

Abstract
Cardiac contusion is usually caused by blunt chest trauma and, although it is potentially a life-threatening condition, the diagnosis of a myocardial contusion is difficult because of non-specific symptoms and the lack of an ideal test to detect myocardial damage. Cardiac enzymes, such as creatine kinase (CK), creatine kinase MB fraction (CK-MB), cardiac troponin I (cTn-I), and cardiac troponin T (cTn-T) were used in previous studies to demonstrate the blunt cardiac contusion (BCC). Each of these diagnostic tests alone is not effective for diagnosis of BCC. The aim of this study was to investigate the serum heart-type fatty acid binding protein (h-FABP), N-terminal pro-B-type natriuretic peptide (NT-proBNP), CK, CK-MB, and cTn-I levels as a marker of BCC in blunt chest trauma in rats. The eighteen Wistar albino rats were randomly allocated to two groups; group I (control) (n=8) and group II (blunt chest trauma) (n=10). Isolated BCC was induced by the method described by Raghavendran et al. (2005). All rats were observed in their cages and blood samples were collected after five hours of trauma for the analysis of serum h-FABP, NT-pro BNP, CK, CK-MB, and cTn-I levels. The mean serum NT-pro BNP was significantly different between group I and II (10.3±2.10 ng/L versus 15.4±3.68 ng/L, respectively; P=0.0001). NT-pro BNP level >13 ng/ml had a sensitivity of 87.5%, a specificity of 70%, a positive predictive value of 70%, and a negative predictive value of 87.5% for predicting blunt chest trauma (area under curve was 0.794 and P=0.037). There was no significant difference between two groups in serum h-FABP, CK, CK-MB and c Tn-I levels. A relation between NT-Pro BNP and BCC was shown in this study. Serum NT-proBNP levels significantly increased with BCC after 5 hours of the blunt chest trauma. The use of NT-proBNP as an adjunct to other diagnostic tests, such as troponins, electrocardiography (ECG), chest x-ray and echocardiogram may be beneficial for diagnosis of BCC.
Keywords: NT-Pro BNP, h-FABP, blunt chest trauma, blunt cardiac contusion, trauma, emergency medicine
Introduction
There is a limited amount of data available on the pathophysiological mechanism and functional implications of blunt cardiac contusion [1]. The spectrum of injury of blunt cardiac contusion (BCC) (formerly known as myocardial contusion) varies from contused myocardium, showing muscle necrosis, edema, and hemorrhagic infiltrate to cardiac rupture [2,3]. The BCC also could be manifested indifferent forms of life threatening cardiac rhythm disturbance, such as ventricular flutter/fibrillation, without any morphological changes [4,5].
Due to the fact that there is no gold standard test for diagnosis of BCC, its incidence varies widely among clinical series of trauma patients, ranging between 8 and 76% [1,6]. On the other hand, autopsy studies reported the incidence of BCC in patients who died after major blunt trauma to range between 14% and 16% [7].
Heart-type fatty acid binding protein (h-FABP) which is a soluble cytoplasmic protein consisting of 132 amino acid residues and weighing 14.9 kd, is reported to be a rapid marker of perioperative myocardial damage that peaks earlier than CK-MB or cTn-T in adults [8,9]. Small studies have also examined the utility of serum h-FABP for predicting the risk of myocardial damage [8]. But sufficient evidence has not demonstrated for predicting BCC.
Increased serum N-terminal pro-B-type natriuretic peptide (NT-proBNP) is a useful marker for diagnosis and prognosis of impaired cardiac function in patients with congestive heart failure, ischemic heart disease or sepsis [10,11]. Also the levels of NT-proBNP concentrations are shown to increase in patients with left ventricular dysfunction [11]. Measurement of NT-proBNP may be useful for estimating cardiac injury in patients with blunt chest trauma [10]. However, as h-FABP, also there is no sufficient evidence related to NT-proBNP for predicting BCC [8].
In this study, we investigated the importance of some biomarkers such as CK, CK-MB, cTn-I, h-FABP and NT-proBNP in the predicting of cardiac contusions after blunt chest trauma.
Material and methods
Study design and settings
This experimental study was conducted at the Experimental Medicine and Research Center of Yeditepe University Faculty of Medicine after approval from the Local Ethical Committee of the Turkish Republic Yeditepe University for Animal Studies (Decision Number: 321, 13/03/2013).
Preparation of experimental animals
This study was conducted using eighteen Wistar albino rats weighting 250 to 300 grams.
Care of the animals was in accordance with the recommendations of the Helsinki Declaration and the guidelines of French regulations for animal experiments.
Before the study, all animals were kept in metal cages at 22°C with a 12-hour light/dark cycle for 10 days. Animals were fed with a standard rat chow with water ad libitum until the time they were used for experimentation. After lung contusion, the animals were given free access to pellet feed and water.
