

Abstract
In Brief
Physiological changes associated with aging have the potential to affect the treatment of diabetes. However, evidence regarding treatment of diabetes in geriatric patients has been limited, especially for “oldest-old” patients. Recent research has provided greater insight into the risks and benefits of treatment, and new guidelines provide more specific information regarding treatment goals in older people with diabetes and encourage greater individualization of treatment.
Geriatric patients make up an important part of the overall diabetes population. The Centers for Disease Control and Prevention estimates that, including undiagnosed patients, 10.9 million, or 26.9% of the population ≥ 65 years of age have diabetes.1
One challenge in treating geriatric patients is that this group can have a wide range of ages and medical conditions. For example, one geriatric patient could be a 65-year-old man who has been recently diagnosed with type 2 diabetes and has mild hypertension and hyperlipidemia but who is otherwise healthy, whereas another patient could be an 86-year-old woman with a history of type 2 diabetes for several years, an A1C of 8.6%, and concurrent conditions, including hypertension, hyperlipidemia, coronary artery disease, arthritis, and vision and hearing impairments. Given this level of heterogeneity, it is important to identify in all patients any changes associated with aging and to consider how these circumstances will affect treatment as aging continues.
More specifically defining the term “geriatric” can aid in this process. Although the age of 60 or 65 years is often used as the defining criterion, there can be significant differences between a patient who is 65 and someone who is 90 years of age. Other definitions divide geriatrics into broader age ranges, and, although this can vary, a common classification system is youngest-old (65–74 years of age), middle-old (75–85 years), and oldest-old (> 85 years).
Despite the changes that occur with aging, individuals with advanced age and comorbidities often are excluded from randomized, controlled trials.2 Therefore, providing true evidence-based care to geriatric patients may be difficult, making it all the more important for clinicians to be aware of key changes that occur with aging and how these can affect the use of various medications for the treatment of diabetes. This article reviews some of the significant aging-related physiological and social changes that could affect diabetes care, recent changes in treatment recommendations for older patients with diabetes, and medication considerations that are especially important in the elderly population.
Age-Related Changes that May Affect Diabetes Treatment
Some important changes associated with aging that can affect medication use are classified as either pharmacokinetic (what the body does to a medication) or pharmacodynamic (what the medication does to the body). However, as discussed below, there are additional factors that also may affect how particular medications will act in elderly patients.
Pharmacokinetic changes
Perhaps the most commonly considered aging-related physiological change with regard to medications is the potential decrease in renal function that can occur with advancing age and affect some medications. However, the rate of renal decline is not uniformly predictable as patients age;3 hence, the doses of a renally adjusted medication may not need to be decreased for all older patients. Although some diabetes medications are affected by changes in renal function, the variability of age-related renal decline means that dosing decisions should not be based on patients’ age alone.
Hepatic drug metabolism also can be affected by aging. However, aging does not affect all metabolic pathways in the liver to the same degree, and changes in drug metabolism can vary substantially from one patient to another.4–7 The first-generation sulfonylurea chlorpropamide is a classic example of a diabetes therapy that is affected by aging-related physiological changes. This agent should be avoided in older patients because decreased hepatic metabolism brought on by aging can lengthen its half-life in the body.8
Pharmacodynamic changes
Older patients may be more sensitive to the effects of medications, such as the glucose-lowering action of antihyperglycemic agents or the orthostatic effects of antihypertensive therapies.9 On the other hand, in some cases, older patients may demonstrate a decreased response to some medications. For example, older patients tend to have reduced sympathetic nervous system responses9 and thus may also have a decreased response to medications such as β-blockers or βagonists, which affect the adrenergic system.10
Hypoglycemia unawareness
The decreased central nervous system responses that are common with aging also may play a role in the development of hypoglycemia unawareness. In one study comparing 13 people with diabetes ≥ 65 years of age to 13 people with diabetes aged 39–64 years,11 those in the older age-group maintained hormonal responses to hypoglycemia but exhibited more hypoglycemia unawareness, indicating a possible decreased sensitivity to hormonal responses. The authors noted that a lack of hypoglycemia symptoms also has been linked to a longer duration of diabetes, which could have been an additional contributing factor.11 Because some older patients may have had diabetes for an extended period of time, the possibility of increased hypoglycemia unawareness must be considered.
Changes in functional status
Diabetes may have an effect on patients’ functional status, which could, in turn, affect their medical care. In the Study of Osteoporotic Fractures,12 women with diabetes had a 42% increased risk of any functional disability, as well as an increased risk of disability for specific tasks. Women with diabetes also had an increase in the number of falls.13 Interestingly, women with diabetes who were not taking insulin had a higher risk of falling than those who took insulin. This was attributed to a greater number of risk factors for falls in the group not treated with insulin13 and highlights the high number of comorbidities that could be present in some people with diabetes. Because hyperglycemia can cause functional impairment, it is important to adequately control glycemia to avoid complications that could complicate treatment later in life.
Diabetes was been found to be an independent risk factor for hearing loss based on audiometric testing as part of the National Health and Nutrition Examination Survey.14 Multiple diabetes-related factors, including peripheral neuropathy, coronary heart disease, low HDL cholesterol, and general poor health, were all associated with an increased likelihood of hearing impairment.15
Multiple studies have also investigated cognitive function and diabetes. Cognitive dysfunction has been linked to both hyper-16 and hypoglycemia.17 Further, it has been linked to a greater likelihood of experiencing severe hypoglycemia.18 Although dementia tends to increase with age in the general population, a systematic review and meta-analysis19 found that diabetes is associated with a faster rate of decline in cognitive function among older adults, with the relative risk for dementia in people with diabetes being 1.47 (95% CI 1.25–1.73) compared to people without diabetes.
In addition to these limitations, concomitant conditions, whether related to diabetes (e.g., visual impairment), or not (e.g., arthritis), could affect older patients’ ability to perform tasks such as reading prescription labels and administering insulin. Consideration of such limitations is important when designing a therapy regimen for older adults. For those with cognitive or other functional impairments, keeping the regimen as simple as possible is essential.2,20
Multiple chronic conditions
In treating older patients, the existence of comorbidities must be considered along with natural changes of the aging process. Huang et al.21 analyzed data in older people with diabetes and determined that multiple comorbidities (and the functional impairments that may accompany them) were greater predictors than age alone of both shorter life expectancy and lack of benefit of intensive blood glucose control. The presence of comorbidities also can increase the risk of medication-related complications. For example, the possibility of drug-drug interactions and the use of medications that could negatively affect diabetes (e.g., corticosteroids) can increase as more medications are needed to treat comorbidities. In addition, hyperglycemia can be an even greater problem for patients with comorbidities. For example, nephropathy can compound age-related changes in renal function, neuropathy can complicate other functional impairments, and bed-bound patients are potentially at greater risk of problematic wounds if their glycemic control is poor.
