

Abstract
Cyprus maintains a population-based cancer registry that allows for in-depth study of cancer in a culturally- and environmentally-unique setting. Using eleven years of collected data (1998-2008), we present the first comprehensive analysis of cancer in Cyprus. We calculated gender-specific, world age-adjusted incidence rates and time trends for the 26 most incident cancers. This study revealed that overall world age-standardized rates among males increased from 195.4 cases per 100,000 in 1998-2002 to 239.0 cases per 100,000 in 2006-2008. For the entire eleven-year period, prostate, lung, colorectal, and bladder cancers were the most incident cancers among males. Among females, the overall world age-standardized rate increased from 180.6 cases per 100,000 in 1998-2002 to 217.1 cases per 100,000 in 2006-2008. Over the entire period, breast, colorectal, uterine, and thyroid were the most incident cancers in females. There were sixteen sex-specific cancers that indicated statistically significant increasing incidence trends over the study period, and no types for which the rate was significantly decreasing. Thyroid cancer illustrated rapid increases in rates. Results were compared to other Mediterranean European registries reported in Cancer Incidence in 5 Continents report for 1997-2002. Overall cancer incidence in Cyprus is lower than that of Southern Mediterranean countries, and given the known environmental risk factors in Cyprus, the low rate of lung cancer is especially interesting. The epidemiologic patterns reported in this study open the door for future etiologic studies to elucidate role of environmental and lifestyle factors of cancer in this population and highlight opportunities for cancer prevention and control.
Keywords: Cancer Incidence, Time Trends, Cyprus, Mediterranean, Registry-Based
Introduction
Over 12.6 million new cancer cases and 7.56 million cancer deaths were reported worldwide in 2008, with an estimated global prevalence of 585.8 cases per 100,000 adults 1. In light of the growing economic and healthcare burden of cancer, it is increasingly important for every nation to assess its own cancer incidence patterns. In the European Union (EU) alone, the European Cancer Observatory estimated that there were over 2.44 million new cancer cases and 1.23 million deaths in 2008. The incidence rate of cancer varies widely throughout the EU, with European age-standardized rates ranging from 523.9 in France to 265.8 in Cyprus (males) and 432.5 in Denmark to 199.2 in Greece (females)(rates per 100,000) 2.
Cyprus is a small island country situated in the eastern Mediterranean whose unique environmental and cultural history makes it an interesting setting to study cancer incidence. Cyprus has been a member of the Middle East Cancer Consortium (MECC) since 1998, and through that association, the Cyprus Ministry of Health (MOH) has overseen the development of an externally validated, population-based cancer registry.
To our knowledge, this is the first in-depth analysis of the Cyprus cancer registry data. Recently, Znaor et al. (2013) published a broad overview of the cancer burden in Southeast Europe which did include some data on Cyprus, but did not focus, on Cyprus and reported rates only for 2008 and for fewer cancer types 3. This study builds on the reports of short intervals by the MOH (reporting separate incidence figures for the years 1998-2000, 2003-2005, 2005-2007, and 2006 - 2008) 4,5. The aim of this study was to investigate the eleven-year (1998-2008) incidence rates and trends of cancer in Cyprus and compare them to those of other Mediterranean European countries that reported to IARC in the Cancer Incidence in 5 Continents report for the period 1997-2002 6.
Materials and Methods
Data Sources
The Cyprus Cancer Registry (CyCR) is a population-based cancer registry administered by the Cyprus MOH that was established in 1998 with support from MECC and the National Cancer Institute, USA. The CyCR covers the government-controlled southern part of the island of Cyprus, therefore our analysis does not include patients who are permanent residents of the area that is not under the effective control of the Government of the Republic of Cyprus (Figure 1). Using the classification system established by MECC, the CyCR uses ICD-O-3 to record information on 57 different cancer types, and the CANREG4 software, used for registration, derives the appropriate ICD-10 codes 5,7.
Figure 1.

Geopolitical map of Cyprus. The registry population is the southern part of the island labeled “Area Controlled by Cyprus Government”(CIA World Factbook).
We obtained the data for this study from the CyCR in datasets containing a randomized subject identifier (that was created and kept by the Health Monitoring Unit (HMU)), year of diagnosis, sex, and age at diagnosis. The best available estimates for the annual age- and sex-specific population sizes were obtained from the annual demographic reports published by the Statistical Service of Cyprus 8. Figure 2 displays the population pyramid for Cyprus during the eleven-year study period.
Figure 2.

Population pyramid for study period 1998-2008. The percentage of the total population falling into each of the seventeen age categories is indicated by a bar to the left for males and right for females.
Statistical Analysis
For each of the twenty-six most common cancer types in Cyprus, we calculated annual sex-specific, crude, and world age-standardized incidence rates. Age-specific incidence rates were calculated for each of six pooled age categories (0-29, 30-39, 40-49, 50-59, 60-69 and 70+) using the Doll world population as the standard 9. Patients with missing age data were excluded from the analysis. The eleven-year study period was subdivided into three shorter time periods (1998-2002, 2003-2005 and 2006-2008) to facilitate the investigation of incidence trends over time. The choice for this temporal division was due to 1) the period IARC data is available for international comparisons (roughly 1998 – 2002), 2) the entry of Cyprus in the EU in 2004 in order capture the larger wave of immigration and emigration that occurred around that time (2003-2005) and 3) the post-EU period (2006-2008).
