

Abstract
Background:
Stress in nurses may increase the prevalence of musculoskeletal discomforts.
Aim:
The aim of this study was to determine the prevalence of musculoskeletal discomforts and job stress among nurses and to investigate the association between musculoskeletal discomforts and occupational stressors.
Materials and Methods:
In this cross-sectional study, 144 nurses in one of the main referral hospitals of Tehran-Iran were randomly selected and studied. Data were collected by HSE job stress questionnaire and The Cornell Musculoskeletal Discomfort Questionnaire through interviews with nurses in their workplace.
Results:
Most reported musculoskeletal discomforts localized in the neck, back, knee and shoulder and the minimal discomforts were in wrist and elbow. On the other hand, stressors such as demand, changes in workplace, control and responsibilities had significant effect on increasing musculoskeletal discomforts of organs such as neck, shoulders and back (P < 0.001).
Conclusion:
There was a significant association between stressors such as demand, control, responsibilities and changes in workplace and reported musculoskeletal disorders, especially in neck, shoulders and back. It is suggested to use defined programs for management and control of stressors to control occupational stress in nurses. Moreover, prevention of musculoskeletal discomforts due to their high prevalence in the study population is important.
Keywords: Job stress, musculoskeletal discomfort, nurses
Introduction
Hospitals are one of the major components of health care system and its proper function in coordination with a number of other factors lead to provision of public health services.[1] Nurses play an important role in health care organizations and without efficient and resourceful nursing staff, success of health care system is threatened.[2] National Institute for Occupational Safety and Health (NIOSH) listed nursing among 40 occupations with high incidence of diseases related to excessive workload. It is also believed that nursing profession is probably at the top of stressful jobs in a healthcare system.[3] It is obvious that nurses' physical and mental health problems with higher work-related stressors are crucial factors in reducing the quantity and quality of their work performance particularly in taking care of patients. Furthermore, poor work performance would bring about physical and psychosocial problems and might result in frustration.[4,5] There are many psychosocial factors in a work environment with important role in the occurrence of musculoskeletal disorders, especially back pain.[5,6,7] Hanse et al. in their study concluded that work-related stress due to excessive mental workload has a direct impact on developing musculoskeletal disorders in personnel.[8] Yip et al. showed an elevated prevalence of musculoskeletal disorders in nurses with more stress in their study.[9] The results from another study conducted using the HSE job questionnaire, highlighted the importance of nurses' occupational stress on their performance.[10] According to Wikstrom et al., almost 30% of individuals working in the health sector, believe that their tasks are physically stressful. The study also mentioned that such proportion is more than 60% in nurses and healthcare assistants.[11] Corona et al. reported that work-related stress is one of the influential factors in causing musculoskeletal problems among health care personnel and in particular physiotherapists and nurses.[12]
Different studies showed a significant correlation between the incidence of low back pain and psychosocial factors in the work environment.[13,14] Among which, those conducted on nurses, widely highlight the significant association between psychosocial factors (including work-related stress) and musculoskeletal disorders.
Therefore, the association between work-related stress and musculoskeletal disorders is very important to better management and prevention of disorders and workforce disability. Since in previous studies, this correlation was not surveyed in Iranian nurses with probably different work-related stress such as higher work hours and having more responsibilities for patients,[15] we decided to investigate the association between work-related stress as an influential mental factor and musculoskeletal disorders, to prevent such disorders in Iranian nursing staff.
Materials and Methods
This cross-sectional study was performed from May to December 2014 in a main referral hospital in Tehran, Iran. Inclusion criteria were nurses with a minimum age of 27 years and at least 4 years of working experience. Exclusion criteria were nurses with any prior musculoskeletal or psychological disorders established before employment. From 491 working nurses of 38 internal and surgical wards, intensive care unit (ICU), cardiac care unit (CCU), emergency ward and dialysis department, 144 subjects meeting the inclusion criteria were selected by cluster random sampling method. The study was reviewed and assented in the ethical committee of AJA University of Medical Sciences and subjects were purposely entered the study after being justified on the study aims. All participants were ensured that identity and confidentiality of their responses were protected and no individual identity would be determinable through demographic variables such as age, marital status, work experience and smoking.
