

Abstract
Background:
Since risk factors of hypertension are formed during adolescent period and regarding that attitudes change occurs more easily in these ages, the present paper aimed to evaluate the impact of education based on the theory of planned behavior in hypertension prevention behaviors in female adolescent students.
Methods:
In this quasi-experimental study, 160 girls of 12–16 yr old (80 in each case and control group), who had not been educated in prevention of hypertension over the recent three months, participated. Four schools in Tehran were selected based on cluster sampling method during two stages. The education was provided based on the theory of planned behavior in two sections (nutrition and physical activity) in four sessions. Data gathered before and after education through a two-part valid and reliable questionnaire. The results were analyzed based on SPSS software, version 17.
Results:
The results of independent t-test showed in the nutrition section, attitude (P=0.000), subjective norm (P=0.025), perceived control (P=0.016) and behavioral intention (P=0.025); significantly increased. About physical activity, except subjective norm (P=0.219), the mean score of the attitude (P=0.001), perceived control (P=0.000) and behavioral intention (P=0.000) revealed a significant difference between two groups.
Conclusion:
Education based on the theory of planned behavior affects the intention of preventive behaviors of hypertension in female adolescents.
Keywords: Health education, adolescent behavior, Hypertension, Theory of planned behavior
Introduction
Currently, hypertension is increasingly growing in the most of developing countries due to rapid changes in lifestyle and the increase in urbanization stress (1). As reported by World Health Statistics (2012), 28.1% of men and 25% of women suffer from systolic blood pressure (BP) more than 140 or diastolic one above 90 across the world. Such statistics are estimated 26.1% for males and 22.4% for females in Iran. In this case, a growth of cardiovascular disease for about 3%, from 2002 to 2008, has been reported in Iran (2), while the age of hypertension is decreasing. In Iran, 4.7% of total investigated 13–18 years old students had a BP higher than normal level. Furthermore, hypertension was more in females compared to males (3). In a study, systolic BP of females was significantly higher than males (4).
In line with these findings, new views about the prevention of hypertension emphasize on prevention and treatment of hypertension during the adolescence, since the risk factors for cardio-vascular disease are formed during adolescence period. Hence, it is reasonable to start a healthy lifestyle to improve health level from adolescence period (5). Considering the fact that adolescents usually do not put any limitation for their nutrition and do not consider it, inappropriate nutrition is observed in this age group more than any other group (6).
In order to increase the impact of health education, community health nurses could take advantage of behavioral change theories (7). One is the theory of planned behavior (TPB) which provides a systematic framework for the health education. According to this theory, the intention to conduct a behavior is related to an individual's positive or negative evaluation of self-performance of the particular behavior (attitude), an individual's perception about the particular behavior, which is influenced by the judgment of significant others, such as parents, spouse, friends and, teachers (subjective norms), and an individual's perceived ease or difficulty of performing the particular behavior (perceived behavioral control) (8, 9). This theory presents an appropriate framework to study behaviors associated with nutrition, such behaviors are those activities conducted to confront competitive motivations and twofold attitude, mentioning that they are influenced by social factors. Therefore, the theory that pays attention to the impact of attitudes, subjective norms, and perceived behavioral control is appropriate to conduct nutritional behaviors (10). In a study investigating the application of TPB in healthy nutritional behaviors in American adolescents, the TPB was effective to predict affecting factors of nutritional behaviors (11). All components of the TPB had a positive correlation with behavioral intention where the theory could predict the intention of physical activities accomplishment up to 58% among Australian adolescents (12).
One of the most appropriate strategies for health education is the workshop. Activities of the workshop are based on the process of problem solving, aim to provide a condition for the participants to make decisions on a health problem or behavior, and then provide their own solutions (13). School, as the focal center of education, is a suitable place, making adolescents accessible assumed as a place to acquire health information from health assistants. In this regard, Shi-Chung et al. examined nutrition-based health improvement in schools; leading to the increase of student’s attitudes in school using educational intervention (14). Further, applying the education based on TPB led to the increase of attitude, perceived behavioral control and intentional behavior in physical activity dimension (15, 16).
