pump or their partner or caretaker is capable and willing to take over this responsibility. Pump therapy has the advantage of being able to provide more than one basal rate, permit the use of reduced temporary basal rate for increased activity, provide an insulin bolus calculator (incorporated in the pump to calculate bolus dosing based on glucose level, carbohydrate intake, and sensitivity factor), and permit the use of extended or dual boluses for patients with gastroparesis. The memory and vibration features may be helpful in the elderly population. As with MDI regimens, postmeal administration of prandial insulin via the insulin pump may be advisable to avoid hypoglycemia in individuals with unpredictable food intake.
Insulin pump therapy (CSII) with CGM. The use of CGM-augmented pump therapy has not been well studied in older adults. In adults > 25 years of age, frequent use of CGM was associated with lower A1C levels and fewer episodes of hypoglycemia.24 The ASPIRE (Automation to Simulate Pancreatic Insulin REsponse) study examined the use of CGM-augmented pumps with a low glucose threshold suspend feature in patients with type 1 diabetes ages 16–70 years. Hypoglycemia was reduced without deterioration in A1C levels.82 This technology holds promise for improving quality of life by decreasing hypoglycemia.
Premixed insulins. Premixed insulins are rarely used in type 1 diabetes because of their nonphysiological profiles. In specific circumstances when other regimens are not possible, twice-daily dosing (before breakfast and dinner) can be considered. Snacks may be needed mid-morning, mid-afternoon, and at bedtime to avoid hypoglycemia. Glucose levels should be checked in the middle of the night to rule out hypoglycemia.
Residents of long-term care facilities
Diabetes is a well-recognized risk factor for admission to long-term care (LTC) facilities.83 Adults in LTC have increased hospitalization rates, susceptibility to infections, macrovascular complications, depression, physical disabilities, and cognitive decline compared to ambulatory adults without diabetes.84,85 Management of type 1 diabetes in LTC residents is challenging because of variable nutritional status, erratic meal consumption and fluid intake, difficulties with communication related to cognitive dysfunction, and inadequate training of staff in the monitoring and treatment of type 1 diabetes. All of these factors make this population particularly vulnerable to wide glycemic excursions, with unrecognized hypo- and hyperglycemia.
MDI therapy with flexible blood glucose targets is generally used in LTC facilities (Table 2). Meals of fixed composition should be given with consideration to the residents’ food preferences to avoid unintentional weight loss and malnutrition. Administration of fixed prandial insulin doses (immediately postmeal if intake is uncertain) is desirable to enhance patient safety. Older adults with type 1 diabetes who are unable to ingest meals require basal insulin to avoid DKA. Premixed insulins should be used rarely because of the high risk of hypoglycemia given the variable dietary habits and poor ability to recognize and communicate about hypoglycemia in this vulnerable population. More frequent blood glucose monitoring is indicated during acute illnesses, when food intake is changing, and when adjusting insulin doses for hyper- or hypoglycemia.
Most older adults in LTC facilities are dependent on facility staff to perform self-care tasks. The staff should have diabetes education and training, understand the importance of glucose monitoring in type 1 diabetes, and be alert for possible hypoglycemia and serious hyperglycemia. Glucose monitoring results should be regularly reviewed, with modification of insulin dosing and diet as needed when hypoglycemia or severe hyperglycemia is detected. Results from a pilot study suggest that telemedicine consultations may be of benefit in reducing hypoglycemia and severe hyperglycemic events for insulin-treated residents in skilled nursing facilities.86
Management of cardiovascular risk factors
The risk of cardiovascular disease (CVD) is 7.7-fold higher in women with type 1 diabetes and 3.6-fold higher in men with type 1 diabetes compared to those without diabetes.87 High CVD risk is associated with nephropathy88,89 and the presence of the metabolic syndrome.90–92 No large trials have focused on management of cardiovascular risk factors in older adults with type 1 diabetes. ADA/AGS recommendations (Table 3) are primarily based on studies that included all older adults with diabetes.