The presence of multiple medical conditions also may affect patients’ attitudes toward treatment. A study using a semi-structured interview22 found that older people with diabetes were more concerned about their functional status and ability to maintain activities of daily living than they were about their specific diabetes treatment goals. The authors recommended that practitioners explore patients’ goals and individual circumstances as part of developing an appropriate treatment plan.22 This type of discussion allows patients to help with prioritization and encourages shared decision-making.23
Cost Issues Affecting the Care of Older Adults With Diabetes
Cost can be an important issue for older adults, many of whom are living on a fixed income. Even for patients with Medicare Part D (prescription coverage), clinicians must remember that more expensive medications may have a high-tier status and therefore a high and potentially unaffordable required copayment. The so-called “doughnut hole” in Medicare Part D (i.e., the gap in prescription coverage between the upper limit of initial coverage and the threshold for catastrophic care coverage) may also become an issue even for patients who can afford their initial prescription copayments. Although the doughnut hole is scheduled to be gradually eliminated by 2020,24 additional out-of-pocket costs for patients whose expenses fall within that gap may remain a significant hurdle for some patients until then.
Safety of Intensive Glycemic Control in Older Patients
There is no doubt that glycemic control remains important even as patients continue to age. Geriatric patients are prone to develop all of the same diabetes complications as younger patients. However, the question of how aggressively glycemia should be targeted in geriatrics has been the subject of much debate.
Recent research studies have suggested the need for greater caution with regard to intensive glycemic control as patients age or develop serious comorbidities. The Veterans Affairs Diabetes Trial (VADT)25 and the ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation) trial26 did not find a decrease in mortality with intensive glycemic control but did find benefits for albuminuria and nephropathy, respectively. Although the ACCORD (Action to Control Cardiovascular Risk in Diabetes) trial27 was halted early because of concerns about increased mortality with intensive control in younger patients, no increase in mortality was found in patients ≥ 65 years of age. Because those studies identified some overall benefits to intensive control of diabetes, they did not result in changes to general diabetes treatment guidelines. However, all three of these studies, for which the mean age of subjects was in the range of 60–70 years, emphasized the need for individualized treatment, taking factors such as age and comorbidities into account.28 Still, the extent to which their findings can be extrapolated to the oldest geriatric patients and those with increased comorbidities is limited because of the studies’ exclusion criteria.
Retrospective analyses of large patient databases have provided some evidence to further quantify the results from these trials. These analyses have the advantage of including frail patients who generally are excluded from randomized trials, but their findings must be interpreted carefully with regard to the number of variables potentially affecting outcomes. Two such analyses,29,30 which focused specifically on older patients (one involved patients ≥ 50 years and the other involved patients ≥ 60 years), found a U-shaped relationship between A1C and mortality, indicating both the importance of glycemic control and the need for caution against overtreatment in older patients. Additionally, a 5-year observational study designed to assess the impact of comorbidity on cardiovascular outcomes31 found that tight glycemic control at baseline (target A1C < 6.5 or < 7.0%) was beneficial for cardiovascular outcomes for patients with mild comorbidity but not for those with a high level of comorbidity.
One likely explanation for these observations is increased hypoglycemia from intensive control. Like hyperglycemia, hypoglycemia has been linked to cardiovascular disease (CVD),32 and older patients may be at greater risk of hypoglycemia for a variety of reasons. The emergency room visitation rate for hypoglycemia increases substantially with age, with those ≥ 75 years of age having nearly double the rate of those 65–74 years of age and triple the rate of those 45–64 years of age.33 An article examining the reasons for medication-related emergency department visits by older adults found that insulin and oral hypoglycemic agents were two of the most common causes, resulting in 13.9 and 10.7% of the hospitalizations, respectively.34
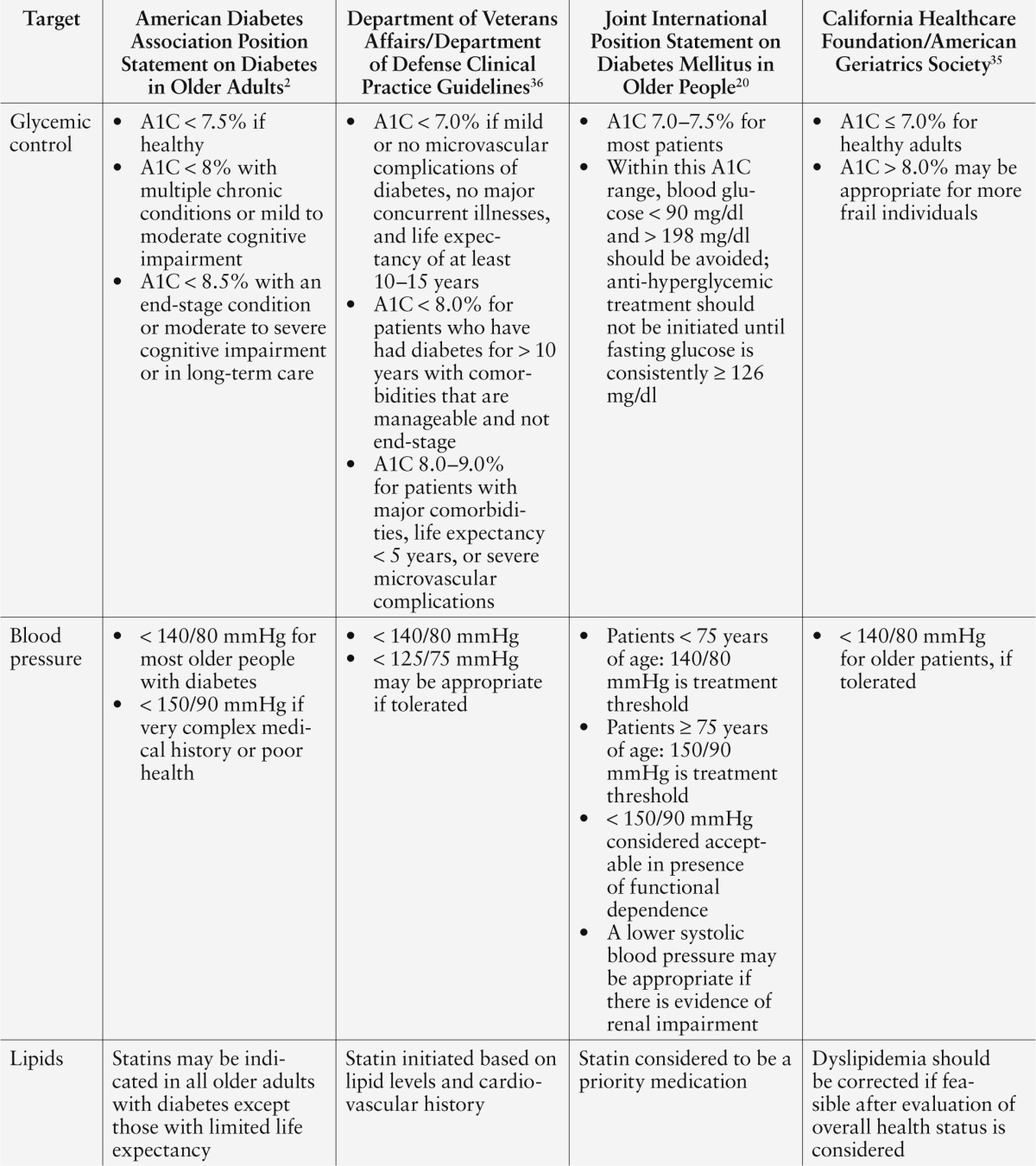
Findings such as these, coupled with the fact that a time period of as long as 8 years may be required to see the benefits of intensive glucose treatment,35 have shaped more recent guidelines for appropriate blood glucose targets in older individuals. A summary of recommendations for the management of hyperglycemia in older patients is offered in Table 1.2,20,35,36 When considering the effects of hypoglycemia and the individualization of treatment, daily blood glucose readings may be a better indicator than A1C alone. Some older or frail patients may be able to maintain a lower A1C safely if there are no issues with hypoglycemia, but others may need a higher A1C target to avoid the consequences of hypoglycemia.