Based on the derived incidence rates, we calculated sex-specific, age-adjusted annual percent change (APC) and 95% confidence intervals (CIs) of the incidence trends for the twenty-six cancer types investigated. The sex-specific APCs and their CIs were estimated based on poisson regression using year of diagnosis (continuous) and age group (categorical) as covariates and the age-specific count of incident cases as the outcome. Overdispersion was assessed using model diagnostics (such as AIC), and when existed, negative binomial regression was used as an alternative modeling strategy. When the data was sparse (there were a low number of incidence cases for a cancer type) our analysis involved collapsing the youngest age groups and creating ≤40 or ≤50 age groups, as needed. Analysis was performed using the PROC GENMOD procedure in SAS 9.3.
In order to assess how the calculated Cypriot rates compared internationally, we used data from the IARC Cancer Incidence in 5 Continents IX publication for Mediterranean countries that shared regional and lifestyle characteristics with Cyprus 10. We chose to make comparisons with Italy, Spain, France, Malta, and Turkey (selecting the regional registries geographically closest to Cyprus); we will hereafter call these countries the “EUROMED” region. Although Greece shares many characteristics with Cyprus, it was not included in the comparison since it does not have a national cancer registry and consequently has no data available in the IARC publication. We report incidence rates for 1997-2002 for these EUROMED regional registries for all cancer types combined and for the top ten cancer types in Cyprus.
Results
The CyCR recorded a total of 23,806 cases of cancer from 1998-2008, and we excluded 482 cases (2.02%) because of missing age data. These cases represent patients residing in the government-controlled part of Cyprus, for which we have more detailed information on the socioeconomic and environmental factors influencing the population. Cancer incidence in Cyprus could be affected by migration; over the 11-year period of our study a total of about 174,000 long-term immigrants were recorded to have come to Cyprus. However, it should be noted that the majority of these immigrants are of a younger age; 85% of these immigrants were less than 49 years old 11,12. The major countries showing migration to Cyprus include Greece, UK, Asia and after Cyprus joined the EU a wave of immigrants from Eastern European countries was recorded. Tables 1 and 2 display the incidence analysis, by sex, for the three time blocks of the study period (analysis of these cancer types for the entire eleven years can be found in supplemental tables 1 and 2). We analyzed a total of 12,309 male cases (11,970 of which had known age) and 11,497 female cases (11,354 of which had known age). The median age of cancer diagnosis was 68 years for males and 62 years for females. The overall world age-standardized cancer rate among males increased from 195.4 cases per 100,000 during 1998-2002 to 239.0 cases per 100,000 during 2006-2008. For the entire eleven- year period, prostate, lung, colorectal, and bladder were the most incident cancer types for males. Among females, the overall world age-standardized cancer rate started at 180.6 cases per 100,000 in 1998-2002, and increased to 217.1 cases per 100,000 in 2006-2008. Over the eleven-year period, breast, colorectal, uterine, and thyroid were the most incident cancer types in females. Breast cancer had the highest incidence of any cancer type for both sexes during all three time periods. The cancer type with the most marked increase in rates over the three time blocks was female thyroid cancer, which rose from a world age-standardized rate of 9.9 cases per 100,000 during 1998-2002 to 20.1 in 2006-2008, more than doubling in just eleven years. Breast and prostate cancer showed a sharp increase in incidence rates in the second period (2003 – 2005), and thyroid cancer showed the biggest increase in the third period (2006 – 2008). Interestingly, even though Cyprus was the main producer of chrysotile asbestos in Europe, the incidence rates of mesothelioma were very low with a world age-standardized rate of 0.45 and 0.25 cases per 100,000 during 1998-2002, 0.85 and 0.48 during 2003-2005, and 1.33 and 0.21 during 2006-2008 for males and females respectively.