To evaluate subjects' musculoskeletal disorders and job stresses, two anonymous questionnaires were used as the Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) and the UK's Health and Safety Executive (HSE). CMDQ was used to collect data related to subjects' musculoskeletal disorders.[16,17,18] CMDQ is a well-designed data collection tool developed by Professor Alan Hedge and his colleagues at Cornell University in 1999.[17,18] Through three levels of disorder frequency, severity of disorder and working ability interference effects and use of a body map diagram, CMDQ evaluates the prevalence of musculoskeletal disorders of 12 body parts (totally 20 regions of the body) during the previous working week.
This questionnaire includes four parts and designed for both male and female subjects evaluating standing and sedentary tasks. CMDQ is now widely used in the US and other countries and considered as a valuable tool for evaluation of musculoskeletal disorders.[19,20] The questionnaire has also been cross-culturally adapted and its Spanish, Turkish and Persian versions are now available.[21,22]
The Cronbach's alpha coefficient for the questionnaire was 0.986. For levels of frequency of disorder, severity of disorder and working ability interference effects, the Cronbach's alpha coefficients measured as 0.955, 0.961 and 0.969, respectively. To determine the validity of questionnaire, the Visual Analogue Scale (VAS, 0-100) was used. VAS scaled subjects' pain and discomfort and the results were in agreement with the findings from Afifehzadeh-Kashani et al., who presented kappa coefficients from 0.828 to 0.960 in different organs of the body. Hence, a complete agreement obtained between the responses from visual scale and CMDQ.[22]
To assess work-related stress, the questionnaire developed by the UK's Health and Safety Executive (HSE) was used. The questionnaire consists of 35 items and seven subscales and designed at the end of 1990s to assess workers and employees' stress level.
The seven subscales of the HSE questionnaire are literally the major factors that contribute to the work-related stress among employees. These seven subscales are 1. Demands include topics such as workload, job characteristics and work environment, 2. Control how much a person is in the course of their work, 3. Support provided by management, 4. Support provided by colleagues, 5. Relationships at work, 6. Organizational change, 7. Changes in organization resources.[23] Receiving lower scores signifies being exposed to higher risks of stressors (increased stress level). The questionnaire has been successfully used in assessing the stress level among military personnel,[24] nursing and surgery staff.[25] The HSE questionnaire has been validated in several Iranian studies and considered as suitable and valid for the assessment of work-related stress based on the obtained results.
Statistical analysis
The data collected through the questionnaire was eventually analysed using SPSS statistical software (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.) by Pearson test.
Results
The mean age of participants was 34.95 ± 4.41 years ranged 27 to 43 years and 50.7% of them were male. The subjects' work experience was 11.19 ± 4.25 years with minimum 4 and maximum 14 years of experience.
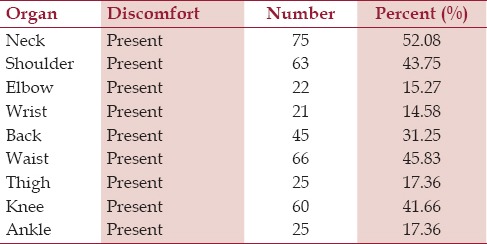
Based on participants' report, the highest level of discomfort associated with involved anatomical sites were neck (52.08%), waist (45.83%), shoulder (43.75%) and knee (41.66%), respectively. Also the lowest level of discomfort was in wrists (14.58%). Table 1 shows the prevalence of musculoskeletal disorders in nurses.
Table 1.