Blood pressure. The goal for treatment of hypertension in healthy older adults and frail older adults without end-stage chronic illness who have type 1 diabetes is < 140/80 mmHg. The ADA/AGS guidelines recommend a higher systolic and diastolic blood pressure target (< 150/90 mmHg) in older adults with poor health status, end-stage chronic illness, or short life expectancy and those residing in LTC facilities.
The European Society of Hypertension/European Society of Cardiology 2013 guidelines for treating hypertension in the elderly recommend the following: 1) in the elderly with systolic blood pressure ≥ 160 mmHg, reduce to 140–150 mmHg; 2) in fit elderly patients < 80 years of age with initial systolic blood pressure ≥ 140 mmHg, consider treatment to < 140 mmHg; 3) in elderly patients > 80 years of age in good physical and mental condition with an initial systolic blood pressure ≥ 160 mmHg, reduce to 140–150 mmHg; 4) in frail elderly patients, treatment is at the discretion of the physician; 5) the diastolic blood pressure goal for patients with diabetes is < 85 mmHg; and 6) well-tolerated antihypertensive medications should be continued with advanced age unless considered unsafe.93
Blood pressure should be lowered gradually to reduce the risk of hypotensive symptoms, especially in the frail elderly. Renal function and serum potassium should be monitored within 1–2 weeks of initiation of therapy for those taking ACE inhibitors or angiotensin receptor blockers and at least yearly thereafter. If diuretics are used to treat hypertension, electrolytes should be monitored within 1–2 weeks of initiation of therapy and periodically thereafter.
Lipids. The ADA recommends annual monitoring of the fasting lipid profile. In the presence of overt CVD, the goal for LDL cholesterol is < 70 mg/dl. In the absence of overt CVD, the LDL goal is < 100 mg/dl. The triglyceride goal is < 150 mg/dl, and HDL cholesterol goals are > 40 mg/dl in men and > 50 mg/dl in women. Statin therapy is indicated in healthy older adults and frail older adults with complex health status to reduce CVD morbidity and mortality, unless contraindicated or not tolerated. In older adults with poor health status and those residing in LTC facilities, life expectancy should be considered when determining the benefit of statin therapy. The use of other lipid-lowering medications alone or in combination has not been shown to be of benefit in older adults with type 1 diabetes.
Aspirin. The role of aspirin for primary prevention of CVD in older adults with type 1 diabetes is unclear. In healthy adults, aspirin (75–162 mg/day) is generally recommended for those with high CVD risk (10-year risk > 10%, including older adults with one additional risk factor). Aspirin is also used in patients with known CVD for secondary prevention. The potential benefits of aspirin therapy should be weighed against the risk of bleeding in these individuals, especially in older adults with multiple medical conditions, severe cognitive impairment, or a high risk for falls.
Conclusion
Older adults with type 1 diabetes are a heterogeneous group and have not been well studied. With long-duration diabetes, hypoglycemia is common, regardless of A1C level. Individualized treatment plans using more complex insulin regimens and lower glycemic goals with frequent SMBG are recommended in healthy older adults. For individuals with poor health status and frailty, modifications are suggested. Older adults should be assessed for hypo- and hyperglycemia; hypertension; physical disabilities; vision, hearing, and cognitive impairments; pain; social support; urinary incontinence; polypharmacy; depression; nutritional deficits; fall risk; and the need for social services. The treatment plan should focus on minimizing hypoglycemia and serious hyperglycemia and should address identified physical, emotional, and social challenges to enhance safety and quality of life. In the future, new insulin preparations and technological advances are expected to contribute to better therapeutic approaches for this growing population.