Table 1.
Cases count, registry percent, annual crude and world age-standardized incidence rates for the top twenty-six cancer types for males in Cyprus 1998-2008
| 1998-2002 | 2003-2005 | 2006-2008 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Site | Count all ages | % Total | Crude rate | AWSR | Count all ages | % Total | Crude rate | AWSR | Count all ages | % Total | Crude rate | AWSR |
| Prostate | 1086 | 23.87 | 63.33 | 42.81 | 973 | 26.67 | 90.22 | 56.20 | 1060 | 25.78 | 92.83 | 58.01 |
| Tr., br., lung | 597 | 13.12 | 34.81 | 25.94 | 428 | 11.73 | 39.68 | 26.92 | 484 | 11.77 | 42.39 | 28.15 |
| Colon & rectum | 511 | 11.23 | 29.80 | 21.23 | 424 | 11.62 | 39.31 | 26.64 | 515 | 12.52 | 45.10 | 29.21 |
| Bladder | 433 | 9.52 | 25.25 | 15.93 | 303 | 8.31 | 28.09 | 14.26 | 362 | 8.80 | 31.70 | 16.05 |
| NHL | 204 | 4.48 | 11.90 | 9.66 | 184 | 5.04 | 17.06 | 13.12 | 155 | 3.77 | 13.57 | 9.79 |
| Leukemia | 201 | 4.42 | 11.72 | 9.45 | 145 | 3.97 | 13.44 | 10.21 | 172 | 4.18 | 15.06 | 11.15 |
| Stomach | 168 | 3.69 | 9.80 | 7.16 | 112 | 3.07 | 10.38 | 7.19 | 144 | 3.50 | 12.61 | 8.38 |
| Kidney | 122 | 2.68 | 7.11 | 5.47 | 84 | 2.30 | 7.79 | 5.40 | 76 | 1.85 | 6.66 | 4.77 |
| Pancreas | 99 | 2.18 | 5.77 | 4.17 | 80 | 2.19 | 7.42 | 5.02 | 84 | 2.04 | 7.36 | 5.11 |
| Brain & NS | 101 | 2.22 | 5.89 | 5.12 | 63 | 1.73 | 5.84 | 4.76 | 79 | 1.92 | 6.92 | 5.46 |
| Liver | 80 | 1.76 | 4.66 | 3.49 | 64 | 1.75 | 5.93 | 3.93 | 83 | 2.02 | 7.27 | 4.55 |
| Testis | 75 | 1.65 | 4.37 | 4.42 | 80 | 2.19 | 7.42 | 7.42 | 65 | 1.58 | 5.69 | 5.74 |
| Larynx | 72 | 1.58 | 4.20 | 3.20 | 49 | 1.34 | 4.54 | 3.23 | 75 | 1.82 | 6.57 | 4.75 |
| Melanoma of skin | 61 | 1.34 | 3.56 | 2.88 | 44 | 1.21 | 4.08 | 2.98 | 74 | 1.80 | 6.48 | 4.46 |
| Thyroid | 57 | 1.25 | 3.32 | 2.87 | 52 | 1.43 | 4.82 | 4.37 | 63 | 1.53 | 5.52 | 4.71 |
| Multiple myeloma | 54 | 1.19 | 3.15 | 2.36 | 60 | 1.64 | 5.56 | 3.45 | 61 | 1.48 | 5.34 | 3.33 |
| Hodgkin disease | 50 | 1.10 | 2.92 | 3.02 | 43 | 1.18 | 3.99 | 4.25 | 43 | 1.05 | 3.77 | 4.02 |
| Oral cavity | 47 | 1.03 | 2.74 | 2.20 | 43 | 1.18 | 3.99 | 2.75 | 47 | 1.14 | 4.12 | 2.99 |
| Connective soft tissue | 38 | 0.84 | 2.22 | 1.74 | 33 | 0.90 | 3.06 | 2.59 | 45 | 1.09 | 3.94 | 2.94 |
| Gallbladder | 46 | 1.01 | 2.68 | 1.70 | 31 | 0.85 | 2.87 | 1.76 | 31 | 0.75 | 2.71 | 1.62 |
| Bone | 29 | 0.64 | 1.69 | 1.72 | 16 | 0.44 | 1.48 | 1.45 | 15 | 0.36 | 1.31 | 1.39 |
| Other | 418 | 9.19 | 24.37 | 17.71 | 337 | 9.24 | 31.25 | 21.36 | 379 | 9.22 | 33.19 | 21.94 |
| All Types but skin | 4488 | 98.66 | 261.71 | 192.52 | 3604 | 98.79 | 334.17 | 228.23 | 4038 | 98.20 | 353.62 | 234.49 |
| All types | 4549 | 100.00 | 265.26 | 195.39 | 3648 | 100.00 | 338.25 | 231.20 | 4112 | 100.00 | 360.10 | 238.96 |
Table 2.
Cases count, registry percent, average annual crude and world age-standardized incidence rates for the top twenty-six cancer types for females in Cyprus 1998-2008
| 1998-2002 | 2003-2005 | 2006-2008 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Site | Count all ages | % Total | Crude rate | ASRW | Count all ages | % Total | Crude rate | ASRW | Count all ages | % Total | Crude rate | ASRW |
| Breast | 1497 | 34.28 | 84.32 | 64.06 | 1213 | 36.81 | 108.17 | 78.82 | 1311 | 34.19 | 110.23 | 77.72 |
| Colon & rectum | 456 | 10.44 | 25.69 | 16.77 | 342 | 10.38 | 30.50 | 18.85 | 440 | 11.47 | 37.00 | 22.32 |
| Uterus | 304 | 6.96 | 17.12 | 12.30 | 233 | 7.07 | 20.78 | 14.04 | 235 | 6.13 | 19.76 | 12.77 |
| Thyroid | 195 | 4.47 | 10.98 | 9.90 | 157 | 4.76 | 14.00 | 12.61 | 269 | 7.01 | 22.62 | 20.06 |
| NHL | 159 | 3.64 | 8.96 | 6.56 | 123 | 3.73 | 10.97 | 7.58 | 143 | 3.73 | 12.02 | 8.23 |
| Ovary | 189 | 4.33 | 10.65 | 8.01 | 99 | 3.00 | 8.83 | 6.57 | 132 | 3.44 | 11.10 | 7.36 |
| Tr., br., lung | 139 | 3.18 | 7.83 | 5.34 | 110 | 3.34 | 9.81 | 6.51 | 156 | 4.07 | 13.12 | 8.57 |
| Leukemia | 143 | 3.27 | 8.06 | 6.10 | 130 | 3.95 | 11.59 | 8.68 | 104 | 2.71 | 8.74 | 6.18 |
| Stomach | 119 | 2.72 | 6.70 | 4.58 | 55 | 1.67 | 4.90 | 3.28 | 91 | 2.37 | 7.65 | 4.43 |
