

Abstract
Background:
Patients with chronic postural headaches may suffer from spontaneous intracranial hypotension (SIH). Trauma, degenerative disc spurring and connective tissue disorders are documented risk factors; in most cases there is no inciting event. Despite sophisticated means of evaluating the neuraxis, many cerebrospinal fluid (CSF) leaks are radiographically occult and treatment is focused on thoracic and cervical-thoracic regions. Although lumbar epidural blood patch (EBP) is the initial treatment of choice after failed conservative management, several studies document the need for treatment aimed at the specific leak area.
Case Description:
This report describes the case of a 42-year-old female with scleroderma and sudden onset postural headaches. Magnetic resonance imaging revealed diffuse pachymeningeal enhancement suggestive of intracranial hypotension. Computed tomographic myelography demonstrated a collection of fluid ventral to the cervical thecal sac; an exact location for CSF egress was not identified. Conservative measures followed by lumbar EBP failed to alleviate her symptoms. The patient underwent placement of a lumbar drain and dynamic radionuclide cisternography (RIC). Panoramic images of the spine were taken at the time of the pressurized saline injection. The CSF leak was clearly visualized at C1–2. Treatment was focused at this region using percutaneous injection of autologous blood and fibrin glue.
Conclusion:
SIH is disabling if left untreated. Spinal CSF leaks are often discrete and difficult to identify using static imaging. The use of pressurized, RIC by lumbar drain injection allows for the real-time evaluation of CSF dynamics and can more precisely identify slow flow leaks often missed with static imaging.
Keywords: Epidural blood patch, percutaneous, radionuclide cisternography, spontaneous cerebrospinal fluid leak, spontaneous intracranial hypotension
INTRODUCTION
Background and importance
Spontaneous intracranial hypotension (SIH) typically results from a spontaneous cerebrospinal fluid (CSF) leak,[17,21] most common in the thoracic or cervical-thoracic regions. Descent of the brain due to CSF hypovolemia causes tension on pain sensitive structures such as the meninges and blood vessels, leading to headaches that initially improve with recumbence. Mechanical factors combined with an underlying structural dural disorder cause the primary spontaneous spinal CSF leak.[20,21,24,28,30] SIH, including its various clinical presentations as well as pathophysiological mechanisms, has been well documented in the literature.[14,25,26,27,28] Despite our understanding of the disease and the advanced imaging modalities available to evaluate the cranial-spinal axis, often a structural lesion is not identified and small or radiographically occult tears in the dura or nerve sleeves are considered responsible.[24] Most studies that have examined the utility of the different imaging modalities-magnetic resonance imaging (MRI) or computed tomographic myelography (CTM), digital subtraction myelography (DSM) or radionuclide cisternography (RIC)-acknowledge that in a subset of patients the CSF leak flow pattern falls below the resolution of standard imaging.[5,9,10,15,23,32,35] In this population of patients standard imaging misses slow flow, intermittent CSF leaks that can be identified using pressurized, dynamic RIC.
Clinical presentation
Presentation and examination
This patient is a 42-year-old Caucasian female with a history of scleroderma who presented with sudden onset holocranial headache associated with nausea, vomiting, and photophobia, improving with recumbence. The onset of symptoms was unprovoked. The patient denied recent trauma, lumbar puncture or history of headaches. Physical examination revealed a nontoxic-appearing female with stable hemodynamic parameters; who was neurologically intact. The patient had no obvious physical manifestations of scleroderma, and home medications were geared toward symptom management.
Neuro-diagnostics
Noncontrast CT and CT angiography were negative for intracranial hemorrhage, mass or vascular lesion. An attempt was made by the emergency room physician to obtain a lumbar puncture. However, the procedure was aborted as CSF pressures were sub-atmospheric and a fluid sample could not be obtained. The patient was admitted for bed rest and intravenous fluid hydration with the presumptive diagnosis of SIH.
