

A 76 year old man presented to the emergency department, Tri-Service General Hospital, Taiwan, with intermittent dull abdominal pain for three weeks in August 2013. One reducible soft mass was found over his left flank under the ribs and enlarged when coughing. The computed tomography (CT) of abdomen demonstrated a herniation of retroperitoneal fat through left superior lumbar space, also known as Grynfeltt triangle (Fig. 1). He underwent lumbar oblique incision to return the hernia sac and repaired the defect by layered closure in a right decubitus position (Fig. 2A and 2B). The patient exhibited no symptoms six months after discharge.
Fig. 1.

The computed tomography of abdomen showed retroperitoneal fat protruding through Grynfeltt's triangle (bold red arrow) bound by the 12th rib superiorly (thin red arrow), the quadratus lumborum muscle medially (triangle), and internal oblique muscle laterally (asterisk).
Fig. 2A.
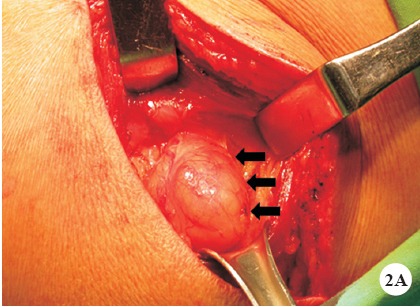
The operation demonstrated a soft, tympanic and compressible herniated sac with a smooth surface (arrows).
Fig. 2B.
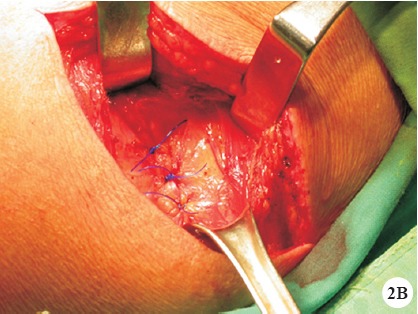
The defect was repaired by direct apposition of the internal oblique muscle and fascia with non-absorbable sutures.
Grynfeltt hernia may sometimes cause incarceration, strangulation, and bowel obstruction. Enlarged bulging size is an important clue to differentiate from lipoma by increasing intra-abdominal pressure, such as coughing. Prompt abdominal CT and early surgical repair can prevent possible bowel ischaemia.