| Cervix uteri | 104 | 2.38 | 5.86 | 4.35 | 69 | 2.09 | 6.15 | 4.46 | 80 | 2.09 | 6.73 | 4.76 |
| Brain, & NS | 91 | 2.08 | 5.13 | 4.47 | 50 | 1.52 | 4.46 | 3.20 | 80 | 2.09 | 6.73 | 4.66 |
| Melanoma of skin | 85 | 1.95 | 4.79 | 3.56 | 53 | 1.61 | 4.73 | 3.58 | 81 | 2.11 | 6.81 | 4.61 |
| Pancreas | 75 | 1.72 | 4.22 | 2.46 | 51 | 1.55 | 4.55 | 2.57 | 86 | 2.24 | 7.23 | 3.35 |
| Bladder | 84 | 1.92 | 4.73 | 3.08 | 65 | 1.97 | 5.80 | 2.96 | 65 | 1.69 | 5.47 | 3.33 |
| Multiple myeloma | 43 | 0.98 | 2.42 | 1.47 | 55 | 1.67 | 4.90 | 3.25 | 63 | 1.64 | 5.30 | 3.48 |
| Kidney | 67 | 1.53 | 3.77 | 2.93 | 41 | 1.24 | 3.66 | 2.27 | 43 | 1.12 | 3.62 | 2.51 |
| Hodgkin disease | 62 | 1.42 | 3.49 | 3.64 | 42 | 1.27 | 3.75 | 3.95 | 32 | 0.83 | 2.69 | 3.24 |
| Gallbladder | 68 | 1.56 | 3.83 | 2.41 | 33 | 1.00 | 2.94 | 1.62 | 35 | 0.91 | 2.94 | 1.53 |
| Connective, soft tissue | 41 | 0.94 | 2.31 | 1.93 | 36 | 1.09 | 3.21 | 2.55 | 33 | 0.86 | 2.77 | 2.19 |
| Liver | 35 | 0.80 | 1.97 | 1.21 | 26 | 0.79 | 2.32 | 1.32 | 39 | 1.02 | 3.28 | 1.65 |
| Oral cavity | 29 | 0.66 | 1.63 | 1.07 | 18 | 0.55 | 1.61 | 1.18 | 17 | 0.44 | 1.43 | 0.83 |
| Bone | 22 | 0.50 | 1.24 | 1.25 | 15 | 0.46 | 1.34 | 1.24 | 4 | 0.10 | 0.34 | 0.41 |
| Larynx | 8 | 0.18 | 0.45 | 0.32 | 6 | 0.18 | 0.54 | 0.36 | 5 | 0.13 | 0.42 | 0.27 |
| Other | 352 | 8.06 | 19.83 | 12.92 | 273 | 8.29 | 24.34 | 14.89 | 291 | 7.59 | 24.47 | 13.98 |
| All Types but skin | 4282 | 98.05 | 241.20 | 177.04 | 3242 | 98.39 | 289.10 | 201.95 | 3754 | 97.89 | 315.65 | 212.49 |
| All types | 4367 | 100.00 | 245.99 | 180.60 | 3295 | 100.00 | 293.83 | 205.53 | 3835 | 100.00 | 322.46 | 217.10 |
Tables 3 and 4 report the results of the incidence trend analysis, and figures 3 and 4 display the trends for the top five cancer types in men and women. For both males and females during the period 1998-2008, the annual rate of all types of cancer combined increases significantly at the alpha 0.05 level. Both males and females had similar APCs for all types combined with the values for males being slightly higher (5.94%) than for females (5.47%). Among males, ten cancer types displayed significantly increasing trends in incidence rate. The male cancer type with the highest significant APC was prostate cancer (9.2%). Among females, six cancer types displayed significantly increasing trends in incidence rate with multiple myeloma as the highest significant APC (11.94%). Female thyroid cancer had the second highest significant APC, increasing at a rate of more than ten percent annually (10.17%).
Table 3.
Eleven-Year World Age-Standardized Incident Trend Analysis
| Cancer Type | Male (APC, 95% CI) | Female (APC, 95% CI) |
|---|---|---|
| Breast | 2.85 (1.84,3.87)* | |
| Prostate | 9.20 (7.03,11.41)* | |
| Lung | 2.07 (0.44,3.73)* | 6.84 (3.51,10.27)* |
| Colorectal | 4.71 (2.97,6.47)* | 6.94 (4.78,9.14)* |
| Bladder | 2.37 (−1.63,6.53) | 2.09 (−2.27,6.64) |
| Stomach | 2.61 (−0.47,5.78) | −0.09 (−3.86,3.82) |
| Non-Hodgkin's lymphoma | 0.55 (−2.11,3.28) | 2.80 (−0.27,5.96) |
| Thyroid | 6.55 (1.50,11.85)* | 10.17 (7.36,13.06)* |
| Liver | 4.38 (1.30,8.82)* | 8.27 (1.49,15.5)*† |
| Uterus | 1.17 (−1.09,3.48) | |
| Leukemia | 3.39 (0.55,6.31)* | 1.21 (−2.03,4.56) |
| Brain | 0.61 (−3.32,4.70) | 1.70 (−2.46,6.05) |
| Pancreas | 2.80 (−1.10,6.85)† | 3.94 (−0.63,8.71)† |
| Kidney | −1.07 (−4.70,2.69) | −1.27 (−6.17,3.89) |
| Gallbladder | −1.11 (−6.93,5.07)† | −1.84 (−6.94,3.55)† |
| Ovary | 1.03 (−2.53,4.71) | |
| Melanoma of the skin | 8.31 (3.15,13.73)* | 3.62 (−0.72,8.15) |
| Multiple myeloma | 4.85 (−0.18,10.13)† | 11.94 (6.24,17.96)* |
| Hodgkin's lymphoma | 4.08 (−1.30,9.74) | −1.13 (−6.28,4.31) |
| Cervix | −0.21 (−4.09,3.82) | |
| Testis | 4.52 (0.19,9.04)* | |
| Connective, soft tissue | 6.33 (0.17,12.87)* | 2.36 (−3.52,8.58) |
| Larynx | 5.43 (0.74,10.34)* | −1.56 (−14.6,13.46)† |
| Bone | −5.59 (−12.87,2.30) | −6.99 (−15.63,2.53) |
| Oral cavity | 5.13 (−0.44,11.01) | −1.45 (−8.90,6.62) |
| All types | 5.94 (5.12, 6.77)* | 5.47 (4.56,6.40)* |
Statistically significant trend over time at the α=0.05 level
Estimate from Collapsed Age Group analysis
Table 4.