Considering that educational program about risk factors of hypertension rather than reinforcing tendency to improvement of sport and physical activity in schools is emphasized by health experts (17), this study designed an educational program based on TPB to investigate intention to change of nutrition and activity related behaviors among female adolescents of schools.
Material and Methods
Design and sampling
In this quasi-experimental study 160, girl adolescent were participated. For this, four schools in the central region of Tehran were selected based on cluster sampling method during two stages. According to studies related to the impact of education on the hypertension related behaviors (11), and also with regard to the Alfa error 5%, and study power 90%, the sample size equals 40 people in each group, however, by considering the loss and coefficient of cluster sampling, and also with the purpose of decreasing error, sample size was considered 80 people in each group. As the quasi-experimental studies, we had not any blinding.
The study began in December 2011 and finished in May 2012. First, each of the eight central regions of Tehran (districts number six with 30 schools, 10 with 16 schools, 11 with 21 schools and, 12 with 31 schools) was considered as a cluster, and then one school was selected from each cluster at random via table of random numbers. All students of these schools were almost 18000 and 752 students were selected in this stage. As randomly, two schools were allocated as the case group and two schools as the control group. Finally, in each school, one class and in each class 40 students were selected randomly (80 girls in the case group and 80 girls in the control group). Since the south and north regions of Tehran have considerable cultural, social, and economic differences, the comparison between the participants of these regions could make bias in the study results, therefore, the central regions of Tehran selected.
Inclusion and exclusion criteria
Overall, 12–16 year old girls who had not educated in prevention of hypertension over the recent three months and had not had a special nutritional regimen participated in the study. Not participating in even one of the class sessions, participating in the other similar educational classes, and loosing tendency to take part in the study are the criteria to get out of the study. According to the mentioned criteria, none of the samples were excluded from the study.
Measurements
The data were gathered in two stages (before education and after education) through a self-report two-part questionnaire:
The questionnaire of demographic character-ristics: The first part entailed 13 demographic items including age, parents' educational status, family members, birth order, history of specific disease, history of specific medication use, family history of hypertension and its complications, family history of certain diets use, source of acquiring health information, history of participating in sport class or team, and history of BP measurement.
The questionnaire of investigating components of TPB: The second part consisted of 49 phrases in Likert scale related to prevention of hypertension and based on TPB involving the attitude in nutritional dimension (10 phrases), attitude in physical activity dimension (8 phrases), subjective norms in nutrition dimension (6 phrases), subjective norms in physical activity dimension (5 phrases), perceived behavioral control in nutrition dimension (5 phrases), perceived behavioral control in nutrition physical activity (5 phrases), behavioral intention in nutrition dimension (5 phrases)and, behavioral intention in physical activity dimension (5 phrases). Each dimension of nutrition and physical activity was designed using the guidance of questionnaire analysis based on theory of planned behavior (18). According to the available standard instruction, the 5 point Likert-style scale is used to measure the questions (0=strongly disagree, 1=disagree, 2= having no idea, 3=agree, 4= strongly agree).
Reliability and validity
The validity of questionnaire was determined by two methods of face validity and content validity, which confirmed by 10 experts of cardiologist and 10 nurses. The total content validity index (CVI) in the “relevancy”, “simplicity”, and “clarity” respectively equals 82.5, 92.94, and 90.71. The reliability of the questionnaire further evaluated through internal consistency (α = 0.91) and test-retest (r =0.82).