References
- 1.DIAMOND project group : Incidence and trends of childhood type 1 diabetes worldwide 1990–1999. Diabet Med 23:857–866, 2006 [DOI] [PubMed] [Google Scholar]
- 2.Patterson CC, Dahlquist GG, Gyürüs E, Green A, Soltész G; EURODIAB study group: Incidence trends for childhood type 1 diabetes in Europe during 1989–2003 and predicted new cases 2005–20: a multicentre prospective registration study. Lancet 373:2027–2033, 2009 [DOI] [PubMed] [Google Scholar]
- 3.International Diabetes Federation : Diabetes Atlas. 5th ed. Brussels, Belgium, International Diabetes Federation, 2011 [Google Scholar]
- 4.Schutt M, Fach EM, Seufert J, Kerner W, Lang W, Zeyfang A, Welp R, Holl RW; DPV Initiative and the German BMBF Competence Network Diabetes Network: Multiple complications and frequent severe hypoglycaemia in ‘elderly’ and ‘old’ patients with type 1 diabetes. Diabet Med 29:e176–e179, 2012 [DOI] [PubMed] [Google Scholar]
- 5.DCCT Research Group : The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 329:977–986, 1993 [DOI] [PubMed] [Google Scholar]
- 6.Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ, Raskin P, Zinman B; DCCT⁄EDIC Study Research Group: Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 353:2643–2653, 2005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.White NH, Sun W, Cleary PA, Danis RP, Davis MD, Hainsworth DP, Hubbard LD, Lachin JM, Nathan DM: Prolonged effect of intensive therapy on the risk of retinopathy complications in patients with type 1 diabetes mellitus: 10 years after the Diabetes Control and Complications Trial. Arch Ophthalmol 126:1707–1715, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Brown AF, Mangione CM, Saliba D, Sarkisian CA; California Healthcare Foundation/American Geriatrics Society Panel on Improving Care for Elders with Diabetes: Guidelines for improving the care of the older person with diabetes mellitus. J Am Geriatr Soc 51(5 Suppl. guidelines):S265–S280, 2003 [DOI] [PubMed] [Google Scholar]
- 9.American Diabetes Association : Economic costs of diabetes in the U.S. in 2012. Diabetes Care 36:1033–1046, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Thunander M, Petersson C, Jonzon K, Fornander J, Ossiansson B, Torn C, Edvardsson S, Landin-Olsson M: Incidence of type 1 and type 2 diabetes in adults and children in Kronoberg, Sweden. Diabetes Res Clin Pract 82:247–255, 2008 [DOI] [PubMed] [Google Scholar]
- 11.Turner R, Stratton I, Horton V, Manley S, Zimmet P, Mackay IR, Shattock M, Bottazzo GF, Holman R: UKPDS 25: Autoantibodies to islet-cell cytoplasm and glutamic acid decarboxylase for prediction of insulin requirement in type 2 diabetes. Lancet 350:1288–1293, 1997 [DOI] [PubMed] [Google Scholar]
- 12.Merger SR, Leslie RD, Boehm BO: The broad clinical phenotype of type 1 diabetes at presentation. Diabet Med 30:170–178, 2013 [DOI] [PubMed] [Google Scholar]
- 13.Palmer JP, Fleming GA, Greenbaum CJ, Herold KC, Jansa LD, Kolb H, Lachin JM, Polonsky KS, Pozzilli P, Skyler JS, Steffes MW: C-peptide is the appropriate outcome measure for type 1 diabetes clinical trials to preserve beta-cell function: report of an ADA workshop, 21–22 October 2001. Diabetes 53:250–264, 2004 [DOI] [PubMed] [Google Scholar]
- 14.DCCT Research Group : Effect of intensive therapy on residual beta-cell function in patients with type 1 diabetes in the Diabetes Control and Complications Trial: a randomized, controlled trial. Ann Intern Med 128:517–523, 1998 [DOI] [PubMed] [Google Scholar]