Prevalence of musculoskeletal disorders among nurses based on the Cornell Scale
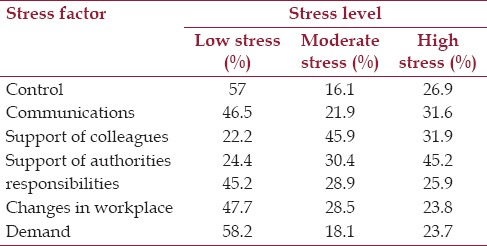
According to the results of HSE Occupational Stress questionnaire, demand and control were respectively the major stressors causing the highest level of stress in nurses. Support from colleagues and authorities were considered the least frequent stressors. Table 2 shows the frequency of stressors contributing to the level of stress among nurses.
Table 2.
Prevalence of stress factors in the stress level
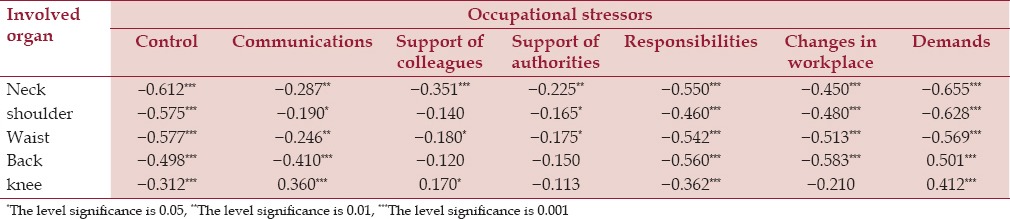
The results showed that factors such as stress, job demands, control and changes have a significant association with reported discomfort in the body organs, especially neck, shoulders, back and hip. The association between stressors and involved organs are presented in Table 3.
Table 3.
The relationship between stressors and involved organs
Discussion
The main objective of this study was to examine the effects of mental factors (particularly work-related stress) on musculoskeletal disorders among 144 Iranian nurses in different departments of a main referral hospital in Tehran, Iran. For this goal, we used two comprehensive questionnaires; HSE and CMDQ which provided a complete description of subject musculoskeletal disorders and job stresses. The results indicated a significant association between work-related stress (manifested as job demands, control, responsibilities and changes in workplace) and subjects' musculoskeletal disorders.
In this study, most musculoskeletal problems reported by nurses were associated to necks and backs, which is consistent with the results of Maul et al.[26] In another study by Lagerström et al., a significant proportion of nurses had back pain,[27] which could be due to nature of their tasks; bending, rotating, moving the patient, lifting heavy objects etc.[19,28] Furthermore, based on the results of HSE job stress questionnaire, job demands, responsibilities at work, changes in workplace, control and communications inflict stress on the nursing staff.
To study the importance of job demands on nurses, the study by Karasek et al. revealed that demands and requirements are the main contributors to cause fatigue and health problems such as musculoskeletal disorders. This is almost in agreement with the results of this study.[29]
Studies performed by the NIOSH emphatically demonstrated the obvious effect of control on job, role ambiguity, poor decision making and some other stressors in causing musculoskeletal disorders.[30] Choobineh et al. showed that excessive amount of physical and mental stress on nurses may increase the prevalence of musculoskeletal disorders among them.[31] Study by the Karask research team indicated high levels of job demands in nursing profession among which high level of physical demands would increase the likelihood of physical harm, especially musculoskeletal disorders. They also revealed that fatigue and disorders are the consequences of interaction between high psychological job demands and low control of individuals over their working activities.[32] Control in decision making is of other influential factors on work-related stress, which is consistent with the study of Barzideh et al.[33] and Karask et al.[32]
Smithi et al. showed that higher levels of work-related stress increase the prevalence of musculoskeletal problems, and the type of stressor can be associated with a particular musculoskeletal disorder. This means that poor decision making and excessive mental workload might lead to neck problems; low control on working activities along with lack of participation in decision making causes hand-related disorders and inadequate social support is a contributor to elbow pain.[34]
Hanse et al. cited that inadequate power to control working activities is one of the major reasons for development of job stress and job related injuries, which is in agreement with the findings of our study.[8]
Another influential factor is the role. Moore et al. presented a theory that job stress arises from the structure of the organization and phenomena such as role ambiguity, role conflict and work pressure are of the main concerns.[35]
Results from a study conducted in hospital nurses in Kashan showed that duality of roles, scope of responsibility and workload are significant contributors of stress in nurses.[36]
The results from multiple studies suggest that personality traits play an important role in developing, reducing or eliminating disorders.[37,38] These are consistent with the results of our study.