Intervention
After allocating the participants into two groups of case and control, participants, their parents and deans of schools were justified with the aim and procedure of the. So after a week, a pretest was administered for both case and control groups using the questionnaire. Once more, after a week, the educational classes with the content of “teaching accurate nutrition and physical activities to prevent hypertension” were held for the case group using the workshop method during four weeks, one session a week and two hours each session (two sessions for nutrition and two sessions for physical activity). Educators were two trained health community nurses. In each session, separate times were allocated for attitude change, subjective norms change, perceived control change, and finally for question / answer. At the end of each session, participants were provided with an educational pamphlet with the summative content of the educational program due to making the opportunity to solve any question. To follow up the case group, six weeks later than the intervention, one review session held for the group. Three months after the reviewing session, a post-test was held for both groups using the same questionnaire (13). Because students were repeatedly recommended to complete all items of questionnaire, the study had not missed data. A confounding variable was the researchers’ inability to control completely the participants not to receive educational information from other educational resources during the study. Anyhow, the researchers recommended the adolescents and their families to avoid same educational programs.
Data analysis
The data were analyzed using descriptive and inferential statistics (independent t-test, K-S test, paired t-test, and Chi-Square test) through SPSS version 17 (Chicago, IL, USA). Level of significance for the test equals 0.05.
Ethical notes
The present paper is confirmed by the Ethics Committee of Tehran University of medical sciences. The research objectives were explained for all of the adolescents participating in the study, deans, and adolescents’ parents, and then the adolescents’ written consents were received. Moreover, a similar educational session presented to the control group after collecting post-test data.
Results
Descriptive results
The result of the K-S test reveals that there was no significant difference between the case and control groups in terms of all demographic characteristics (P< 0.05). The summary of demographic characteristics of participants is shown in Table 1.
Table 1:
Demographic characteristics of participants
| Variable | Classification | Percentage in Case Group | Percentage in Control Group | P-value |
|---|---|---|---|---|
| Age | 12 years | 25.7 | 32.7 | P=0.84€ |
| 13 years | 51.5 | 44.7 | ||
| 14 years and above | 22.8 | 22.6 | ||
| Father's education level | Primary and secondary school | 45.7 | 32.5 | P=0.06¥ |
| Diploma | 53.5 | 52 | ||
| Academic | 2.8 | 15.5 | ||
| Mother’s education level | Primary and secondary school | 54.4 | 50 | P=0.65¥ |
| Diploma | 42.8 | 45 | ||
| Academic | 2.8 | 5 | ||
| Family members | 2 | 5.7 | 0 | P=0.95¥ |
| 3 to 5 | 88.6 | 75 | ||
| Above 5 | 5.7 | 25 | ||
| Birth order | First | 38 | 30 | P=0.34¥ |
| Second | 29.5 | 40 | ||
| Third | 13.4 | 25 | ||
| Fourth and above | 19.1 | 5 | ||
| History of certain disease | Yes | 2.9 | 2.5 | P=0.75Ω |
| No | 97.1 | 97.5 | ||
| History of medicine use | Yes | 2.9 | 2.5 | P=0.75Ω |
| No | 97.1 | 97.5 | ||
| Family history of hypertension | Yes | 20 | 22.5 | P=0.23¥ |
| No | 80 | 77.5 | ||
| History of hypertension complications | Yes | 14.2 | 17 | P=0.54¥ |
| No | 85.8 | 83 | ||
| No | 85.7 | 80 | ||
| Family history of certain diets | Yes | 12.8 | 19.5 | P=0.34¥ |
| No | 87.2 | 80 | ||
| Source of acquiring health information (only one choice) | Radio and television | 42.2 | 40 | P=0.34¥ |
| Friends | 22.8 | 15 | P=0.29¥ | |
| Family | 54.2 | 42.5 | P=0.77¥ | |
| Books and magazines | 48.5 | 45 | P=0.83¥ | |
| Teachers | 42.5 | 50 | P=0.85¥ | |
| Individuals and health team | 11.4 | 7.5 | P=0.66Ω | |
| Other | 8.5 | 5 | P=0.50Ω | |
| History of participating in sport class or team | Yes | 31.5 | 27.5 | P=0.21¥ |
| No | 68.5 | 72.5 | ||
| History of measuring BP | Yes | 11.5 | 12.5 | P=0.61Ω |
| No | 88.5 | 87.5 |
Independent t-test/
Chi square test/
Fisher Exact
Analytical results
The results of independent t-test indicate that there is no statically significant difference between two groups in terms of the components of the TPB including attitude, subjective norm, perceived behavioral control, and behavioral intention in terms of nutrition and physical activity (P>0.05) (Table 2).