- 15.Livingstone SJ, Looker HC, Hothersall EJ, Wild SH, Lindsay RS, Chalmers J, Cleland S, Leese GP, McKnight J, Morris AD, Pearson DW, Peden NR, Petrie JR, Philip S, Sattar N, Sullivan F, Colhoun HN: Risk of cardiovascular disease and total mortality in adults with type 1 diabetes: Scottish Registry Linkage Study. PLoS Med 9:e1001321, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jacobson AM, Braffett BH, Cleary PA, Gubitosi-Klug RA, Larkin ME, DCCT/EDIC Research Group: The long-term effects of type 1 diabetes treatment and complications on health-related quality of life: a 23-year follow-up of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications cohort. Diabetes Care 36:3131–3138, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Beck RW, Tamborlane WV, Bergenstal RM, Miller KM, Dubose SN, Hall CA: The T1D Exchange Clinic Registry. J Clin Endocrinol Metab 97:4383–4389, 2012 [DOI] [PubMed] [Google Scholar]
- 18.Miller KM, Beck RW, Bergenstal RM, Goland RS, Haller MJ, McGill JB, Rodriguez H, Simmons JH, Hirsch IB: T1D Exchange Clinic network: evidence of a strong association between frequency of self-monitoring of blood glucose, hemoglobin A1C levels in T1D Exchange Clinic Registry participants. Diabetes Care 36:2009–2014, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Weinstock RS, Xing D, Maahs DM, Michels A, Rickels MR, Peters AL, Bergenstal RM, Harris B, Dubose SN, Miller KM, Beck RW; for the T1D Exchange Clinic Network: Severe hypoglycemia and diabetic ketoacidosis in adults with type 1 diabetes: results from the T1D Exchange Clinic Registry. J Clin Endocrinol Metab 98:3411–3419, 2013 [DOI] [PubMed] [Google Scholar]
- 20.Laiteerapong N, Karter AJ, Liu JY, Moffet HH, Sudore R, Schillinger D, John PM, Huang ES: Correlates of quality of life in older adults with diabetes: the Diabetes & Aging Study. Diabetes Care 34:1749–1753, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Inouye SK, Studenski S, Tinetti ME, Kuchel GA: Geriatric syndromes: clinical, research, and policy implications of a core geriatric concept. J Am Geriatr Soc 55:780–791, 2007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cigolle CT, Langa KM, Kabeto MU, Tian Z, Blaum CS: Geriatric conditions and disability: the Health and Retirement Study. Ann Intern Med 147:156–164, 2007 [DOI] [PubMed] [Google Scholar]
- 23.Lee PG, Cigolle C, Blaum C: The co-occurrence of chronic diseases and geriatric syndromes: the Health and Retirement Study. J Am Geriatr Soc 57:511–516, 2009 [DOI] [PubMed] [Google Scholar]
- 24.JDRF Continuous Glucose Monitoring Study Group : Effectiveness of continuous glucose monitoring in a clinical care environment: evidence from the JDRF Continuous Glucose Monitoring trial. Diabetes Care 33:17–22, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.MacLeod KM, Hepburn DA, Frier BM: Frequency and morbidity of severe hypoglycaemia in insulin-treated diabetic patients. Diabet Med 10:238–245, 1993 [DOI] [PubMed] [Google Scholar]
- 26.Microvascular and acute complications in IDDM patients : the EURODIAB IDDM Complications study. Diabetologia 37:278–285, 1994 [DOI] [PubMed] [Google Scholar]
- 27.ter Braak EW , Appelman AM, van de Laak M, Stolk RP, van Haeften TW, Erkelens DW: Clinical characteristics of type 1 diabetic patients with and without severe hypoglycemia. Diabetes Care 23:1467–1471, 2000 [DOI] [PubMed] [Google Scholar]
- 28.McCoy RG, Van Houten HK, Ziegenfuss JY, Shah ND, Wermers RA, Smith SA: Increased mortality of patients with diabetes reporting severe hypoglycemia. Diabetes Care 35:1897–1901, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Nordin C: The case for hypoglycaemia as a proarrhythmic event: basic and clinical evidence. Diabetologia 53:1552–1561, 2010 [DOI] [PubMed] [Google Scholar]