On the other hand, some studies have shown that physical, social and psychological needs might be the main reason for changing jobs among health professionals.[39] Changing job is of factors affecting nurses' work-related stress; career change is a serious challenge for health care professionals.[40] Golparvar et al. reported that mismatch between individuals' capabilities and job demands along with working on a new job, cause work-related stress.[41]
Conclusion
Identifying, assessing and prioritizing work-related stressors are important for prevention of work-related disorders. In the meantime, nurses due to the essence of their profession, are more prone to harms caused by such stressors. In this study, a significant association was found between nurses' musculoskeletal disorders and work-related stress. Additionally, there was a significant association between work-related stressors such as job demands, having control over working activities, individual's roles, changes and reported musculoskeletal disorders, especially in neck, shoulder, back and waist. Due to high prevalence of musculoskeletal disorders among the population of Iranian nurses in this study, measures should be taken to manage and control nurses' work-related stress. Therefore, controlling physical pressure and improving working conditions as well as considering psychosocial factors are some priorities in this regard.
Financial support and sponsorship
This study is funded by AJA University of Medical Sciences in Tehran, Iran.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
A special thank you goes to those who contributed to this paper.
References
- 1.Asefzadeh S, Rezapour A. Health Management. 2nd ed. Qazvin: Qazvin University of Medical Sciences Publication; 2008. pp. 173–174. [Google Scholar]
- 2.Eastaugh SR. Hospital nurse productivity enhancement. J Health Care Finance. 2007;33:39–47. [PubMed] [Google Scholar]
- 3.Levy BS, Wegman DH. Occupational Health: Recognizing And Preventing Work-Related Disease and Injury. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2000. pp. 715–727. [Google Scholar]
- 4.Fortinash KM, Holoday Worret PA. Psychiatric Mental Health Nursing. 4th ed. St. Louis: Mosby; 2008. [Google Scholar]
- 5.Winwood PC, Lushington K. Disentangling the effects of psychological and physical work demands on sleep, recovery and maladaptive chronic stress outcomes within a large sample of Australian nurses. J Adv Nurs. 2006;56:679–89. doi: 10.1111/j.1365-2648.2006.04055.x. [DOI] [PubMed] [Google Scholar]
- 6.Huang GD, Feuerstein M, Sauter SL. Occupational stress and work-related upper extremity disorders: Concepts and models. Am J Ind Med. 2002;41:298–314. doi: 10.1002/ajim.10045. [DOI] [PubMed] [Google Scholar]
- 7.Ghaffari M, Alipour A, Farshad AA, Jensen I, Josephson M, Vingard E. Effect of psychosocial factors on low back pain in industrial workers. Occup Med (Lond) 2008;58:341–7. doi: 10.1093/occmed/kqn006. [DOI] [PubMed] [Google Scholar]
- 8.Hanse JJ, Forsman M. Identification and analysis of unsatisfactory psychosocial work situations: A participatory approach employing video-computer interaction. Appl Ergon. 2001;32:23–9. doi: 10.1016/s0003-6870(00)00057-0. [DOI] [PubMed] [Google Scholar]