Table 2:
Comparison between Mean and SD of attitudes, subjective norm, perceived behavioral control, and behavioral intention of participants in terms of nutrition and physical activity in case group with control group before intervention
| Group Variable | Case Mean | SD | Control Mean | SD | |
|---|---|---|---|---|---|
| Nutrition | Attitude | 36.42 | 2.88 | 35.49 | 4.09 |
| Subjective norm | 19.63 | 3.51 | 20.84 | 3.60 | |
| Perceived behavioral control | 16.70 | 1.70 | 15.79 | 2.11 | |
| Behavioral intention | 17.15 | 1.37 | 16.48 | 2.69 | |
| Physical activity | Attitude | 27.80 | 2.55 | 27.54 | 3.11 |
| Subjective norm | 17.30 | 2.40 | 16.66 | 2.44 | |
| Perceived behavioral control | 16.46 | 2.19 | 14.64 | 1.91 | |
| Behavioral intention | 18.18 | 1.80 | 16.58 | 2.23 |
Further, the results of paired t-test signified that after intervention, both in nutrition and physical activity, attitude, perceived behavior control, and behavioral intention significantly increased in the case group compared to the control group while subjective norm had a significant difference only in nutrition part. There was no significant difference in components of TPB in paired t-test of the control group. (P> 0.05) (Table 3).
Table 3:
Comparison between Mean and SD of attitudes, subjective norm, perceived behavioral control, and behavioral intention of participants in terms of nutrition and physical activity in case and control groups before and after intervention
| Case Before intervention Mean | SD | After intervention Mean | SD | Control Before intervention Mean | SD | After intervention Mean | SD | ||
|---|---|---|---|---|---|---|---|---|---|
| Nutrition | Attitude | 36.42 | 2.88 | 41.27 | 2.84 | 35.49 | 4.09 | 34.58 | 3.82 |
| Subjective norm | 19.63 | 3.51 | 21.28 | 2.81 | 20.84 | 3.59 | 19.41 | 2.49 | |
| Perceived behavioral control | 16.70 | 1.70 | 18.54 | 1.31 | 15.79 | 2.11 | 15.46 | 2.65 | |
| Behavioral intention | 17.15 | 2.37 | 21.57 | 1.46 | 16.48 | 2.69 | 17.87 | 2.17 | |
| Physical activity | Attitude | 27.80 | 2.55 | 30.27 | 5.89 | 27.54 | 3.11 | 27.90 | 2.94 |
| Subjective norm | 17.30 | 2.40 | 17.97 | 2.48 | 16.66 | 2.44 | 16.53 | 2.41 | |
| Perceived behavioral control | 16.46 | 2.19 | 19.40 | 1.44 | 14.46 | 1.91 | 15.46 | 2.60 | |
| Behavioral intention | 18.18 | 1.80 | 20.41 | 2.54 | 16.58 | 2.23 | 18.31 | 2.54 |
Moreover, according to the results of independent t-test signified in Table 4, the case group compared with control group indicate a significant difference in terms of nutrition in the all dimensions of TPB and a significant difference in the dimensions of attitude, perceived behavioral control, and behavioral intention in terms of physical activity (P<0.05).