Table 1.
Medication Recommendations for Geriatric Patients With Diabetes
After appropriate targets are determined, medication choices can be determined based on patients’ risk of hypoglycemia and concurrent medical conditions. Brief highlights related to the use of the major groups of antihyperglycemic agents in older patients are offered below. Information is given on the relative risk of hypoglycemia with each drug class. However, antihyperglycemic agents used in combination will have a higher risk of causing hypoglycemia even if the individual components of the combination therapy have a low risk of hypoglycemia when used as monotherapy.
Not all medications offer specific geriatric dosing guidance. Therefore, it may be prudent to start a medication at a lower dose—even one-half or one-fourth of the typical adult starting dose, if feasible. In many cases, it is not necessary in the outpatient setting to bring a chronic condition such as diabetes under control rapidly, and it may be beneficial to titrate more slowly to allow geriatric patients to become tolerant of the medication.37 This does not mean that patients should remain on their low starting dose; some older patients will ultimately be able to tolerate the same maintenance dose as younger people with diabetes if the dose is titrated slowly. Ongoing monitoring of adverse events and effectiveness is important to determine whether the dose should be increased. A motto that sums up these principles for geriatric dosing is “Start low, go slow, but still get somewhere.”37
Metformin
Metformin is considered the first-line treatment for type 2 diabetes in older patients because it is efficacious, inexpensive, and has a low risk of causing hypoglycemia.20,36,38 The most common side effects are gastrointestinal (GI) in nature and may be attenuated in older patients by using a more gradual dose titration schedule. Rather than the typical metformin starting dose of 500 mg twice daily, older patients and those who seem to have poor GI tolerability may benefit from a regimen that starts at 500 mg once daily, with dose titration every 2–4 weeks.39
The use of metformin extended release (XR) may help to reduce GI side effects in some people. However, a retrospective review found that metformin XR was linked to better GI tolerability in some patient cohorts, but not in all patients.40 Therefore, gradual dose titration may still be important for older adults even when using metformin XR.
Because of the expected aging-related decline in renal function, the possibility of metformin-induced lactic acidosis in older patients has been a concern. However, as the evidence base for this issue has expanded, more recent dosing guidance in the United States and internationally has focused on patients’ estimated glomerular filtration rate (GFR) rather than their serum creatinine level.41 No dosing changes are recommended until the estimated GFR is ≥ 30 and < 45 ml/min/1.73 m2, at which point one-half of the maximum dose is recommended.41 Stopping metformin is recommended when the estimated GFR is < 30 ml/min/1.73 m2.41 Use of these criteria may prevent unnecessary discontinuation of metformin in older people with diabetes who could benefit from it.
Sulfonylureas
Sulfonylureas long have been considered a first-line treatment for diabetes in older patients,36 but some guidelines have raised concerns about their association with an increased risk of hypoglycemia.20,38 Some drugs in the sulfonylurea class may pose less hypoglycemia risk than others, although evidence is contradictory. According to the Beers Criteria for potentially inappropriate medications in older adults, glyburide should be avoided in elderly patients because of its potential for prolonged hypoglycemia (related to its potentially extended half-life in older patients).8 Some sources consider glimepiride to pose less of a risk for hypoglycemia than glipizide.37 However, the U.S. Department of Veterans Affairs/Department of Defense guidelines36 state that glipizide causes less hypoglycemia.
All sulfonylureas are inexpensive and available generically, which may be an important benefit for older adults living on fixed incomes.
Meglitinides
The meglitinides (also called glinides) offer the advantage of flexible dosing for patients who have irregular eating patterns, including some older patients who may not eat three meals per day or follow a consistent meal schedule. Meglitinides may also cause less hypoglycemia than sulfonylureas when they are dosed correctly and only taken when patients eat a meal. However, these agents must be used with caution in patients who have renal impairment, and repaglinide must be used cautiously in those with hepatic impairment.20
Thiazolidinediones
Thiazolidinediones (TZDs) have a potential advantage in older adults because they have a low risk of causing hypoglycemia.36 However, they have been associated with several other issues that may be a problem for some older adults with diabetes. These include possible links to chronic heart failure, the development of fractures, and bladder cancer.42
Because of these concerns, TZDs are no longer recommended as a first-line treatment.20,38 When they are used, pioglitazone generally has been preferred over rosiglitazone because the U.S. Food and Drug Administration (FDA) had placed restrictions on the latter based on possible links to myocardial infarction (MI).43 However, in late November 2013, the FDA proposed easing some of these restrictions on rosiglitazone.