- 9.Yip VY. New low back pain in nurses: Work activities, work stress and sedentary lifestyle. J Adv Nurs. 2004;46:430–40. doi: 10.1111/j.1365-2648.2004.03009.x. [DOI] [PubMed] [Google Scholar]
- 10.Arbabisarjou A, Ajdari Z, Omeidi KH, Jalalinejad R. The relationship between Job stress and performance among the hospitals Nurses. World Sci J. 2013;1:181–8. [Google Scholar]
- 11.Wickström G, Laine M, Pentti J, Elovainio M, Lindström K. Work Conditions and Wellbeing in the Social and Health Care Sector - Changes in the 1990's. Helsinki: Finnish Institute of Occupational Health; 2000. [Google Scholar]
- 12.Corona G, Amedei F, Miselli F, Padalino MP, Tibaldi S, Franco G. Association between relational and organizational factors and occurrence of musculoskeletal disease in health personnel. G Ital Med Lav Ergon. 2005;27:208–12. [PubMed] [Google Scholar]
- 13.Rosenstock L, Cullen M, Brodkin C, Redlich C. Textbook of Clinical Occupational and Environmental Medicine. 4th ed. Philadelphia: Elsevier Health Sciences; 2004. [Google Scholar]
- 14.Musculoskeletal Disorders and the Workplace: Low Back and Upper Extremities. Washington DC: National Academies Press; 2001. National Research Council (US) and Institute of Medicine (US) Panel on Musculoskeletal Disorders and the Workplace. [PubMed] [Google Scholar]
- 15.Malekpour F, Mohammadian Y, Malekpour AR, Mohammadpour Y, Sheikh Ahmadi A, Shakarami A. Assessment of mental workload in nursing by using NASA- TLX. J Urmia Nurs Midwifery Fac. 2014;11:892–9. [Google Scholar]
- 16.Huang Y, Robertson MM, Chang K. The Role of Environmental Control on environmental satisfaction, communication, and psychological stress: Effects of office ergonomics training. Environ Behav. 2004;36:617–37. [Google Scholar]
- 17.Hedge A, Morimoto S, McCrobie D. Effects of keyboard tray geometry on upper body posture and comfort. Ergonomics. 1999;42:1333–49. doi: 10.1080/001401399184983. [DOI] [PubMed] [Google Scholar]
- 18.Stanton NA, Hedge A, Brookhuis K, Salas E, Hendrick HW. Handbook of Human Factors and Ergonomics Methods. Boca Raton: CRC Press; 2004. [Google Scholar]
- 19.Menzel NN, Brooks SM, Bernard TE, Nelson A. The physical workload of nursing personnel: Association with musculoskeletal discomfort. Int J Nurs Stud. 2004;41:859–67. doi: 10.1016/j.ijnurstu.2004.03.012. [DOI] [PubMed] [Google Scholar]
- 20.Fagarasanu M, Kumar S. Musculoskeletal symptoms in support staff in a large telecommunication company. Work. 2006;27:137–42. [PubMed] [Google Scholar]
- 21.Erdinc O, Hot K, Ozkaya M. Turkish version of the Cornell Musculoskeletal Discomfort Questionnaire: Cross-cultural adaptation and validation. Work. 2011;39:251–60. doi: 10.3233/WOR-2011-1173. [DOI] [PubMed] [Google Scholar]
- 22.Afifehzadeh-Kashani H, Choobineh A, Bakand S, Gohari M, Abbastabar H, Moshtaghi P. Validity and reliability farsi version cornell musculoskeletal discomfort questionnaire (CMDQ) Iran Occup Health J. 2011;7:10. [Google Scholar]
- 23.Cousins R, Mackay CJ, Clarke SD, Kelly C, Kelly PJ, McCaig RH. Management standards and work-related stress in the UK: Practical development. Work Stress. 2004;18:113–36. [Google Scholar]
- 24.Azad-Marzabadi E, Golami Fesharaki M. Reliability and validity assessment for the HSE job stress questionnaire. J Behav Sci. 2011;4:11–2. [Google Scholar]