Table 4:
Comparison between Mean and SD of attitudes, subjective norm, perceived behavioral control, and behavioral intention of participants in terms of nutrition and physical activity in case group with control group after intervention
| Group Variable | Case Mean | SD | Control Mean | SD | |
|---|---|---|---|---|---|
| Nutrition | Attitude | 41.27 | 2.84 | 34.58 | 3.82 |
| Subjective norm | 21.28 | 2.81 | 19.41 | 2.9 | |
| Perceived behavioral control | 18.54 | 1.31 | 15.46 | 2.65 | |
| Behavioral intention | 21.57 | 1.45 | 17.87 | 2.17 | |
| Physical activity | Attitude | 30.27 | 5.89 | 27.90 | 2.94 |
| Subjective norm | 17.97 | 2.49 | 16.53 | 2.41 | |
| Perceived behavioral control | 19.40 | 1.44 | 15.46 | 2.60 | |
| Behavioral intention | 20.41 | 2.54 | 18.31 | 2.54 |
Discussion
The obtained results indicate that the mean of attitude, subjective norm, perceived behavioral control, and behavioral intention regarding nutrition dimension increased after the intervention in the case group. In other words, adolescent students showed higher tendency to have healthy nutritional behavior to prevent hypertension (attitude), felt more expectations from who were important to her has a healthy diet (subjective norm), and considered themselves more capable to accomplish healthy nutritional behaviors. Hence, it can conclude that the intention of healthy nutritional behaviors was increased in them. Meanwhile, attitude and behavioral intention had a more highlighted role among the components of the theory (Fig. 1 and 2). In fact, the results proved that educational intervention leads to reinforcing the beliefs and attitudes of adolescents and also the increase of mean score of behavioral intention in nutrition dimension; revealing their tendency to have healthy diets. Further, adolescent participants, followed by receiving information about the positive effect of behaviors proposed by educational program in their nutritional behaviors, showed more control to have healthy nutritional behaviors.
Fig. 1:
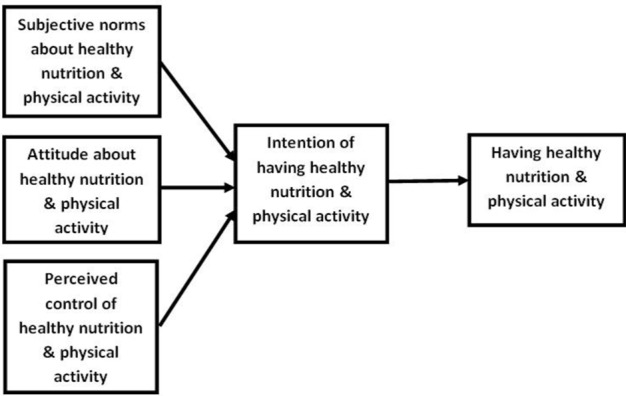
The components of TPB based on variables before education
Fig. 2:
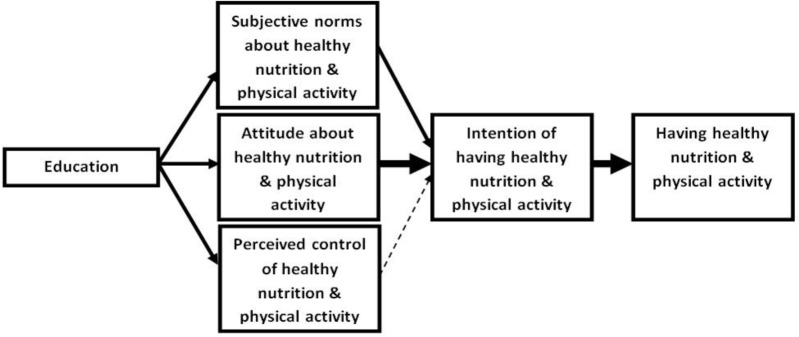
- High effect:

- Low effect:
In this regards, Tavakkoli et al. worked on nutritional behavior improvement, investigating the effect of education in nutritional behaviors in army personnel and found the findings consistent with the present paper's results (19). The research findings are also consistent with the findings reported by Jordan et al. (20). They concluded that the attitude of mothers having young children was improved after an educational intervention using training in small groups. However, the sample was inconsistent in terms of age with the current study samples, but the same educational method was used in intervention leading to the similar results.
Considering these findings, it seems that educational intervention in group sessions can increase the probability of positive changes in deterministic dimensions of attitude by providing a field to exchange information and use of peers' experiences. Attitude towards a subject is derived from the beliefs of an individual about that subject. That is, the favorable consequence of a behavior will improve the individual's attitude toward that behavior. Since the aim of the present study was to make adolescents familiar with the benefits of healthy nutritional behaviors through the proposed intervention, the obtained results were expected by the researcher.