TZDs are comparatively expensive options, although a generic form of pioglitazone is now available.
Dipeptidyl peptidase-4 inhibitors
Dipeptidyl peptidase-4 (DPP-4) inhibitors are considered to be one of the first agents to use either along with or as an alternative to metformin because of their efficacy and low risk of hypoglycemia.36,38 Sitagliptin, saxagliptin, and alogliptin require dose adjustment for renal impairment but can still be given to people with renal disease.44–46 No renal adjustment is needed for linagliptin.47 These agents are not available generically and are expensive.
α-Glucosidase inhibitors
The α-glucosidase inhibitors (AGIs) are considered to have a low risk of hypoglycemia because they delay the absorption of carbohydrates. However, caution must be used if they are not discontinued with initiation of prandial insulin because AGIs could cause a delay in peak postprandial blood glucose levels in relation to the onset of action of prandial insulin doses.37
The most limiting side effects of these agents have been GI complaints. Although these agents are typically initiated with dosing three times daily, tolerability may be improved in older people by starting with once-daily dosing with the largest meal and adding a dose with an additional meal every 2 weeks.48 Because older patients may be more sensitive to GI upsets than the general population, monitoring is important. Renal impairment is also a concern, and AGIs are contraindicated when serum creatinine values are > 2.0 mg/dl.49,50
AGIs are moderately priced, and acarbose is available in a generic formulation.
Sodium-glucose co-transporter 2 inhibitors
Canagliflozin is the first available agent in the sodium-glucose co-transporter 2 (SGLT2) inhibitor class. These medications work by increasing renal glucose excretion and therefore are considered to have a low risk of causing hypoglycemia when used as monotherapy.
Canagliflozin has been studied specifically in older patients, including those ≥ 75 years of age.51 Compared to younger patients, those ≥ 65 years of age have been found to experience a higher rate of volume depletion, causing problems such as dizziness and orthostasis. These effects were more noticeable in those ≥ 75 years of age and were dose-dependent. Therefore, dose titration is important, and, in older patients, it may be best to initiate therapy with 100 mg daily and increase if needed and tolerated. Canagliflozin also has been found to have decreased benefit in older compared to younger patients.
Renal function must be considered because canagliflozin is ineffective in patients with a GFR < 30 ml/min/1.73 m2. Canagliflozin can cause hyperkalemia and therefore will require monitoring if given to patients who take diuretics or medications such as ACE inhibitors, which increase potassium levels. This is a particularly important consideration for many geriatric patients.51 Canagliflozin is also comparatively expensive.
Colesevelam
Colesevelam is a bile acid sequestrant that has a low risk of hypoglycemia when used as monotherapy and does not require any adjustments for elderly patients. However, it has potential for drug interactions by preventing absorption of some medications. This may be of particular concern for older people or those with multiple comorbidities who are more likely to take numerous medications.52
Colesevelam has been associated with esophageal obstruction, a potential issue for patients who have difficulty swallowing. It has a high pill burden (up to six tablets per day), which may be of concern for patients who take a large number of medications. It also can cause constipation and is not recommended for those with gastroparesis or other GI disturbances.52 This agent is not available generically and is expensive.
Bromocriptine
Bromocriptine is a dopamine agonist and one of the more recently approved agents for type 2 diabetes. Data on its use in geriatric patients are limited. However, bromocriptine is believed to reduce insulin resistance and therefore should have a low risk of causing hypoglycemia when used as monotherapy.
Dopamine agonists can cause orthostasis and sleep attacks, in which the patient suddenly falls asleep, and can interfere with the action of antipsychotic agents.53 Bromocriptine is moderately expensive.
Glucagon-like peptide-1 receptor agonists
Glucagon-like peptide-1 (GLP-1) receptor agonists are considered to be an effective and generally safe option for the treatment of type 2 diabetes. In general, these do not need special consideration in geriatric patients. Exenatide should not be used in people with a creatinine clearance <30 ml/min, and caution is recommended when increasing the dose from 5 to 10 μg in those with moderate renal impairment (30–50 ml/min).54Liraglutide does not require dosing adjustment for renal impairment. Worsening renal function has been reported with GLP-1 receptor agonists, but it is unclear whether these were responsible for the dysfunction because other medications affecting renal function or hydration often were also present.54,55.
Because these agents slow GI transit time, they are not recommended for people with gastroparesis or other GI motility disorders. It is also important to monitor patients for GI symptoms and weight loss, which can be significant.54,55
Because GLP-1 receptor agonists are injectable medications, due consideration must be given to ensure that patients can self-inject or receive injections from others appropriately. These agents are expensive.
Insulin
Insulin is the most effective treatment available for diabetes but also has substantial potential for causing hypoglycemia. Insulin will clearly be needed and can have substantial benefit in some older people with diabetes. However, the changes that occur with aging and the likely presence of additional comorbidities (e.g., problems with vision, cognition, and dexterity), may require further consideration to ensure that patients who use insulin can avoid potential harm. This does not mean insulin should be avoided in the elderly, but rather that clinicians should consider helpful options such as insulin pens, pre-drawn insulin, and direct assistance from a family member or caregiver for some of their older patients with diabetes.
Some insulins may have a lower risk of causing hypoglycemia. A pooled analysis of five randomized, controlled trials comparing the addition of NPH insulin or insulin glargine to oral agents found no difference between the treatments with regard to daytime symptomatic hypoglycemia or hypoglycemia severity.56 However, the glargine group had a lower incidence of both nocturnal symptomatic and nocturnal severe hypoglycemia.56 This study found no age-related differences with regard to hypoglycemia, but patients in the study were all ≤ 80 years of age.
A joint position statement of the International Association of Gerontology and Geriatrics, the European Diabetes Working Party for Older People, and the International Task Force of Experts in Diabetes 20 states that a regimen of basal insulin only may cause less hypoglycemia than basal-bolus or premixed insulin regimens. Sliding-scale insulin, in which the dose of insulin varies based on the blood glucose level, is not recommended by the Beers Criteria because such a dosing algorithm is more likely to cause hypoglycemia without improving glycemic control.8 The American Diabetes Association (ADA) position statement on the treatment of diabetes in older adults recommends against sliding-scale insulin as the sole treatment for glycemic control in inpatient and long-term care settings,2 and sliding-scale dosing may be even more problematic for patients who live in their own homes where insulin is not administered by a health care professional. Because sliding-scale doses are not consistent, this may be a particular issue for patients with vision, dexterity, or cognition problems.