- 25.Sahraian A, Davidi F, Bazrafshan A, Javadpour A. Occupational Stress among Hospital Nurses: Comparison of Internal, Surgical, and Psychiatric Wards. Int J Community Based Nurs Midwifery. 2013;1:182–90. [Google Scholar]
- 26.Maul I, Läubli T, Klipstein A, Krueger H. Course of low back pain among nurses: A longitudinal study across eight years. Occup Environ Med. 2003;60:497–503. doi: 10.1136/oem.60.7.497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lagerström M, Josephson M, Pingel B, Tjernström G, Hagberg M. The Moses Study Group. Evaluation of the implementation of an education and training programme for nursing personnel at a hospital in Sweden. Int J Ind Ergonom. 1998;21:79–90. [Google Scholar]
- 28.Mosadegh Rad AM. Eximine the Relationship between nurses' knowledge about ergonomics and job injuries. J Shahrekord Univ Med Sci. 2004;6:21–32. [Google Scholar]
- 29.Karasek R, Theorell T. Stress, Productivity and Reconstruction of Working Life. New York: Basic Books; 1992. [Google Scholar]
- 30.Sauter S, Hurrell J, Murphy L, Levi L. Psychosocial and organizational factors. In: Stellman JM, editor. Encyclopaedia of Occupational Health and Safety. 4th ed. Vol. 2. Geneva, Switzerland: International Labour Office; 1998. pp. 34.1–34.77. [Google Scholar]
- 31.Choobineh A, Rajaeefard A, Neghab M. Perceived demands and musculoskeletal disorders among hospital nurses. Hakim Research Journal. 2007;10:70–5. doi: 10.1080/10803548.2006.11076699. [DOI] [PubMed] [Google Scholar]
- 32.Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B. The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol. 1998;3:322–55. doi: 10.1037//1076-8998.3.4.322. [DOI] [PubMed] [Google Scholar]
- 33.Barzideh M, Choobineh A, Tabatabaei S. Job stress dimensions and their relationship to job change intention among nurses. J Ergono. 2013;1:33–42. [Google Scholar]
- 34.Smith MJ, Conway FT, Karsh BT. Occupational stress in human computer interaction. Ind Health. 1999;37:157–73. doi: 10.2486/indhealth.37.157. [DOI] [PubMed] [Google Scholar]
- 35.Moore S, Lindquist S, Katz B. Home health nurses: Stress, self-esteem, social intimacy, and job satisfaction. Home Care Provid. 1997;2:135–41. doi: 10.1016/s1084-628x(97)90139-8. [DOI] [PubMed] [Google Scholar]
- 36.Bahrami A, Akbari H, Mousavi SG, Hannani M, Ramezani Y. Job stress among the nursing staff of Kashan hospitals. KAUMS Journal (FEYZ) 2011;15:366–73. [Google Scholar]
- 37.Widiger TA. Five factor model of personality disorder: Integrating science and practice. J Res Pers. 2005;39:67–83. [Google Scholar]
- 38.Widiger TA, Seidlitz L. Personality, psychopathology, and aging. J Res Pers. 2002;36:335–62. [Google Scholar]
- 39.Choobineh A, Movahed M, Tabatabaie SH, Kumashiro M. Perceived demands and musculoskeletal disorders in operating room nurses of Shiraz city hospitals. Ind Health. 2010;48:74–84. doi: 10.2486/indhealth.48.74. [DOI] [PubMed] [Google Scholar]
- 40.Hayes LJ, O'Brien-Pallas L, Duffield C, Shamian J, Buchan J, Hughes F, et al. Nurse turnover: A literature review - an update. Int J Nurs Stud. 2012;49:887–905. doi: 10.1016/j.ijnurstu.2011.10.001. [DOI] [PubMed] [Google Scholar]
- 41.Golparvar M, Hosseinzadeh B. Model of relation between person-job none fit with emotional exhaustion and desire to leave work: Evidence for the stress - unequilibrium-compensation model. J Appl Psychol. 2011;5:41–56. [Google Scholar]