Comparison of Calculated Cypriot Incidence to Cancer Incidence in Five Continents results 1998-2002 from Other EuroMed Countries
| Registry | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Cancer Type | Sex | Spain, Girona (1998-2002) | Spain, Murcia (1997-2001) | France, Herault (1998-2002) | Italy, Salerno (1998-2001) | Italy, Sassari (1998-2002) | Malta (1998-2002) | Cyprus (1998-2002) | Turkey, Antalya (1998-2002) |
| Breast | Female | 66.5 | 57.3 | 95.1 | 59.1 | 73.9 | 67.7 | 64.1 | 29.1 |
| Prostate | Male | 57.5 | 38.5 | 82.7 | 23.8 | 34.5 | 35.1 | 42.8 | 19.1 |
| Lung | Male | 54.7 | 50.4 | 47.5 | 50 | 49.4 | 38.8 | 25.9 | 37.5 |
| Female | 5.4 | 4.8 | 10.5 | 6.1 | 8.2 | 6.1 | 5.3 | 4.8 | |
| Colon | Male | 28.6 | 23 | 23.2 | 19.4 | 20.6 | 15.1 | 14.2 | 7.6 |
| Female | 18.6 | 16.3 | 16.3 | 13.3 | 13.7 | 14.1 | 11.9 | 5.6 | |
| Rectal | Male | 15.5 | 15.5 | 14.7 | 8.8 | 11.4 | 12.5 | 7.3 | 5.3 |
| Female | 7.8 | 7.9 | 9.1 | 5.7 | 6.1 | 8.5 | 5.0 | 3.5 | |
| Bladder | Male | 35.8 | 37.6 | 15.7 | 37.8 | 28.7 | 26.8 | 15.9 | 15.8 |
| Female | 4.6 | 4.2 | 2.5 | 5 | 4.3 | 4.6 | 3.1 | 2.5 | |
| NHL | Male | 12.1 | 9.8 | 10.7 | 11.1 | 12.1 | 10.5 | 9.7 | 5.3 |
| Female | 9.3 | 7.3 | 7.8 | 8.9 | 8 | 7.6 | 6.6 | 3.9 | |
| Uterus | Female | 6.6 | 12.3 | 10.2 | 9.9 | 12.3 | 16.5 | 12.3 | 7.2 |
| Leukemia | Male | 7.7 | 9 | 9.1 | 10.3 | 11.2 | 10.3 | 14.9 | 5.9 |
| Female | 5.4 | 7.1 | 6 | 6.8 | 6.4 | 5.8 | 9.6 | 4.1 | |
| Stomach | Male | 12.4 | 11.9 | 7 | 10.8 | 9 | 10.9 | 7.2 | 10.6 |
| Female | 6.5 | 6 | 3.1 | 5.8 | 4.9 | 4.6 | 4.6 | 5.5 | |
| Thyroid | Male | 2.4 | 2.2 | 2.2 | 3.5 | 3.1 | 1.7 | 2.9 | 1.1 |
| Female | 6.5 | 7.4 | 7.3 | 12.4 | 12 | 9.4 | 9.9 | 4.5 | |
| All types | Male | 400.4 | 350.3 | 323.4 | 295.3 | 349.4 | 314.6 | 195.4 | 182.0 |
| Female | 252.4 | 218.9 | 236.7 | 218.4 | 251.9 | 249.9 | 180.6 | 125.8 | |
Figure 3.
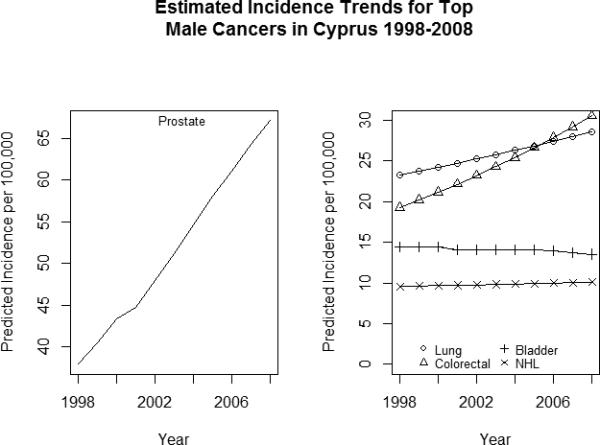
Plots of the model estimated annual age adjusted incidence rate of the top five cancer types for males during the study period. The plot on the left illustrates the trend in prostate cancer (separated due to its higher incidence rates). The plot on the right depicts the trend in lung, colorectal, bladder and non-Hodgkin's lymphoma which make up the remaining top five cancers.
Figure 4.

Plots of the model estimated annual age adjusted incidence rate of the top five cancer types for females during the study period. The plot on the left illustrates the trend in breast cancer (separated due to its higher incidence rates). The plot on the right depicts the trend in colorectal, uterine, thyroid and non-Hodgkin's lymphoma which make up the remaining top five cancers.
Table 4 displays world age-standardized cancer incidence rates per 100,000 people in the EUROMED region for 1997-2002. During that period, Cyprus has the lowest rate of male lung cancer for the entire region. The rates of Cypriot male and female stomach, leukemia, and thyroid, as well as prostate, uterine, female lung, and male bladder cancers were in line with the rates seen in the rest of the region. For male and female colon, rectal, Non-Hodgkin Lymphoma, overall cancer, and female bladder cancers, only the Turkish regional registry had rates lower than the Cypriot rates.