The patient was further assessed with an MRI of the brain with gadolinium. Diffuse smooth pachymeningeal enhancement over the cerebral convexities was consistent with meningeal hyperemia and intracranial hypotension[28] [Figure 1]. Twice, the patient underwent lumbar epidural blood patch (EBP), followed by bed rest and continued hydration. The patient experienced transient symptom relief, but the postural headaches recurred with 2 weeks.
Figure 1.
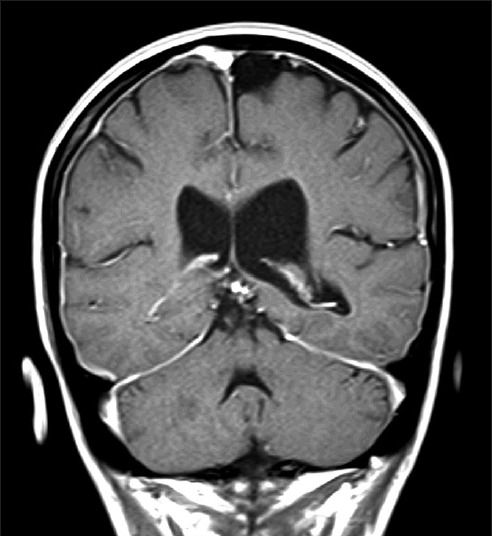
Sagittal magnetic resonance imaging of the brain with gadolinium demonstrates diffuse, smooth enhancement of the pachymeninges suggestive of meningeal hyperemia and intracranial hypotension
Diagnostic intervention
Efforts were then focused at identifying the source of the leak, as lumbar EBP had proved unsuccessful. CTM of the entire spinal axis demonstrated a subtly enhancing epidural fluid collection anterior to the cervical spinal cord [Figure 2]. However, the exact location of the CSF leak was not defined. The working hypothesis was that this might be attributable to an intermittent, slow flow dural rent with pressure too low to be observed with static imaging. To mitigate this problem, a lumbar drain was placed at L4–5 under fluoroscopy for the purpose of controlled dynamic imaging.
Figure 2.
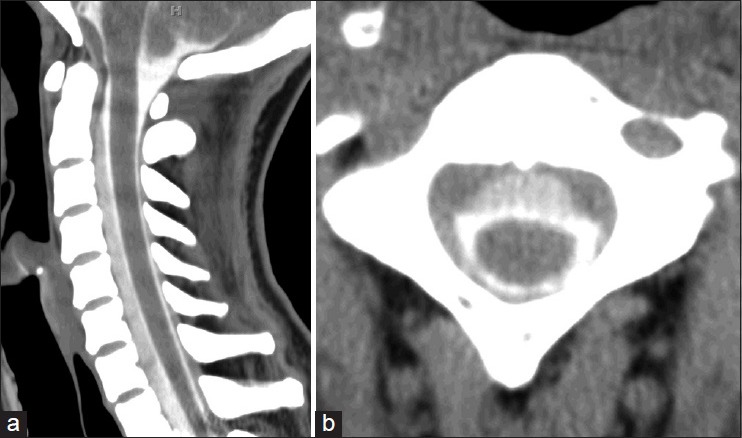
Computed tomography (CT) of the cervical spine following intrathecal administration of contrast. (a) Sagittal and (b) axial CT demonstrates contrast anterior to the cervical thecal sac. This collection is attenuated in comparison to the intra-dural contrast. The presence of this ventral epidural fluid collection suggests cerebrospinal fluid-contrast egress
The patient was then brought to nuclear medicine for injection of radiotracer via the lumbar drain. The patient was placed in the left lateral position and two cubic centimeters (cc) of indium-111-diethyl-enetriamine penta-acetic acid radiotracer was administered via lumbar drain. Immediate postinjection static images revealed a photopenic region in the mid-cervical spine likely attributable to the extradural fluid accumulation seen on CTM [Figure 3]. Extravasation of radiotracer was not demonstrated. Following this observation, 20-cc of sterile saline were pushed through the lumbar drain by the attending neurosurgeon. Dynamic images were taken at the same time as the saline push. Extravasation of radiotracer was seen dorsally at C1–2 [Figure 4].