- 30.Bree AJ, Puente EC, Daphna-Iken D, Fisher SJ: Diabetes increases brain damage caused by severe hypoglycemia. Am J Physiol Endocrinol Metab 297:e194–e201, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kodl CT, Seaquist ER: Cognitive dysfunction and diabetes mellitus. Endocr Rev 29:494–511, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Gold AE, MacLeod KM, Frier BM: Frequency of severe hypoglycemia in patients with type 1 diabetes with impaired awareness of hypoglycemia. Diabetes Care 17:697–703, 1994 [DOI] [PubMed] [Google Scholar]
- 33.Matyka K, Evans M, Lomas J, Cranston I, Macdonald I, Amiel SA: Altered hierarchy of protective responses against severe hypoglycemia in normal aging in healthy men. Diabetes Care 20:135–141, 1997 [DOI] [PubMed] [Google Scholar]
- 34.Brierley EJ, Broughton DL, James OF, Alberti KG: Reduced awareness of hypoglycaemia in the elderly despite an intact counterregulatory response. Q J Med 88:439–445, 1995 [PubMed] [Google Scholar]
- 35.Bremer JP, Jauch-Chara K, Hallschmid M, Schmid S, Schultes B: Hypoglycemia unawareness in older compared with middle-aged patients with type 2 diabetes. Diabetes Care 32:1513–1517, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cryer PE: Hypoglycemia in type 1 diabetes mellitus. Endocrinol Metab Clin North Am 39:641–654, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hypoglycaemia Study Group UK: Risk of hypoglycaemia in types 1 and 2 diabetes: effects of treatment modalities and their duration. Diabetologia 50:1140–1147, 2007 [DOI] [PubMed] [Google Scholar]
- 38.Trief PM, Xing D, Kittlesrud J, Olson BA, Young L, Peters A, Miller KM, Beck R, Weinstock RS: Depression in adults with type 1 diabetes participating in the T1D Exchange clinic registry. Presented at the 73rd American Diabetes Association Scientific Session, Chicago, Ill., June 2013. Diabetes 62 (Suppl. 1):808–P, 2013 [Google Scholar]
- 39.Anderbro T, Amsberg S, Adamson U, Bolinder J, Lins PE, Wredling R, Moberg E, Lisspers J, Johansson UB: Fear of hypoglycaemia in adults with type 1 diabetes. Diabet Med 27:1151–1158, 2010 [DOI] [PubMed] [Google Scholar]
- 40.Kirkman MS, Briscoe VJ, Clark N, Florez H, Haas LB, Halter JB, Huang ES, Korytkowski MT, Munshi MN, Odegard PS, Pratley RE, Swift CS; Consensus Development Conference on Diabetes and Older Adults: Diabetes in older adults: a consensus report. J Am Geriatr Soc 60:2342–2356, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Action to Control Cardiovascular Risk in Diabetes Study Group. Gerstein HC, Miller ME, Byington RP, Goff DC, Jr, Bigger JT, Buse JB, Cushman WC, Genuth S, Ismail-Beigi F, Grimm RH, Jr, Probstfield JL, Simons-Morton DG, Friedewald WT: Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med 358:2545–2559, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Duckworth W, Abraira C, Moritz T, Reda D, Emanuele N, Reaven PD, Zieve FJ, Marks J, Davis SN, Hayward R, Warren SR, Goldman S, McCarren M, Vitek ME, Henderson WG, Huang GD; VADT Investigators: Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 360:129–139, 2009 [DOI] [PubMed] [Google Scholar]
- 43.ADVANCE Collaborative Group. Patel A, MacMahon S, Chalmers J, Neal B, Billot L, Woodward M, Marre M, Cooper M, Glasziou P, Grobbee D, Hamet P, Harrap S, Heller S, Liu L, Mancia G, Mogensen CE, Pan C, Poulter N, Rodgers A, Williams B, Bompoint S, de Galan BE, Joshi R, Travert F: Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 358:2560–2572, 2008 [DOI] [PubMed] [Google Scholar]
- 44.Hope SZ, Strain WD: Hypoglycemia in the elderly. Diabetic Hypoglycemia 6:3–10, 2013 [Google Scholar]
- 45.Munshi MN, Segal AR, Suhl E, Staum E, Desrochers L, Sternthal A, Giusti J, McCartney R, Lee Y, Bonsignore P, Weinger K: Frequent hypoglycemia among elderly patients with poor glycemic control. Arch Intern Med 171:362–364, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Huang ES, Liu JY, Moffet HH, John PM, Karter AJ: Glycemic control, complications, and death in older diabetic patients: the Diabetes and Aging Study. Diabetes Care 34:1329–1336, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Piette JD, Kerr EA: The impact of comorbid chronic conditions on diabetes care. Diabetes Care 29:725–731, 2006 [DOI] [PubMed] [Google Scholar]