Discussion
This study showed that cancer in Cyprus exhibits a number of interesting incidence and trend patterns. First, of the twenty-six cancer types studied in men and women, there were sixteen sex-specific cancer sites which showed significantly increasing trends, and none that showed significantly decreasing trends during the study period. Second, a few cancers showed interesting patterns in our analysis. Prostate and breast cancers were the most common cancers in men and women, respectively. Male lung cancer rate was relatively low considering the high smoking rates among males in Cyprus, female thyroid cancer has increased significantly in the studied period, and colorectal cancer was the only cancer that was ranked in the top three most incident cancers for both males and females for the period 1998-2008. Third, Cypriots have a comparatively lower cancer rate than the populations in the EUROMED region, which share lifestyle similarities with Cyprus.
Through comparisons of the rates of the top ten cancer sites in men and women in Cyprus with rates in other countries in the EUROMED region, we found that the Cypriot population experiences a relatively low overall cancer rate. In general, Cyprus has either the lowest rate or a rate comparable with the lower end of the EUROMED region countries. It is unclear why cancer rates are lower in Cyprus compared to neighboring countries; however, there are a number of hypotheses that could be investigated. For example, considering the year-round sunny weather and a diet rich in seafood the population might be exposed to sufficient amounts of vitamin D. Vitamin D has been shown to be a cancer preventive factor13, 14, even though there is conflicting literature in the field 15. Interestingly, Israel, a neighboring country, has higher levels of overall cancer incidence and a documented high prevalence of vitamin D deficiency in the population 16 According to CI5, overall age standardized cancer incidence in Israel for 1998 – 2002 was 323.4 for men (1.7 times higher than Cypriot men for the same period) and 291.4 for women (1.6 times higher than Cypriot women). Another possible cancer protective factor in Cyprus could be related to the Mediterranean diet, which has been suggested to possibly reduce the risk of breast cancer in Cyprus 17.
When we consider the rate of cancer incidence increase among the top cancer types in Cyprus, the trend of thyroid cancer incidence seems to be most noteworthy. Thyroid cancer is higher in Cyprus than Spain and France, similar to Malta, and lower than Italy (these countries rank among the highest thyroid cancer rates in the world). There appears to be a higher incidence of thyroid cancer in the Eastern than Western Mediterranean, but this requires further research to confirm. A global trend of increase in thyroid cancer incidence has been observed, with one possible reason being over-diagnosis due to more frequent use of needle biopsies. Of course, one cannot exclude the impact of radiation on the thyroid cancer increase. The estimated trends among the top five cancer sites in Cyprus suggest that colorectal has surpassed lung cancer to become the second most incident cancer in males. There has been some evidence of a shift in the Cypriot diet away from the traditional Mediterranean diet, and perhaps the increase in colorectal cancer is due to this increase in dietary risk factors 18.
Breast and prostate cancer rates in Cyprus far outpace all other cancer incidence rates. Observed increases in the rates could possibly reflect the availability of a free mammography screening program for breast cancer (initiated in 2004 and extended nationwide in 2007; it is also interesting to note that Cyprus ranks as the 5th country among 31 countries with the highest number of mammography units per million women) and abundant use of PSA testing, both of which result in increased diagnosis 19. Interestingly, the largest increase in breast cancer incidence was within the second period (2003–2005), during which the national breast cancer screening program was initiated in 2004. As more time passes, it will be worthwhile to analyze the impact of the breast cancer screening program and PSA availability in Cyprus on breast and prostate cancer incidence and mortality.
There were no cancer sites for which significant decreases in the annual incidence rate during the study period were reported, and significant increasing trends were reported for sixteen sex-specific cancer sites. This suggests that Cyprus’ cancer burden will continue to increase in the future and additional policies for cancer management as well as prevention and control should be instituted. Our results are in agreement with the reports of the Cypriot Ministry of Health (MOH) and others 3,7 .
Environmental exposures play key roles in the development of many cancer types and Cyprus is affected by a unique spectrum of cancer risk factors. Until the late 1980s, Cyprus was the leading producer of chrysotile asbestos in Europe 20 Air quality needs to be improved; the country exposure levels exceed the allowable limits set by the new European Union regulations 21. In 2002-2003 the primary sources of the air pollution in government-controlled Cyprus were nitrogen oxides (11,677 tns/yr), sulfur dioxide (5,674 tns/yr), benzene (maximum daily average 8.4 μg/m3 in commercial areas), carbon monoxide (35,987 tns/yr), and ozone (maximum daily average 102.6 μg/m3 in mountains) 22. Another large source of air pollution is particulate matter in the form of dust – local or carried across the Mediterranean from North Africa. The dust carries soot, sulphate particles, metals, and inorganic salts, and a number of these particulate pollutants are carcinogenic 23.
Smoking is another environmental factor associated with the development of many cancer types. In Cyprus, the proportion of daily smokers is high relative to other European nations, especially among males 24. Based on health surveys conducted in 2003 and 2008, the proportion of daily male smokers has remained around 38%, while the proportion of daily female smokers has increased during the same period from 10.5% to 14.3% 25, 26. The oldest data available for smoking is from a survey conducted in 1989 which indicated a 43% smoking prevalence in men, suggesting smoking was already common in the 80s 27. Unfortunately, data on smoking in previous decades is lacking and therefore it is difficult to address the impact of smoking on cancer in Cyprus. It is possible that the tobacco-epidemic has not yet affected cancer incidence in Cyprus, and this will become more evident in the coming decades. However, the high levels of air pollution and the prevalence of smoking since the 80s at least make the low male lung cancer rate unusual. With regards to other known risk factors, studies have shown that Cypriots are only exposed to average levels of gamma radiation, radon gas, and water pollution 28-33. The results of this study reveal that although Cyprus has a number of known environmental risk factors, the cancer rates remain relatively low when compared to other countries in the EUROMED region.