Figure 3.

Static nuclear medicine cerebrospinal cisternography following injection of indium-111-diethyl-enetriamine-penta-acetic acid. (a) Right and (b) left lateral initial static images as well as (c) 5 min delayed images were obtained following administration of radiotracer. No evidence of abnormal accumulation of radioisotope is seen with initial or delayed injections. A photopenic region is demonstrated in the mid-cervical spine suggesting extrinsic pressure on the cervical subarachnoid space and corresponding to the epidural fluid collection seen on computed tomography myelography
Figure 4.
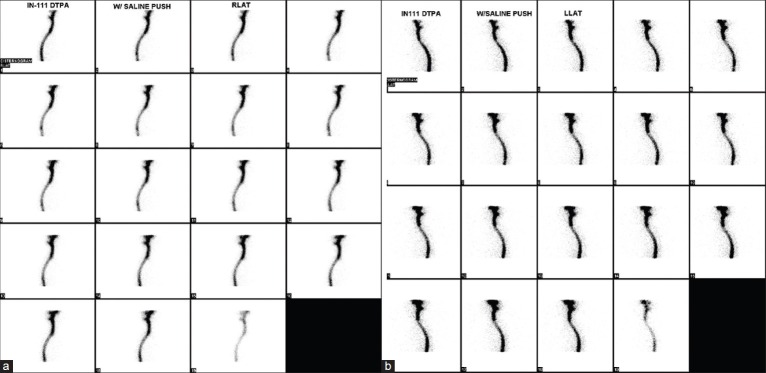
Dynamic nuclear medicine cerebrospinal cisternography following pressurized injection of saline through the lumbar drain. (a) Right and (b) left lateral views are obtained at the time of pressurized saline injection. Evidence of an abnormal accumulation of radioisotope is seen dorsally at C1-2 on both views
Surgical intervention
The patient was referred to the pain clinic for definitive treatment achieved by percutaneous, targeted epidural blood and fibrin patch. Postprocedure, the patient was kept on bed rest for 48 h, followed by a progression of activity as tolerated. She was discharged home on postoperative day six without headache.
DISCUSSION
Spontaneous CSF leaks can result from an abnormality in the cranial or spinal dura. Unlike those in the cranial dura in which patients present with otorrhea or rhinorrhea, spinal CSF leaks generally do not cause any local symptoms and remain undetected unless the diagnosis is actively pursued in a patient suspected of SIH.[28,29] One-third of patients with SIH will have a history of trivial trauma,[30] while two-thirds will have intrinsic dural weakness from an underlying connective tissue disorder.[17,21,22] Occasionally a dural tear from a spondolytic spur may lead to a CSF leak.[34]
Spontaneous intracranial hypotension secondary to CSF hypovolemia is primarily a self-limited condition; most patients will improve with conservative management.[17,28,35] It is pertinent to neurosurgical practice because if the diagnosis is missed and treatment delayed, patients may suffer from a considerably compromised quality of life. Patients often seek specialty care, including pain management, and may undergo unnecessary surgery for secondary manifestations of the disease, such as sub-occipital craniotomy for pseudo - Type 1 Chiari Malformation or evacuation of subdural hematoma.[17,24] It is important to understand risk factors and symptoms for SIH in order to obtain appropriate imaging and identify these patients to avoid delays in care. Otherwise, chronic pain and disability ensue with the potential for more serious neurological sequelae such as cranial nerve palsy, cerebellar dysfunction, and even coma.[4,6,19,25]
The diagnosis of spontaneous CSF leak can be obtained by lumbar puncture with evidence of low CSF pressure. Variable readings, including pressures within the normal range, may be obtained if the CSF leak is intermittent.[1,23,24] Cranial MRI with gadolinium and CTM[24,28] have been described as the initial studies of choice for diagnosing SIH. Characteristic findings of SIH by MRI include diffuse smooth pachymeningeal enhancement from meningeal venous hyperemia.[7,17,24] CTM is mostly utilized for demonstrating the actual site of CSF leak or an extradural fluid collection, but limitations in CSF flow dynamics through the leak can limit its utility.