- 48.Laiteerapong N, Huang ES, Chin MH: Prioritization of care in adults with diabetes and comorbidity. Ann N Y Acad Sci 1243:69–87, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Centers for Disease Control and Prevention : Vision health initiative. Available at http://www.cdc.gov/visionhealth/data/index.htm. Accessed 6 July 2013
- 50.Bainbridge KE, Hoffman HJ, Cowie CC: Diabetes and hearing impairment in the United States: audiometric evidence from the National Health and Nutrition Examination Survey, 1999 to 2004. Ann Intern Med 149:1–10, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bainbridge KE, Hoffman HJ, Cowie CC: Risk factors for hearing impairment among U.S. adults with diabetes: National Health and Nutrition Examination Survey 1999–2004. Diabetes Care 34:1540–1545, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Khan MI, Barlow RW, Weinstock RS: Acute hypoglycemia decreases central retinal function in the human eye. Vision Res 51:1623–1626, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Sarma AV, Kanaya AM, Nyberg LM, Kusek JW, Vittinghoff E, Rutledge B, Cleary PA, Gatcomb P, Brown JS; DCCT/EDIC Research Group: Urinary incontinence among women with type 1 diabetes–how common is it? J Urol 181:1224–1230, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Jackson SL, Scholes D, Boyko EJ, Abraham L, Fihn SD: Urinary incontinence and diabetes in postmenopausal women. Diabetes Care 28:1730–1738, 2005 [DOI] [PubMed] [Google Scholar]
- 55.Campanelli CM; American Geriatrics Society 2012 Beers Criteria Update Expert Panel: American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 60:616–631, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Villareal DT, Banks M, Siener C, Sinacore DR, Klein S: Physical frailty and body composition in obese elderly men and women. Obes Res 12:913–920, 2004 [DOI] [PubMed] [Google Scholar]
- 57.Miller SL, Wolfe RR: The danger of weight loss in the elderly. J Nutr Health Aging 12:487–491, 2008 [DOI] [PubMed] [Google Scholar]
- 58.Shapses SA, Riedt CS: Bone, body weight, and weight reduction: what are the concerns? J Nutr 136:1453–1456, 2006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Brands AM, Biessels GJ, de Haan EH, Kappelle LJ, Kessels RP: The effects of type 1 diabetes on cognitive performance: a meta-analysis. Diabetes Care 28:726–735, 2005 [DOI] [PubMed] [Google Scholar]
- 60.Cox DJ, Kovatchev BP, Gonder-Frederick LA, Summers KH, McCall A, Grimm KJ, Clarke WL: Relationships between hyperglycemia and cognitive performance among adults with type 1 and type 2 diabetes. Diabetes Care 28:71–77, 2005 [DOI] [PubMed] [Google Scholar]
- 61.Rovet J, Alvarez M: Attentional functioning in children and adolescents with IDDM. Diabetes Care 20:803–810, 1997 [DOI] [PubMed] [Google Scholar]
- 62.Sommerfield AJ, Deary IJ, Frier BM: Acute hyperglycemia alters mood state and impairs cognitive performance in people with type 2 diabetes. Diabetes Care 27:2335–2340, 2004 [DOI] [PubMed] [Google Scholar]
- 63.Inkster B, Frier BM: The effects of hypoglycaemia on cognitive function in type 1 diabetes. Br J Diabetes Vasc Dis 12:221–226, 2012 [Google Scholar]
- 64.Gregg EW, Beckles GL, Williamson DF, Leveille SG, Langlois JA, Engelgau MM, Narayan KM: Diabetes and physical disability among older U.S. adults. Diabetes Care 23:1272–1277, 2000 [DOI] [PubMed] [Google Scholar]
- 65.Sinclair AJ, Conroy SP, Bayer AJ: Impact of diabetes on physical function in older people. Diabetes Care 31:233–235, 2008 [DOI] [PubMed] [Google Scholar]