The results obtained from physical activity dimension revealed that in the case group, all the components of theory, except subjective norm were significantly increased after the intervention. This finding is consistent with other studies, as revealed, subjective norm could not be promoted in the physical activity dimension of their sample while attitude, perceived behavioral control and behavioral intention were increased in the sample (15, 16). Merely using a theoretical program may be the cause for lack of change in the subjective norm in physical activity so that in the study by Quinn et al., attitude towards performing sport activities was increased in fat women after four practical educational sessions and four months after the intervention (21). In our study, it was better to prepare sport sessions at the schools to improve physical activities, accomplishment as a healthy behavior but sport facility was not possible for the researcher. It seems that subjective norm, signifying the importance of the behavior accomplishment of individuals, groups and communities imposed on individual, is a value established in the individuals rooted in her culture, as well as family and social values. In Iranian culture, the tendency of female adolescents to do physical activities is less than males compared with other age groups where there has been no obligation to participate in sport groups from childhood. Moreover, there is not enough sport facilities in public spaces for females. Therefore, it cannot be expected that subjective norm can be changed only through theoretical educational interventions. Another factor affecting subjective norm formation is family, which is undeniable. In this case, it may be better to hold theoretical and practical educational sessions with the participation of family members and adolescents in family groups where on families are encouraged for sport activities in family environments. Indeed, the culture of sport and increasing physical activity should firstly promoted in families to achieve this objective. In this regards, further studies are recommended.
Comparing the mean scores of the case and control groups after the intervention showed a significant difference between two groups in all components but the subjective norm in physical dimension; among them, the perceived behavioral control in both nutrition and physical activity and attitude in physical activity dimension showed the most difference which can be due to presenting better education in this part. The lack of statistically significant difference between the score of attitude, perceived behavioral control and behavioral intention both in nutrition and physical activity was expected with respect to the lack of any intervention in the control group.
Conclusion
The present study aimed to investigate the effect of education based on the TPB in preventive behaviors of hypertension in school female adolescent students. As found, using education based on TPB was effective in hypertension prevention and increased attitude, perceived behavioral control and behavioral intention in both nutrition and physical activity and subjective norms were perceived only in nutrition dimension. With regard to the results, TPB can be introduced as an appropriate theory to design and implement educational intervention in order to change healthy nutrition-related behaviors and physical activity with the aim of improving the intention of preventive behaviors of hypertension in adolescents.
Ethical considerations
Ethical issues (Including plagiarism, Informed Consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc.) have been completely observed by the authors.
Acknowledgements
The authors declare that there is no conflict of interests. This study was conducted under support of Research deputy of Faculty of Nursing and Midwifery of Tehran University of Medical Sciences.
References
- 1. Ghannem H, Darioli R, Limam K, Harrabi I, Gaha R, Trabelsi L, Fredj AH, Bouslama A. (2001). Epidemiology of cardiovascular risk factors among schoolchildren in Sousse, Tunisia. J Cardiovasc Risk, 8: 87–91. [DOI] [PubMed] [Google Scholar]
- 2. WHO (2012). World health statistics 2012. ed. World Health Organization. [Google Scholar]