Radionuclide cisternography is also used to identify radioactivity outside the dural sac.[1,11,17,35] However, as is seen with CTM, if there is no active flow of CSF at the time of the study the ability to identify the leak is limited.[5,15,32] Therefore, the possibility of locating a dural fistula or rent is reduced if the leakage is intermittent[15] or is so slow the tracer does not egress from the subarachnoid space by the time the imaging is completed. Several published studies attempt to rectify this limitation for cranial CSF leaks. Curnes et al. employed the use of controlled, pressurized RIC for the localization of CSF rhinorrhea with good result.[5] Magnaes and Solheim demonstrated improved localization of CSF rhinorrhea by adapting infusion cisternography.[15] However, the use of infusion or pressurized cisternography is limited for evaluation of spinal CSF leaks. One study employed the use of digital subtraction myelography (DSM) as a means of localizing spinal CSF leaks.[9] In this retrospective study by Hoxworth et al., patients with extradural fluid collections by CTM or spinal MRI with an ill-defined location of dural breach were subjected to localized DSM with contrast injection by lumbar drain. Of the patients meeting inclusion criteria, 18% (2 of 11 patients) of leaks were not identified presumably because the CSF leaks were too slow to be readily visualized during the brief 20–30 s DSM acquisition.[9] The authors posit that this technique is useful for identifying rapid CSF leaks when dynamic CTM was insufficient to identify the precise location due to rapid egress of dye from the subarachnoid space.[9] However, the challenge of identification of cryptic or intermittent CSF leaks[8,13] in patients suspicious for SIH remains. Our case offers a possible solution for this problem.
The case presented here provides an alternative for addressing CSF leaks in which the flow characteristics are slow or intermittent, and thus below the resolution of study for “standard static imaging.” The authors modify the use of an already widely accepted form of neuroimaging for SIH (i.e., RIC) in order to identify cryptic CSF leaks.
The use of pressurized RIC to identify the precise location of the CSF leak offers some notable diagnostic advantages to practitioners that may encounter this entity. First, it allows the clinician to obtain a panoramic view[35] of the spine in real-time. Also, the use of the lumbar drain allows for optimal positioning of the patient without compromising intrathecal access; which is more tedious with the Tuohy needle. Furthermore, once the radiotracer is injected, the lumbar drain allows the surgeon to perform a controlled “saline push” which serves to pressurize the CSF leak. RIC then becomes a dynamic study as the gamma camera provides real-time images of the flow of radiotracer throughout the spinal axis at the time of the saline push.
Historically, RIC has been used as a means of confirming SIH when the accumulation of radioactivity is noted outside the subarachnoid space. Its utility was first applied in the setting of SIH when early accumulation of radiotracer in the urinary bladder and kidneys suggested extravasation of intrathecal tracer with reabsorption via the epidural venous plexus.[1,18] Two issues overcome by the technique employed, in this case, include the lack of sensitivity of RIC in smaller, slower leaks and the lack of spatial detail that precludes direct localization of the CSF leak in many cases.[11,16,17] This case illustrates that the use of a pressurized injection via lumbar drain with dynamic cisternography can circumvent these limitations. Extravasation of radiotracer is seen in real-time and the panoramic view of the spine allows for localization of the dural breach.
Increasing support for targeted treatment in SIH is found in the literature, especially when initial lumbar epidural blood patching fails to resolve symptoms. Defining the CSF leak as secondary to dural rent or meningeal diverticulum, allows choice of the most appropriate management, whether by targeted percutaneous blood patch or open surgical treatment. EBP is the treatment of choice in patients who have failed an initial trial of conservative management.[3,31] EBPs have been shown to spread within the epidural space over many spinal levels,[3,30,33] which argues the necessity of finding the precise level of dural rent when percutaneous treatment measures are used. Failure of EBP therapy or recurrence after initial success seems to be common in patients with a cervical CSF leak. Recently, “targeted” blood patching delivered near or at the level of a CSF leak has been gaining in clinical utility.[8,13] Furthermore, when an EBP does not alleviate symptoms, several studies have demonstrated that targeted delivery of fibrin glue, by epidural catheter[12] or by traditional percutaneous methods[2,23,29] -as demonstrated in this case-provides resolution of neurological symptoms and headaches.