- 66.Richardson JK, Thies SB, DeMott TK, Ashton-Miller JA: Gait analysis in a challenging environment differentiates between fallers and nonfallers among older patients with peripheral neuropathy. Arch Phys Med Rehabil 86:1539–1544, 2005 [DOI] [PubMed] [Google Scholar]
- 67.Buman MP, Hekler EB, Haskell WL, Pruitt L, Conway TL, Cain KL, Sallis JF, Saelens BE, Frank LD, King AC: Objective light-intensity physical activity associations with rated health in older adults. Am J Epidemiol 172:1155–1165, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.American Geriatrics Society : AGS/BGS clinical practice guideline: Prevention of falls in older persons, 2010 Available from http://www.americangeriatrics.org/health_care_professionals/clinical_practice/clinical_guidelines_recommendations/2010. Accessed 6 June 2013 [Google Scholar]
- 69.Volpato S, Leveille SG, Blaum C, Fried LP, Guralnik JM: Risk factors for falls in older disabled women with diabetes: the women’s health and aging study. J Gerontol A Biol Sci Med Sci 60A:1539–1545, 2005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Schwartz AV, Hillier TA, Sellmeyer DE, Resnick HE, Gregg E, Ensrud KE, Schreiner PJ, Margolis KL, Cauley JA, Nevitt MC, Black DM, Cummings SR: Older women with diabetes have a higher risk of falls: a prospective study. Diabetes Care 25:1749–1754, 2002 [DOI] [PubMed] [Google Scholar]
- 71.Bonds DE, Larson JC, Schwartz AV, Strotmeyer ES, Robbins J, Rodriguez BL, Johnson KC, Margolis KL: Risk of fracture in women with type 2 diabetes: the Women’s Health Initiative Observational Study. J Clin Endocrinol Metab 91:3404–3410, 2006 [DOI] [PubMed] [Google Scholar]
- 72.National Osteoporosis Foundation : 2013. clinician’s guide to prevention and treatment of osteoporosis. Available from http://www.nof.org/files/nof/public/content/file/950/upload/523.pdf. Accessed 22 September 2013
- 73.Roy T, Lloyd CE: Epidemiology of depression and diabetes: a systematic review. J Affect Disord 142 (Suppl):S8–S21, 2012 [DOI] [PubMed] [Google Scholar]
- 74.Lin EH, Katon W, Von Korff M, Rutter C, Simon GE, Oliver M, Ciechanowski P, Ludman EJ, Bush T, Young B: Relationship of depression and diabetes self-care, medication adherence, and preventive care. Diabetes Care 27:2154–2160, 2004 [DOI] [PubMed] [Google Scholar]
- 75.Peyrot M, McMurray JF, Jr, Kruger DF: A biopsychosocial model of glycemic control in diabetes: stress, coping and regimen adherence. J Health Soc Behav 40:141–158, 1999 [PubMed] [Google Scholar]
- 76.Munshi MN, Segal AR, Suhl E, Ryan C, Sternthal A, Giusti J, Lee Y, Fitzgerald S, Staum E, Bonsignor P, DesRochers L, McCartney R, Weinger K: Assessment of barriers to improve diabetes management in older adults. Diabetes Care 36:543–549, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA; Cardiovascular Health Study Collaborative Research Group: Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 56:M146–M156, 2001 [DOI] [PubMed] [Google Scholar]
- 78.Heise T, Nosek L, Rønn BB, Endahl L, Heinemann L, Kapitza C, Draeger E: Lower within-subject variability of insulin detemir in comparison to NPH insulin and insulin glargine in people with type 1 diabetes. Diabetes 53:1614–1620, 2004 [DOI] [PubMed] [Google Scholar]
- 79.Poon K, King AB: Glargine and detemir: safety and efficacy profiles of the long-acting basal insulin analogs. Drug Health Patient Saf 2:213–223, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Pieber TR, Treichel HC, Hompesch B, Philotheou A, Mordhorst L, Gall MA, Robertson LI: Comparison of insulin detemir and insulin glargine in subjects with type 1 diabetes using intensive insulin therapy. Diabet Med 24:635–642, 2007 [DOI] [PubMed] [Google Scholar]