Pramlintide
Pramlintide is indicated as an add-on therapy to insulin. No specific information is provided for its use in the elderly. However, pramlin-tide packaging information includes specific warnings that it could potentially increase the likelihood of insulin-induced hypoglycemia and that patients who use pramlintide should understand how to use insulin and check their blood glucose appropriately. Insulin doses should be reduced, usually by 50%, when pramlintide is initiated.57 Pramlintide is a very expensive option.
Aspirin
Aspirin treatment is still recommended for most older people with diabetes because of its clear benefit for secondary prevention of cardiovascular events, and it is also generally recommended for primary prevention in patients with both diabetes and other cardiovascular risk factors.2,58 However, as with other aspects of CVD in older people with diabetes, aspirin has not been well studied. A Japanese study59 of people with diabetes who had no history of CVD did not find benefit of aspirin for the general study cohort but did find a reduction in combined cardiovascular endpoints in a subgroup analysis of participants who were ≥ 65 years of age. In a population-based cohort study,60 taking ≤ 300 mg/day of aspirin was found to increase the risk of major bleeding (GI or cerebral hemorrhage) in the general population. However, aspirin did not cause a higher rate of bleeding in people with diabetes. Interestingly, these results may have been confounded by the fact that diabetes is an independent risk factor for increased bleeding. Thus, caution is still advised in using daily aspirin therapy for older people with diabetes.
The GI risk associated with aspirin treatment potentially can be prevented by the use of proton pump inhibitors or other gastroprotective agents.61 However, for older patients with diabetes who are at risk for other types of bleeding, clinicians must evaluate whether the risk of bleeding merits such treatment.
Joint professional guidance from the ADA, American Heart Association, and American College of Cardiology Foundation recommends aspirin at a dose of 75–162 mg daily.58
Treatment of Hypertension in Older Adults With Diabetes
Treating hypertension is important for preventing CVD, nephropathy, and retinopathy in older adults with diabetes.2,20,36 However, research has raised questions about whether some older patients—especially the oldest-old and those who are more frail—should have less intensive blood pressure targets than younger patients.
The ACCORD blood pressure trial (ACCORD-BP)62 compared systolic blood pressure targets of < 120 and < 140 mmHg and enrolled patients with a mean age of 62 years who had either CVD or cardiovascular risk factors. There was no benefit for the primary composite cardiovascular endpoint (nonfatal MI, nonfatal stroke, and death from cardiovascular causes) with more intensive blood pressure control. There was benefit for stroke reduction (number needed to treat: 89 for 5 years to prevent 1 stroke) but not for other secondary endpoints. Patients in the intensive group experienced some medication-related side effects at a significantly higher rate.
In the VADT to assess glycemic control and cardiovascular risk, patients (mean age 60 years) were given stepwise treatment to maintain blood pressure at a target of < 130/80 mmHg. A retrospective analysis indicated increased cardiovascular mortality at systolic blood pressure level > 140 mmHg but also at diastolic blood pressure levels < 70 mmHg.63 The diastolic result was in contrast to the ACCORD-BP results, in which the group with a systolic blood pressure target of <120 mmHg had a mean diastolic pressure of 64.4 mmHg and those in the group with a systolic blood pressure target of < 140 mmHg had a mean diastolic blood pressure of 70.5 mmHg, but mortality was not increased.62
Post-hoc analyses64,65 of two different trials treating patients with known coronary artery disease found that the relationship between blood pressure and mortality followed a J-shaped curve, in which mortality increased for both high and low blood pressure levels. Although evidence of a J-curve has been debated, the potential increased mortality at low blood pressure levels has been hypothesized to be related to poor perfusion of the heart and other organs. Poor perfusion may be a greater issue in older patients because of increasing arterial wall stiffness with aging.63
These data indicate a clear benefit to treating hypertension in older people with diabetes but also support the need to consider less aggressive targets, including a minimum blood pressure level, to avoid causing harm in some elderly patients. The VADT considered 105/70 mmHg to be the minimum blood pressure, but a true minimum would need to be confirmed in a randomized, controlled trial. One challenge in interpreting these findings is that isolated systolic hypertension occurs more commonly in the geriatric population. Therefore, weighing the benefit of lowering systolic blood pressure against the risk of excessively lowering diastolic blood pressure must occur on an individual basis when planning each patient’s therapy regimen.
Medications recommended for treating hypertension in older people with diabetes are the same as for younger patients. However, one consideration in older patients may be a possible link between hypoglycemia unawareness and β-blockers, given that many older patients already have a blunted response to sympathetic activation in the presence of hypoglycemia. β-Blockers are important for treating comorbidities such as heart failure or MI and therefore should not be withheld; however, avoiding hypoglycemia by setting less aggressive glucose and A1C targets may be prudent for older patients who are also taking a β-blocker.
Treatment of Hyperlipidemia in Older Adults With Diabetes
Lipid control also plays an important role in reducing CVD in people with diabetes. Statins are considered the primary hyperlipidemia treatment and have been shown to have significant clinical benefit over the course of just a few years.66 However, there has been controversy regarding the use of statins in the oldest segment of geriatric patients, because of both a dearth of data and recent evidence indicating potential harm in patients ≥ 80 years of age. A meta-analysis of 14 key statin trials67 indicated that statins offer a similar degree of cardiovascular risk reduction in patients > 75 years of age as in younger patients. However, the majority of the studies in this analysis (11 of 14) only enrolled patients ≤ 80 years of age.
Some trials have focused more specifically on geriatric patients. An analysis as part of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) examined treatment with pravastatin in older patients (aged ≥ 55 years; mean age 66 years) with moderate hypercholesterolemia and controlled hypertension. This study did not find a treatment benefit in terms of all-cause mortality or coronary heart disease, although the placebo group had a greater than expected benefit.68 The Prospective Study of Pravastatin in the Elderly at Risk (PROSPER) trial enrolled geriatric patients 70–82 years of age who were given pravastatin.69 This trial found a benefit of therapy in terms of heart disease but not for overall mortality or stroke.