- 3. Ataei N, Aghamohammadi A, Ziaee V, Hosseini M, Dehsara F, Rezanejad A. (2007). Prevalence of hypertension in junior and senior high school children in Iran. Iran J Pediatr, 17 (Suppl 2): 237–242. [Google Scholar]
- 4. Khodaii S, Faeghi A, Azizi S, Firoozian A, Jafari J. (2006). Blood pressure and obesity in young adolescents in Tehran. Iran J Pediatr, 16 ( 1): 45–50. [Google Scholar]
- 5. Black JM, Hawks JH, Keene AM. (2000). Medical-Surgical Nursing: Clinical Management for Positive Outcomes - 2-Volume Set. ed. W.B. Saunders Company. [Google Scholar]
- 6. Stanhope M, Lancaster J. (2011). Public Health Nursing: Population-Centered Health Care in the Community. 8th ed Mosby., St Louis. [Google Scholar]
- 7. Bensley RJ, Brookins-Fisher J. (2003). Community health education methods: A practical guide. ed. Jones & Bartlett Learning. [Google Scholar]
- 8. Kerr J, Weitkunat R, Moretti M. (2005). ABC of Behavior Change: A guide to successful disease prevention and health promotion. ed. Elsevier Churchill Livingstone. [Google Scholar]
- 9. Amjad N, Wood AM. (2009). Identifying and changing the normative beliefs about aggression which lead young Muslim adults to join extremist anti-Semitic groups in Pakistan. Aggressive Behav, 35: 514–519. [DOI] [PubMed] [Google Scholar]
- 10. Karimi-Shahanjarini A, Omidvar N, Bazargan M, Rashidian A, Majdzadeh R, Shojaeizadeh D. (2010). Iranian female adolescent's views on unhealthy snacks consumption: a qualitative study. Iran J Public Health, 39( 3): 92–101. [PMC free article] [PubMed] [Google Scholar]
- 11. Fila SA, Smith C. (2006). Applying the theory of planned behavior to healthy eating behaviors in urban Native American youth. Int J Behav Nutr Phy, 3: 11. 10.1186/1479-5868-3-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hamilton K, White KM. (2008). Extending the theory of planned behavior: the role of self and social influences in predicting adolescent regular moderate-to-vigorous physical activity. J Sport Exerc Psychol, 30: 56–74. [DOI] [PubMed] [Google Scholar]
- 13. Solhi Mahnaz ZF, Karimzade SK, Taghdisi MH, Jalalian F. (2012). Desighning and Implementing Educational Progran to Promote Physical Activity Among Students: An Application of the Theory of Planned Behavior. Ofoge-E-Danesh, 18( 55): 45–52. [Google Scholar]
- 14. Shi-Chang X, Xin-Wei Z, Shui-Yang X, Shu-Ming T, Sen-Hai Y, Aldinger C, Glasauer P. (2004). Creating health-promoting schools in China with a focus on nutrition. Health Promot Int, 19: 409–418. [DOI] [PubMed] [Google Scholar]
- 15. Parrott MW, Tennant LK, Olejnik S, Poudevigne MS. (2008). Theory of planned behavior: Implications for an email-based physical activity intervention. Psychol Sport Exerc, 9: 511–526. [Google Scholar]
- 16. Hardeman W, Michie S, Sutton S. (2009). Impact of a physical activity intervention program on cognitive predictors of behaviour among adults at risk of Type 2 diabetes (ProActive randomised controlled trial). Int J Behav Nutr Physic Activity, 6: 16 10.1186/1479-5868-6-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jones DW, Materson BJ, Oparil S, Wright JT. (2003). Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertens, 42: 1206–1252. [DOI] [PubMed] [Google Scholar]
- 18. Ajzen I. (1985). From intentions to actions: A theory of planned behavior: Springer-Verlag; Berlin Heidelberg. [Google Scholar]
- 19. Tavakoli H, Nasab HS, Tavakoli R, Karimi A. (2011). Study effects of education on nutritional behaviors in Iranian military personnel. The First International & 4th National Congress on health Education & Promotion, 2011. Tabtiz University of Medical Sciences, [Google Scholar]
- 20. Jordan KC, Freeland-Graves JH, Klohe-Lehman DM, Cai G, Voruganti VS, Proffitt JM, Nuss HJ, Milani TJ, Bohman TM. (2008). A nutrition and physical activity intervention promotes weight loss and enhances diet attitudes in low-income mothers of young children. Nutr Res, 28: 13–20. [DOI] [PubMed] [Google Scholar]
- 21. Quinn A, Doody C, O'Shea D. (2008). The effect of a physical activity education programme on physical activity, fitness, quality of life and attitudes to exercise in obese females. J Sci Med Sport, 11: 469–472. [DOI] [PubMed] [Google Scholar]