CONCLUSIONS
Slow flow or intermittent CSF leaks represent a diagnostic challenge. Failing to establish a diagnosis and localize the area of a dural breach can lead to disability and chronic pain for patients. Pressurized RIC for spinal CSF leaks offers a means of identifying CSF leaks that were previously considered beyond the resolution of standard imaging. Furthermore, this test can be performed with relatively low risk to the patient, as lumbar drain placement is commonplace in neurosurgical practice. Most importantly, this technique provides a means of avoiding excessive testing in patients with signs of SIH and no identifiable source of CSF leak.
Footnotes
Contributor Information
Stephanie Reed Falatko, Email: sreed.falatko@gmail.com.
Prashant Kelkar, Email: DrPSetty@gmail.com.
Pradeep Setty, Email: pkelkar1981@gmail.com.
Doris Tong, Email: doris.tong@michiganspineandbrainsurgeons.com.
Teck Mun Soo, Email: tsoo111292MI@comcast.net.
REFERENCES
- 1.Ali SA, Cesani F, Zuckermann JA, Nusynowitz ML, Chaljub G. Spinal-cerebrospinal fluid leak demonstrated by radiopharmaceutical cisternography. Clin Nucl Med. 1998;23:152–5. doi: 10.1097/00003072-199803000-00004. [DOI] [PubMed] [Google Scholar]
- 2.Angelo F, Giuseppe M, Eliana M, Luisa C, Gennaro B. Spontaneous intracranial hypotension: Diagnostic and therapeutic implications in neurosurgical practice. Neurol Sci. 2011;32(Suppl 3):S287–90. doi: 10.1007/s10072-011-0699-9. [DOI] [PubMed] [Google Scholar]
- 3.Beleña JM, Nuñez M, Yuste J, Plaza-Nieto JF, Jiménez-Jiménez FJ, Serrano S. Spontaneous intracranial hypotension syndrome treated with a double epidural blood patch. Acta Anaesthesiol Scand. 2012;56:1332–5. doi: 10.1111/j.1399-6576.2012.02742.x. [DOI] [PubMed] [Google Scholar]
- 4.Brady-McCreery KM, Speidel S, Hussein MA, Coats DK. Spontaneous intracranial hypotension with unique strabismus due to third and fourth cranial neuropathies. Binocul Vis Strabismus Q. 2002;17:43–8. [PubMed] [Google Scholar]
- 5.Curnes JT, Vincent LM, Kowalsky RJ, McCartney WH, Staab EV. CSF rhinorrhea: Detection and localization using overpressure cisternography with Tc-99m-DTPA. Radiology. 1985;154:795–9. doi: 10.1148/radiology.154.3.3881800. [DOI] [PubMed] [Google Scholar]
- 6.Ferrante E, Savino A, Brioschi A, Marazzi R, Donato MF, Riva M. Transient oculomotor cranial nerves palsy in spontaneous intracranial hypotension. J Neurosurg Sci. 1998;42:177–9. [PubMed] [Google Scholar]
- 7.Fishman RA, Dillon WP. Dural enhancement and cerebral displacement secondary to intracranial hypotension. Neurology. 1993;43(3 Pt 1):609–11. doi: 10.1212/wnl.43.3_part_1.609. [DOI] [PubMed] [Google Scholar]
- 8.Hayek SM, Fattouh M, Dews T, Kapural L, Malak O, Mekhail N. Successful treatment of spontaneous cerebrospinal fluid leak headache with fluoroscopically guided epidural blood patch: A report of four cases. Pain Med. 2003;4:373–8. doi: 10.1111/j.1526-4637.2003.03037.x. [DOI] [PubMed] [Google Scholar]