Potentially more concerning than the mixed findings from these studies is the possibility of harm suggested in other analyses. A systematic review of statin trials70 found that the use of statins may increase overall mortality in patients ≥ 80 years of age.70 Another analysis from the Rotterdam study71 found an increasing inverse relationship between cholesterol levels and mortality with increasing age. This inverse relationship was found to begin at age 65. It has been hypothesized that the increased mortality observed in older patients may be related to statins lowering both smaller and larger LDL molecules. The larger and less dense LDL cholesterol molecules may have a protective benefit in aging.72 These studies do not mean that statins are contraindicated in older patients, although clinicians should evaluate whether a patient has known CVD or whether the issue is merely an elevated LDL level that is first detected in someone ≥ 80 years of age. It has been suggested72 that obtaining an analysis of the molecular structure of older patients’ LDL may be helpful to ensure that patients with small, dense LDL particles receive statin therapy, whereas those with primarily larger and potentially more beneficial LDL particles do not.72
General guidance on the use of statins in older people with diabetes is included in Table 1.
Conclusion
Diabetes is a significant concern requiring treatment in many older patients. However, patients with increasing age and comorbidities may have different needs than younger people with diabetes, and research indicates that less aggressive goal setting and more cautious use of medications may be prudent in this population. Clinicians should not interpret the need for such adjustments as an indication that diabetes treatment is not important in elderly patients. Rather, the treatment of diabetes in the elderly must be individualized to address specific age-related issues, keeping in mind the potential for greater harm and reduced benefits of standard diabetes therapies as patients age and develop more comorbidities.
References
- 1.Centers for Disease Control and Prevention : Diagnosed and undiagnosed diabetes in the United States, all ages, 2010. Available from http://www.cdc.gov/diabetes/pubs/estimates11.htm#1. Accessed 10 August 2013
- 2.Kirkman MS, Briscoe VJ, Clark N, Florez H, Haas LB, Halter JB, Huang ES, Korytkowski MT, Munshi MN, Odegard PS, Pratley RE, Swift CE: Diabetes in older adults. Diabetes Care 35:2650–2664, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lindeman RD, Tobin J, Shock NW: Longitudinal studies on the rate of decline in renal function with age. J Am Geriatr Soc 33:278–285, 1985 [DOI] [PubMed] [Google Scholar]
- 4.O’Malley K, Crooks J, Duke E, Stevenson H: Effect of age and sex on human drug metabolism. BMJ 3:607–609, 1971 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mangoni AA, Jackson SH: Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol 57:6–14, 2004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Turnheim K: Drug therapy in the elderly. Exp Gerentol 39:1731–1738, 2004 [DOI] [PubMed] [Google Scholar]
- 7.Greenblatt DJ, Harmatz JS, Shader RI: Clinical pharmacokinetics of anxiolytics and hypnotics in the elderly: therapeutic considerations (part I). Clin Pharmacokinet 21:165–177, 1991 [DOI] [PubMed] [Google Scholar]
- 8.American Geriatrics Society 2012 Beers Criteria Update Expert Panel: American Geriatrics Society updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 60:616–631, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Turnheim K: Drug dosage in the elderly: is it rational? Drugs Aging 13:357–379, 1998 [DOI] [PubMed] [Google Scholar]
- 10.White M, Roden R, Minobe W, Khan MF, Larrabee P, Wollmering M, Port JD, Anderson F, Campbell D, Feldman AM: Age-related changes in beta-adrenergic neuroeffector systems in the human heart. Circulation 90:1225–1238, 1994 [DOI] [PubMed] [Google Scholar]
- 11.Bremer JP, Jauch-Chara K, Halschmid M, Schmid S, Schultes B: Hypoglycemia unawareness in older compared with middle-aged patients with type 2 diabetes. Diabetes Care 32:1513–1517, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gregg EW, Mangione CM, Cauley JA, Thompson TJ, Schwartz AV, Ensrud KE, Nevitt MC; Study of Osteoporotic Fractures Research Group: Diabetes and incidence of functional disability in older women. Diabetes Care 25:61–67, 2002 [DOI] [PubMed] [Google Scholar]
- 13.Schwartz AV, Hillier TA, Sellmeyer DE, Resnick HE, Gregg E, Ensrud KE, Schreiner PJ, Margolis KL, Cauley JA, Nevitt MC, Black DM, Cummings SR: Older women with diabetes have a higher risk of falls: a prospective study. Diabetes Care 25:1749–1754, 2002 [DOI] [PubMed] [Google Scholar]
- 14.Bainbridge KE, Hoffman HJ, Cowie CC: Diabetes and hearing impairment in the United States: audiometric evidence from the National health and Nutrition Examination Survey, 1999 to 2004. Ann Intern Med 149:1–10, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bainbridge KE, Hoffman HJ, Cowie CC: Risk factors for hearing impairment among U.S. adults with diabetes: national Health and Nutrition Examination Survey 1999–2004. Diabetes Care 34:1540–1545, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cukierman T, Gerstein HC, Williamson JD: Cognitive decline and dementia in diabetes: systematic overview of prospective observational studies. Diabetologia 48:2460–2469, 2005 [DOI] [PubMed] [Google Scholar]
- 17.Whitmer RA, Karter AJ, Yaffe K, Quesenberry CP, Jr, Selby JV: Hypoglycemic episodes and risk of dementia in older patients with type 2 diabetes mellitus. JAMA 301:1565–1572, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Punthakee Z, Miller ME, Launer LJ, Williamson JD, Lazar RM, Cukierman-Yafee T, Seaquist ER, Ismail-Beigi F, Sullivan MD, Lovato LC, Bergenstal RM, Gerstein HC; ACCORD Group of Investigators; ACCORD-MIND Investigators: Poor cognitive function and risk of severe hypoglycemia in type 2 diabetes: post hoc epidemiologic analysis of the ACCORD trial. Diabetes Care 35:787–793, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lu FP, Lin KP, Kuo HK: Diabetes and the risk of multi-system aging phenotypes: a systematic review and meta-analysis. PLoS One 4:e1444, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sinclair A, Morley JE, Rodriguez-Mañas L, Paolisso G, Bayer T, Zeyfang A, Bourdel-Marchasson I,Vischer U, Woo J, Chapman I, Dunning T, Meneilly G, Rodriguez-Saldana J, Gutierrez Robledo LM, Cukierman-Yaffe T, Gadsby R, Schernthaner G, Lorig K: Diabetes mellitus in older people: position statement on behalf of the International Association of Gerontology and Geriatrics (IAGG), the European Diabetes Working Party for Older People (EDWPOP), and the International Task Force of Experts in Diabetes. J Am Med Dir Assoc 13:497–502, 2012 [DOI] [PubMed] [Google Scholar]