- 81.Misso ML, Egberts KJ, Page M, O’Connor D, Shaw J: Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus. Cochrane Database Syst Rev 2010, CD005103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Bergenstal RM, Klonoff DC, Garg SK, Bode BW, Meredith M, Slover RH, Ahmann AJ, Welsh JB, Lee SW, Kaufman FR; for the ASPIRE In-Home Study Group: Threshold-based insulin pump interruption for reduction of hypoglycemia. N Engl J Med 369:224–232, 2013 [DOI] [PubMed] [Google Scholar]
- 83.Dybicz SB, Thompson S, Molotsky S, Stuart B: Prevalence of diabetes and the burden of comorbid conditions among elderly nursing home residents. Am J Geriatr Pharmacother 9:212–223, 2011 [DOI] [PubMed] [Google Scholar]
- 84.Travis SS, Buchanan RJ, Wang S, Kim M: Analyses of nursing home residents with diabetes at admission. J Am Med Dir Assoc 5:320–327, 2004 [PubMed] [Google Scholar]
- 85.Migdal A, Yarandi SS, Smiley D, Umpierrez GE: Update on diabetes in the elderly and in nursing home residents. J Am Med Dir Assoc 12:627–632, 2011 [DOI] [PubMed] [Google Scholar]
- 86.Dy P, Morin PC, Weinstock RS: Use of telemedicine to improve glycemic management in a skilled nursing facility: a pilot study. Telemed J E Health 19:643–645, 2013 [DOI] [PubMed] [Google Scholar]
- 87.Soedamah-Muthu SS, Fuller JH, Mulnier HE, Raleigh VS, Lawrenson RA, Colhoun HM: High risk of cardiovascular disease in patients with type 1 diabetes in the U.K.: a cohort study using the general practice research database. Diabetes Care 29:798–804, 2006 [DOI] [PubMed] [Google Scholar]
- 88.Groop PH, Thomas MC, Moran JL, Waden J, Thorn LM, Makinen VP, Rosengard-Barlund M, Saraheimo M, Hietala K, Heikkila O, Forsblom C; FinnDiane Study Group: The presence and severity of chronic kidney disease predicts all-cause mortality in type 1 diabetes. Diabetes 58:1651–1658, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Beijers HJ, Ferreira I, Bravenboer B, Dekker JM, Nijpels G, Heine RJ, Stehouwer CD: Microalbuminuria and cardiovascular autonomic dysfunction are independently associated with cardiovascular mortality: evidence for distinct pathways: the Hoorn Study. Diabetes Care 32:1698–1703, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.McGill M, Molyneaux L, Twigg SM, Yue DK: The metabolic syndrome in type 1 diabetes: does it exist and does it matter? J Diabetes Complications 22:18–23, 2008 [DOI] [PubMed] [Google Scholar]
- 91.Purnell JQ, Zinman B, Brunzell JD; DCCT/EDIC Research Group: The effect of excess weight gain with intensive diabetes mellitus treatment on cardiovascular disease risk factors and atherosclerosis in type 1 diabetes mellitus: results from the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study (DCCT/EDIC) study. Circulation 127:180–187, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Thorn LM, Forsblom C, Waden J, Saraheimo M, Tolonen N, Hietala K, Groop PH; Finnish Diabetic Nephropathy (FinnDiane) Study Group: Metabolic syndrome as a risk factor for cardiovascular disease, mortality, and progression of diabetic nephropathy in type 1 diabetes. Diabetes Care 32:950–952, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Task Force for the Management of Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) : 2013 ESH/ESC guidelines for the management of arterial hypertension. J Hypertens 31:1281–1357, 2013 [DOI] [PubMed] [Google Scholar]
- 94.American Diabetes Association : Standards of medical care in diabetes—2013. Diabetes Care 36 (Suppl. 1):S11–S66, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.2012 aids for insulin users Diabetes Forecast. January 2012 Available from http://forecast.diabetes.org/magazine/features/2012-aids-insulin-users. Accessed 1 August 2013. [PubMed] [Google Scholar]