The MOH proportionately assigns cases with missing age to an age group for rate calculation, while our analysis excluded those cases (2.02% of all cases) that led to a very slight underestimation of the true incidence rate. This analysis identified one source of possible systematic bias in the CyCR. Nearly half of the cases missing age data (214 of 482, 44.4%) were prostate or bladder cancer patients, and a majority of those cases were attributed to a small group of urologists. Over time, the data collection and case identification methods of the registry have evolved. In 2004, the CyCR incorporated data from the national death registry, and in 2007 it began using electronic medical records from the Bank of Cyprus Oncology Center in Nicosia to improve the registry's case finding capabilities. While the inclusion of DCO cases from the death registry did improve cases coverage, it introduced about 10% of cases annually from 2004 onwards that are currently DCO cases, representing 5.9% of all registry cases. Efforts to follow these patients are ongoing, and as the registry improves it is expected that the proportion of DCO cases will drop. An audit conducted by MECC in 1999 found that the CyCR attained 88% case coverage. The registry has since improved, and based on a 2008 case finding evaluation, the CyCR is estimated to attain 95% coverage of all cancer cases in government-controlled Cyprus 7. As the CyCR improves methods of data collection and physicians improve their diagnostic ability, it is possible that the large increases in the incidence rate of some cancers may be due to improved detection and not true incidence increases for certain cancers (e.g. thyroid cancer).
This publication represents the first in-depth published report on cancer incidence using the data from the Cyprus Cancer Registry during the years 1998-2008. Our results show that although there are many environmental risk factors for cancer, the Cypriot population enjoys relatively lower cancer rates compared to other countries in the EUROMED region. Sixteen sex-specific cancer types show significantly increasing incidence rates, with thyroid cancer in females increasing at a highly significant rate. Future cancer prevention and control research should focus on exploring the epidemiology of lung and thyroid cancers as well as elucidating the effect of breast and prostate screening in changing cancer incidence and mortality in this population.
Supplementary Material
Acknowledgments
The data used in this study was collected by the Health Monitoring Unit of the Ministry of Health of Cyprus. The ideas and opinions expressed herein are those of the authors. Endorsement of these ideas and opinions by the Ministry of Health of Cyprus is not intended nor should it be inferred. The authors would like to acknowledge Kate Watson from the University of Nebraska Medical Center for generating and generously supplying Figure 1 of the map of Cyprus.
Mary Cooter was supported in part by the Cancer Epidemiology Education in Special Populations (CEESP) Program of the University of Nebraska (R25 CA112383). The authors would like to acknowledge the University of Nicosia for the additional financial support of Mary Cooter during her field work in Cyprus. In addition, the authors would like to acknowledge all staff members of the Cyprus Cancer Registry and the Statistical Service of Cyprus for their help and support.
Sources of support
Mary Cooter was supported in part by the Cancer Epidemiology Education in Special Populations (CEESP) Program of the University of Nebraska (R25 CA112383). In addition, Mary Cooter received financial support from the University of Nicosia during her field work in Cyprus.
Footnotes
Conflict of interest statement: The authors declare no conflict of interest.
References
- 1.Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. GLOBOCAN 2008 v2.0, Cancer incidence and mortality worldwide: IARC CancerBase No. 10. International Agency for Research on Cancer. 2010 [Google Scholar]
- 2.Ferlay J, Parkin DM, Steliarova-Foucher E. Estimates of cancer incidence and mortality in Europe in 2008. Eur J Cancer. 2010;46(4):765–781. doi: 10.1016/j.ejca.2009.12.014. [DOI] [PubMed] [Google Scholar]
- 3.Znaor A, van den Hurk C, Primic-Zakelj M, Agius D, Coza D, Demetriou A Dimitrova N, Eser S, Karakilinc H, Zivkovic S, Bray F, Coebergh JW. Cancer incidence and mortality patterns in South Eastern Europe in the last decade: gaps persist compared with the rest of Europe. Eur J Cancer. 2013;49:1683–1691. doi: 10.1016/j.ejca.2012.11.030. [DOI] [PubMed] [Google Scholar]
- 4.Freedman LS, Edwards BK, Ries LAG, Young JL, editors. Cancer incidence in four member countries (Cyprus, Egypt, Israel, and Jordan) of the middle east cancer consortium (MECC) compared with US SEER. National Cancer Institute; 2006. [Google Scholar]
- 5.Republic of Cyprus Ministry of Health . Cyprus cancer registry (CyCR) report for the triennial 1998-2000. Cyprus Cancer Registry; [Google Scholar]
- 6.Ferlay J, Parkin DM, Curado MP, Bray F, Edwards B, Shin HR. Cancer incidence in five continents, volumes I to IX: IARC CancerBase no.9. International Agency for Research on Cancer. 2010 [Google Scholar]
- 7.Republic of Cyprus Ministry of Health . MECC joint registration project Cyprus cancer registry (CyCR) report for 2008-2009 (Data 2003-2005) Cyprus Cancer Registry; 2009. [Google Scholar]