- 21.Huang ES, Zhang Q, Gandra N, Chin MH, Meltzer DO: The effect of comorbid illness and functional status on the expected benefits of intensive glucose control in older patients with type 2 diabetes: a decision analysis. Ann Intern Med 149:11–19, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Huang ES, Gorawara-Bhat R, Chin MH: Self-reported goals of older patients with type 2 diabetes mellitus. J Am Geriatr Soc 53:306–311, 2005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Laiteerapong N, Huang ES, Chin MH: Prioritization of care in adults with diabetes and comorbidity. Ann N Y Acad Sci 1243:69–87, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Centers for Medicare and Medicaid Services : More savings in the drug coverage gap coming through 2020. Available from http://www.medicare.gov/part-d/costs/coverage-gap/more-drug-savings-in-2020.html. Accessed 22 August 2013
- 25.Duckworth W, Abraira C, Moritz T, Reda D, Emanuele N, Reaven PD, Zieve FJ, Marks J, Davis SN, Hayward R, Warren SR, Goldman S, McCarren M, Vitek ME, Henderson WG, Huang GD; VADT Investigators: Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 360:129–139, 2009 [DOI] [PubMed] [Google Scholar]
- 26.ADVANCE Collaborative Group : Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 358:2560–2572, 2008 [DOI] [PubMed] [Google Scholar]
- 27.ACCORD Study Group : Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med 358:2545–2559, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Skyler JS, Bergenstal R, Bonow RO, Buse J, Deedwania P, Gale EA, Howard BV, Kirkman MS, Kosiborod M, Reaven P, Sherwin RS; American Diabetes Association; American College of Cardiology Foundation; American Heart Association: Intensive glycemic control and the prevention of cardiovascular events: implications of the ACCORD, ADVANCE, and VA diabetes trials: a position statement of the American Diabetes Association and a scientific statement of the American College of Cardiology Foundation and the American Heart Association. J Am Coll Cardiol 53:298–304, 2009 [DOI] [PubMed] [Google Scholar]
- 29.Currie CJ, Peters JR, Tynan A, Evans M, Heine RJ, Bracco OL, Zagar T, Poole CD: Survival as a function of HbA(1c) in people with type 2 diabetes: a retrospective cohort study. Lancet 375:481–489, 2010 [DOI] [PubMed] [Google Scholar]
- 30.Huang ES, Liu JY, Moffet HH, John PM, Karter AJ: Glycemic control, complications, and death in older diabetic patients: the Diabetes and Aging Study. Diabetes Care 34:1329–1336, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Greenfield S, Billimek J, Pellegrini F, Franciosi M, De Berardis G, Nicolucci A, Kaplan SH: Comorbidity affects the relationship between glycemic control and cardiovascular outcomes in diabetes: a cohort study. Ann Intern Med 151:854–860, 2009 [DOI] [PubMed] [Google Scholar]
- 32.Goto A, Arah OA, Goto M, Terauchi Y, Noda M: Severe hypoglycaemia and cardiovascular disease: systematic review and meta-analysis with bias analysis. BMJ 347:f4533, 2013. (doi: 10.1136/bmj.f4533) [DOI] [PubMed] [Google Scholar]
- 33.Centers for Disease Control and Prevention : Emergency department visit rates for hypoglycemia as first-listed diagnosis per 1,000 diabetic adults aged 18 years or older, by age, United States, 2006–2009. Available from http://www.cdc.gov/diabetes/statistics/hypoglycemia/fig5byage.htm. Accessed 25 July 2013
- 34.Budnitz DS, Lovegrove MC, Shehab N, Richards CL: Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med 365:2002–2012, 2011 [DOI] [PubMed] [Google Scholar]
- 35.Brown AF, Mangione CM, Saliba D, Sarkisian CA; California Healthcare Foundation/American Geriatrics Society Panel on Improving Care for Elders with Diabetes: Guidelines for improving the care of the older person with diabetes mellitus. J Am Geriatr Soc 51 (Suppl):S265–S280, 2003 [DOI] [PubMed] [Google Scholar]
- 36.U.S Department of Veterans Affairs : VA/DOD clinical practice guidelines: management of diabetes mellitus in primary care (2010). Available from www.healthquality.va.gov/Diabetes_Mellitus.asp. Accessed 12 August 2013
- 37.Neumiller JJ, Setter SM: Pharmacologic management of the older patient with type 2 diabetes mellitus. Am J Geriatr Pharmacother 7:324–342, 2009 [DOI] [PubMed] [Google Scholar]
- 38.Garber AJ, Abrahamson MJ, Barzilay JI, Blonde L, Bloomgarden ZT, Bush MA, Dagogo-Jack S, Davidson MB, Einhorn D, Garvey WT, Grunberger G, Handelsman Y, Hirsch IB, Jellinger PS, McGill JB, Mechanick JI, Rosenbilt PD, Umpierrez GE, Davidson MH: AACE comprehensive diabetes management algorithm. Endocr Pract 19:327–336, 2013 [DOI] [PubMed] [Google Scholar]
- 39.Setter SM, Iltz J, Thams J, Campbell RK: Metformin hydrochloride in the treatment of type 2 diabetes mellitus: a clinical review with a focus on dual therapy. Clin Ther 25:2991–3026, 2003 [DOI] [PubMed] [Google Scholar]
- 40.Blonde L, Daily GE, Jabbour SA, Reasner CA, Mills DJ: Gastrointestinal tolerability of extended-release metformin tablets compared to immediate-release metformin tablets: results of a retrospective cohort study. Curr Med Res Opin 20:565–572, 2004 [DOI] [PubMed] [Google Scholar]
- 41.Lipska KJ, Bailey CJ, Inzucchi SE: Use of metformin in the setting of mild-to-moderate renal insufficiency. Diabetes Care 34:1431–1437, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Pharmaceuticals Takeda. Actos package insert. Deerfield, Ill., Takeda Pharmaceuticals, 2012 [Google Scholar]
- 43.GlaxoSmithKline : Avandia package insert. Research Triangle Park, N.C, GlaxoSmithKline, 2011 [Google Scholar]