- 9.Hoxworth JM, Trentman TL, Kotsenas AL, Thielen KR, Nelson KD, Dodick DW. The role of digital subtraction myelography in the diagnosis and localization of spontaneous spinal CSF leaks. AJR Am J Roentgenol. 2012;199:649–53. doi: 10.2214/AJR.11.8238. [DOI] [PubMed] [Google Scholar]
- 10.Huang C, Chuang Y, Lee C, Lee R, Lin T. Spontaneous spinal cerebrospinal fluid leak and intracranial hypotension. Clin Imaging. 2000;24:270–2. doi: 10.1016/s0899-7071(00)00227-8. [DOI] [PubMed] [Google Scholar]
- 11.Hyun SH, Lee KH, Lee SJ, Cho YS, Lee EJ, Choi JY, et al. Potential value of radionuclide cisternography in diagnosis and management planning of spontaneous intracranial hypotension. Clin Neurol Neurosurg. 2008;110:657–61. doi: 10.1016/j.clineuro.2008.03.014. [DOI] [PubMed] [Google Scholar]
- 12.Kamada M, Fujita Y, Ishii R, Endoh S. Spontaneous intracranial hypotension successfully treated by epidural patching with fibrin glue. Headache. 2000;40:844–7. doi: 10.1046/j.1526-4610.2000.00153.x. [DOI] [PubMed] [Google Scholar]
- 13.Kantor D, Silberstein SD. Cervical epidural blood patch for low CSF pressure headaches. Neurology. 2005;65:1138. doi: 10.1212/01.wnl.0000178893.55200.1c. [DOI] [PubMed] [Google Scholar]
- 14.Leep Hunderfund AN, Mokri B. Second-half-of-the-day headache as a manifestation of spontaneous CSF leak. J Neurol. 2012;259:306–10. doi: 10.1007/s00415-011-6181-z. [DOI] [PubMed] [Google Scholar]
- 15.Magnaes B, Solheim D. Controlled overpressure cisternography to localize cerebrospinal fluid rhinorrhea. J Nucl Med. 1977;18:109–11. [PubMed] [Google Scholar]
- 16.Mokri B. Spontaneous cerebrospinal fluid leaks: From intracranial hypotension to cerebrospinal fluid hypovolemia – Evolution of a concept. Mayo Clin Proc. 1999;74:1113–23. doi: 10.4065/74.11.1113. [DOI] [PubMed] [Google Scholar]
- 17.Mokri B. Spontaneous intracranial hypotension. Curr Neurol Neurosci Rep. 2001;1:109–17. doi: 10.1007/s11910-001-0005-y. [DOI] [PubMed] [Google Scholar]
- 18.Moriyama E, Ogawa T, Nishida A, Ishikawa S, Beck H. Quantitative analysis of radioisotope cisternography in the diagnosis of intracranial hypotension. J Neurosurg. 2004;101:421–6. doi: 10.3171/jns.2004.101.3.0421. [DOI] [PubMed] [Google Scholar]
- 19.Pleasure SJ, Abosch A, Friedman J, Ko NU, Barbaro N, Dillon W, et al. Spontaneous intracranial hypotension resulting in stupor caused by diencephalic compression. Neurology. 1998;50:1854–7. doi: 10.1212/wnl.50.6.1854. [DOI] [PubMed] [Google Scholar]
- 20.Rando TA, Fishman RA. Spontaneous intracranial hypotension: Report of two cases and review of the literature. Neurology. 1992;42(3 Pt 1):481–7. doi: 10.1212/wnl.42.3.481. [DOI] [PubMed] [Google Scholar]
- 21.Schievink WI, Gordon OK, Tourje J. Connective tissue disorders with spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension: A prospective study. Neurosurgery. 2004;54:65–70. doi: 10.1227/01.neu.0000097200.18478.7b. [DOI] [PubMed] [Google Scholar]