- 8.Republic of Cyprus Statistical Service: Demographic report 2010. Printing Office of the Republic of Cyprus; 2012. [Google Scholar]
- 9.Doll R, Payne P, Waterhouse J, editors. Cancer incidence in five continents: A technical report. Springer-Verlag (for UICC); 1966. [Google Scholar]
- 10.Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, Boyle P, editors. Cancer incidence in five continents. IX. IARC Scientific Publications; 2007. [Google Scholar]
- 11.Republic of Cyprus Statistical Service . Demographic report 2003. Printing Office of the Republic of Cyprus; 2004. [Google Scholar]
- 12.Republic of Cyprus Statistical Service . Demographic report 2009. Printing Office of the Republic of Cyprus; 2011. [Google Scholar]
- 13.Bulathsinghala Pubudu, Kostas N, Syrigos, Saif Muhammad W. Role of vitamin D in the prevention of pancreatic cancer. Journal of Nutrition and Metabolism. 2010;2010:721365–9. doi: 10.1155/2010/721365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lappe JM, Travers-Gustafson D, Davies KM, Recker RR, Heaney RP. Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am J Clin Nutr. 2007;85:1586–1591. doi: 10.1093/ajcn/85.6.1586. [DOI] [PubMed] [Google Scholar]
- 15.Sperati F, Vici P, Maugeri-Sacca M, Stranges S, Santesso N, Giordano Mariani L, Antonio Sergi, Domenico Pizzuti, Laura Di Lauro, Luigi Montella, Maurizio Crispo, Anna Mottolese, Marcella Barba, Maddalena Vitamin D supplementation and breast cancer prevention: a systematic review and meta-analysis of randomized clinical trials. PLoS One. 2013;8:e69269. doi: 10.1371/journal.pone.0069269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Steinvil A, Leshem-Rubinow E, Berliner S, Justo D, Finn T, Ish-shalom M, Birati Edo Y, Shalev Varda, Sheinberg Bracha, Rogowski Ori. Vitamin D deficiency prevalence and cardiovascular risk in Israel. Eur J Clin Invest. 2011;41:263–268. doi: 10.1111/j.1365-2362.2010.02403.x. [DOI] [PubMed] [Google Scholar]
- 17.Demetriou CA, Hadjisavvas A, Loizidou MA, Loucaides G, Neophytou I, Sieri S, Kakouri Eleni, Middleton Nicos, Vineis Paolo, Kyriacou Kyriacos. The Mediterranean dietary pattern and breast cancer risk in Greek-Cypriot women: A case-control study. BMC Cancer. 2012;12:113. doi: 10.1186/1471-2407-12-113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lazarou Chrystalleni, Panagiotakos Demosthenes B. Antonia-Leda Matalas: Level of adherence to the Mediterranean diet among children from Cyprus: the CYKIDS study. Public Health Nutrition. 2009;12(7):991–1000. doi: 10.1017/S1368980008003431. [DOI] [PubMed] [Google Scholar]
- 19.Cyprus Ministry of Health Activities in breast cancer screening in Cyprus. 2008 [Google Scholar]
- 20.Peacock P, Droussiotis A. [21 June, 2012];Mines of Cyprus. 2009 ( shropshiremines.org.uk/cyprus/amiandos/amiandos.htm.)
- 21.Cyprus Department of Labour Inspection Air quality in Cyprus: Air Pollution. 2012 [Google Scholar]
- 22.Baumbach Günter, Pfeiffer Heiko. Preliminary assessment of ambient air quality in Cyprus. Cyprus Department of Labour Inspection; 2004. [Google Scholar]
- 23.Cyprus Department of Labour Inspection Air quality statistics in Cyprus. 2012 [Google Scholar]
- 24.Eurostat Public Health Database European health interview survey-collection round 2008: Determinants of Health. European Commission [Google Scholar]
- 25.Republic of Cyprus Statistical Service . Health survey 2003. Printing Office of the Republic of Cyprus; 2005. [Google Scholar]
- 26.Republic of Cyprus Statistical Service . European health survey 2008. Printing Office of the Republic of Cyprus; 2010. [Google Scholar]
- 27.Department of Statistics and Research, Ministry of Finance, Republic of Cyprus . Printing Office of the Republic of Cyprus; 1991. Smoking in Cyprus 1989. [Google Scholar]
- 28.Anastasiou T, Tsertos H, Christofides S, Christodoulides G. Indoor radon (222Rn) concentration measurements in Cyprus using high-sensitivity portable detectors. Journal of Environmental Radioactivity. 2003;68(2):159. doi: 10.1016/S0265-931X(03)00052-3. [DOI] [PubMed] [Google Scholar]
- 29.Fatta D, St Canna-Michaelidou C, Michael E, Demetriou Georgiou M, Christodoulidou A, Achilleos M. Vasquez. Organochlorine and organophosphoric insecticides, herbicides and heavy metals residue in industrial wastewaters in Cyprus. Journal of Hazardous Materials. 2007;145:169. doi: 10.1016/j.jhazmat.2006.11.009. [DOI] [PubMed] [Google Scholar]
- 30.Fatta D, Michael C, St Canna-Michaelidou M, Christodoulidou N, Kythreotou M. Vasquez. Pesticides, volatile and semivolatile organic compounds in the inland surface waters of Cyprus. Desalination. 2007;215:223. [Google Scholar]
- 31.Nikolopoulos Dimitrios, Louizi Anna. Study of indoor radon and radon in drinking water in Greece and Cyprus: implications to exposure and dose. Radiation Measurements. 2008;43(7):1305. [Google Scholar]
- 32.Sarrou I, Pashalidis I. Radon levels in Cyprus. Journal of Environmental Radioactivity. 2003;68(3):269. doi: 10.1016/S0265-931X(03)00066-3. [DOI] [PubMed] [Google Scholar]
- 33.Svoukis E, Tsertos H. February indoor and outdoor in situ high-resolution gamma radiation measurements in urban areas of Cyprus. Radiation Protection Dosimetry. 2007;123(3):384–390. doi: 10.1093/rpd/ncl159. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.