- 44.Merck : Januvia package insert. Whitehouse Station, N.J, Merck, 2013 [Google Scholar]
- 45.Bristol-Myers Squibb : Onglyza package insert. Princeton, N.J, Bristol-Myers Squibb, 2013 [Google Scholar]
- 46.Takeda Pharmaceuticals : Nesina package insert. Deerfield, Ill., Takeda Pharmaceuticals, 2013 [Google Scholar]
- 47.Boehringer Ingelheim : Tradjenta package insert. Ridgefield, Conn., Boehringer Ingelheim, 2013 [Google Scholar]
- 48.Campbell LK, Baker DE, Campbell RK: Miglitol: assessment of its role in the treatment of patients with diabetes mellitus. Ann Pharmacother 34:1291–1301, 2000 [DOI] [PubMed] [Google Scholar]
- 49.Pfizer : Glyset package insert. New York, Pfizer, 2009 [Google Scholar]
- 50.Bayer HealthCare Pharmaceuticals : Precose package insert. Wayne, N.J., Bayer HealthCare Pharmaceuticals, 2012 [Google Scholar]
- 51.Janssen Pharmaceuticals : Invokana package insert. Titusville, N.J., Janssen Pharmaceuticals, 2013 [Google Scholar]
- 52.Daiichi Sankyo : Welchol package insert. Parsippany, N.J., Daiichi Sankyo, 2012 [Google Scholar]
- 53.VeroScience : Cycloset package insert. Tiverton, R.I., VeroScience, 2010 [Google Scholar]
- 54.Bristol-Myers Squibb : Byetta package insert. Princeton, N.J., Bristol-Myers Squibb, 2013 [Google Scholar]
- 55.Novo Nordisk : Victoza package insert. Plainsboro, N.J., Novo Nordisk, 2013 [Google Scholar]
- 56.Lee P, Chang A, Blaum C, Vlajnic A, Gao L, Halter J: Comparison of safety and efficacy of insulin glargine and neutral protamine hagedorn insulin in older adults with type 2 diabetes mellitus: results from a pooled analysis. J Am Geriatr Soc 60:51–59, 2012 [DOI] [PubMed] [Google Scholar]
- 57.Amylin Pharmaceuticals : Symlin package insert. San Diego, Calif., Amylin Pharmaceuticals, 2008 [Google Scholar]
- 58.Pignone M, Alberts MJ, Colwell JA, Cushman M, Inzucchi SE, Mukherjee D, Rosenson RS, Williams CD, Wilson PW, Kirkman MS; American Diabetes Association; American Heart Association; American College of Cardiology Foundation: Aspirin for primary prevention of cardiovascular events in people with diabetes: a position statement of the American Diabetes Association, a scientific statement of the American Heart Association, and an expert consensus document of the American College of Cardiology Foundation. Diabetes Care 33:1395–1402, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Ogawa H, Nakayama M, Morimoto T, Uemura S, Kanauchi M, Doi N, Jinnouchi H, Sugiyama S, Saito Y; Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JAPD) Trial Investigators: Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. JAMA 300:2134–2141, 2008 [DOI] [PubMed] [Google Scholar]
- 60.De Berardis G, Lucisano G, D’Ettorre A, Pellegrini F, Lepore V, Tognoni G, Nicolucci A: Association of aspirin use with major bleeding in patients with and without diabetes. JAMA 307:2286–2294, 2012 [DOI] [PubMed] [Google Scholar]
- 61.Scheiman JM: Prevention of damage induced by aspirin in the GI tract. Best Pract Res Clin Gastroenterol 26:153–162, 2012 [DOI] [PubMed] [Google Scholar]
- 62.Cushman WC, Evans GW, Byington RP, Goff DC, Jr, Grimm RH, Jr, Cutler JA, Simons-Morton DG, Basile JN, Corson MA, Probstfield JL, Katz L, Peterson KA, Friedewald WT, Buse JB, Bigger JT, Gerstein HC, Ismail-Beigi F; ACCORD Study Group: Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 362:1575–1585, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Anderson RJ, Bahn GD, Moritz TE, Kaufman D, Abraira C, Duckworth W; VADT Study Group: Blood pressure and cardiovascular disease risk in the Veterans Affairs Diabetes Trial. Diabetes Care 34:34–38, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Messerli FH, Mancia G, Conti CR, Hewkin AC, Kupfer S, Champion A, Kolloch R, Benetos A, Pepine CJ: Dogma disputed: can aggressively lowering blood pressure in hypertensive patients with coronary artery disease be dangerous? Ann Intern Med 144:884–893, 2006 [DOI] [PubMed] [Google Scholar]
- 65.Bangalore S, Qin J, Sloan S, Murphy SA, Cannon CP; for the PROVE IT-TIMI 22 Trial Investigators: Relationship of blood pressure and cardiovascular events in the pravastatin or atorvastatin evaluation and infection therapy-thrombolysis in myocardial infarction (PROVE IT-TIMI) 22 trial. Circulation 122:2142–2151, 2010 [DOI] [PubMed] [Google Scholar]
- 66.Pyörälä K, Pedersen TR, Kjekshus J, Faergeman O, Olsson AG, Thorgeirsson G: Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease: a subgroup analysis of the Scandinavian Simvastatin Survival Study (4S). Diabetes Care 20:614–620, 1997 [DOI] [PubMed] [Google Scholar]
- 67.Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, Kirby A, Sourjina T, Peto R, Collins R, Simes R; Cholesterol Treatment Trialists’ (CTT) Collaborators: Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 366:1267–1278, 2005; errata Lancet 366:1358, 2005, and Lancet 371:2084, 2008 [DOI] [PubMed] [Google Scholar]
- 68.ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group : Major outcomes in moderately hypercholesterolemic, hypertensive patients randomized to pravastatin vs usual care: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT-LLT). JAMA 288:2998–3007, 2002 [DOI] [PubMed] [Google Scholar]
- 69.Shepherd J, Blauw GJ, Murphy MB, Bollen EL, Buckley BM, Cobbe SM, Ford I, Gaw A, Hyland M, Jukema JW, Kamper AM, Macfarlane PW, Meinders AE, Norrie J, Packard CJ, Perry IJ, Stott DJ, Sweeney BJ, Twomey C, Westendorp RG; for the PROSPER (PROspective Study of Pravastatin in the Elderly) Study Group: Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet 360:1623–1630, 2002 [DOI] [PubMed] [Google Scholar]
- 70.Petersen LK, Christensen K, Kragstrup J: Lipid-lowering treatment to the end? A review of observational studies and RCTs on cholesterol and mortality in 80+-year-olds. Age Ageing 39:674–680, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Newson RS, Felix JF, Heeringa J, Hofman A, Witteman JC, Tiemeier H: Association between serum cholesterol and noncardiovascular mortality in older age. J Am Geriatr Soc 59:1779–1785, 2011 [DOI] [PubMed] [Google Scholar]
- 72.Morley JE: The cholesterol conundrum. J Am Geriatr Soc 59:1955–1956, 2011 [DOI] [PubMed] [Google Scholar]