- 22.Schievink WI, Louy C. Precipitating factors of spontaneous spinal CSF leaks and intracranial hypotension. Neurology. 2007;69:700–2. doi: 10.1212/01.wnl.0000267324.68013.8e. [DOI] [PubMed] [Google Scholar]
- 23.Schievink WI, Maya MM, Louy C, Moser FG, Tourje J. Diagnostic criteria for spontaneous spinal CSF leaks and intracranial hypotension. AJNR Am J Neuroradiol. 2008;29:853–6. doi: 10.3174/ajnr.A0956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Schievink WI, Meyer FB, Atkinson JL, Mokri B. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. J Neurosurg. 1996;84:598–605. doi: 10.3171/jns.1996.84.4.0598. [DOI] [PubMed] [Google Scholar]
- 25.Schievink WI, Moser FG, Pikul BK. Reversal of coma with an injection of glue. Lancet. 2007;369:1402. doi: 10.1016/S0140-6736(07)60636-9. [DOI] [PubMed] [Google Scholar]
- 26.Schievink WI, Smith KA. Nonpositional headache caused by spontaneous intracranial hypotension. Neurology. 1998;51:1768–9. doi: 10.1212/wnl.51.6.1768. [DOI] [PubMed] [Google Scholar]
- 27.Schievink WI, Wijdicks EF, Meyer FB, Sonntag VK. Spontaneous intracranial hypotension mimicking aneurysmal subarachnoid hemorrhage. Neurosurgery. 2001;48:513–6. doi: 10.1097/00006123-200103000-00009. [DOI] [PubMed] [Google Scholar]
- 28.Schievink WI. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA. 2006;295:2286–96. doi: 10.1001/jama.295.19.2286. [DOI] [PubMed] [Google Scholar]
- 29.Schievink WI. Spontaneous spinal cerebrospinal fluid leaks. Cephalalgia. 2008;28:1345–56. doi: 10.1111/j.1468-2982.2008.01776.x. [DOI] [PubMed] [Google Scholar]
- 30.Schievink WI. Spontaneous spinal cerebrospinal fluid leaks: A review. Neurosurg Focus. 2000;9:e8. doi: 10.3171/foc.2000.9.1.8. [DOI] [PubMed] [Google Scholar]
- 31.Sencakova D, Mokri B, McClelland RL. The efficacy of epidural blood patch in spontaneous CSF leaks. Neurology. 2001;57:1921–3. doi: 10.1212/wnl.57.10.1921. [DOI] [PubMed] [Google Scholar]
- 32.Stone JA, Castillo M, Neelon B, Mukherji SK. Evaluation of CSF leaks: High-resolution CT compared with contrast-enhanced CT and radionuclide cisternography. AJNR Am J Neuroradiol. 1999;20:706–12. [PMC free article] [PubMed] [Google Scholar]
- 33.Szeinfeld M, Ihmeidan IH, Moser MM, Machado R, Klose KJ, Serafini AN. Epidural blood patch: Evaluation of the volume and spread of blood injected into the epidural space. Anesthesiology. 1986;64:820–2. doi: 10.1097/00000542-198606000-00028. [DOI] [PubMed] [Google Scholar]
- 34.Vishteh AG, Schievink WI, Baskin JJ, Sonntag VK. Cervical bone spur presenting with spontaneous intracranial hypotension. Case report. J Neurosurg. 1998;89:483–4. doi: 10.3171/jns.1998.89.3.0483. [DOI] [PubMed] [Google Scholar]
- 35.Yoo HM, Kim SJ, Choi CG, Lee DH, Lee JH, Suh DC, et al. Detection of CSF leak in spinal CSF leak syndrome using MR myelography: Correlation with radioisotope cisternography. AJNR Am J Neuroradiol. 2008;29:649–54. doi: 10.3174/ajnr.A0920. [DOI] [PMC free article] [PubMed] [Google Scholar]