Experimental protocol
The rats were randomly allocated to two groups; group I (control) (n=8) and group II (blunt chest trauma) (n=10).
Blunt chest trauma model
The all rats were anaesthetized by intraperitoneal administration of 40 mg/kg of ketamine hydrochloride (Ketalar, 50 mg/mL, Pfizer, Istanbul, Turkey) and fixed on a platform in the supine position by attaching all four legs to the platform with sticky tape. BCC was induced by employing the method for isolated BCC described by Raghavendran et al [12,13].
A hollow cylindrical weight (400 g) was dropped from a height of 50 cm (impact energy =1.96 J) on to a Lexon plate with an attached precordial shield placed on the chest of the supine rat. The precordial shield was designed to protect the heart from contusion and thus directed the impact energy bilaterally to the lungs of the rats. The impact energy generated via this mechanism was calculated with the following equation: E=mgh [E: energy; g: gravity (9.8 m/s2); h: height from the Lexon plate (50 cm) and m: mass of the cylindrical weight (0.40 kg)]. Total energy transferred to the chest wall of the rat was 1.96 J.
All rats were observed in their cages 5 h after trauma.
Biochemical analysis
Collection of samples
At the end of the observation period, mid sternotomy was performed on each rat and 4 mL of blood was collected from the left ventricle of rats. At the end of the experimental period, the rats were sacrificed.
Blood samples were collected (5 ml gel tube and 2 ml K2-EDTA) and centrifuged 4000 rpm for 10 minutes and then samples were analyzed within 30 minutes. Heart tissue samples were placed in 10% neutral formaldehyde and stored at 4°C for evaluation of tissue damage.
c Troponin-I measurements
We measured cardiac cTn-I testing (Tn-I Ultra assay on Advia Centaur XP (Germany) automated chemiluminescence analyzer and reported ng/ml.
CK-MB and CK activities measurements
Serum CK-MB and CK activities were determined by respectively enzymatic immune-inhibition and kinetic methods on Beckmann Coulter AU680 chemistry analyzer (CA, USA) and reported U/L.
N-terminal pro-B-type natriuretic peptide measurements
NT-pro BNP levels were analyzed (K2-EDTA anticoagulated whole blood) using time resolved florescence assay on AQT90 FLEX immunoassay analyzer (Radiometer, DK) and reported in ng/L.
Heart fatty acid-binding protein measurements
The serum h-FABP was measured quantitatively by a Sandwich enzyme-linked immunosorbentassay (ELISA) technique, using Rat (h-FABP) ELISA kit manufactured by Sun Red, Shanghai, China. According to manufacturer’s instructions; a sensitivity 1.424 ng/ml, assay range: 1 ng/ml-450 ng/ml was used (Catalog No: 201-11-0644). The end product was measured spectrophotometrically at 450 nm using ELx800 Absorbance Microplate Reader (Bio Tek® Instruments, Inc Winooski, Vermont, USA).
Statistical methods
The data of this study were analyzed by using the statistical software of Number Cruncher Statistical System (NCSS) version 2007 (Utah, USA). Data were expressed by descriptive statistics (mean and standard deviation). For a comparison of variables of normal distribution, the t-test for independent samples was used and Mann-Whitney U test was used for the comparison of variables with non-normal distribution. The Fisher’s exact test was used to analyze qualitative variables and Pearson correlation analyses were used to determine relationships between variables. The results were considered significant at P<0.05.
Results
All rats survived the study period
There was a significant difference in mean serum NT-pro BNP levels between group I and II (were 10.3±2.10 ng/L and 15.4±3.68 ng/L respectively, P=0.0001) (Figure 1).
Figure 1.
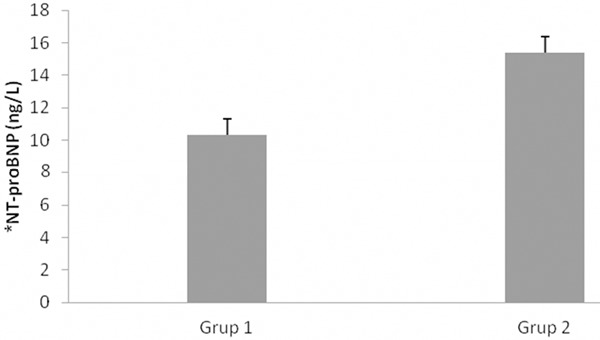
Serum NT-proBNP levels of the study groups. *NT-proBNP: N-terminal pro-B-type natriuretic peptide.
NT-pro BNP levels more than 11 had a sensitivity of 80%, a specificity of 75%, a positive predictive value of 80%, and a negative predictive value of 75% in predicting blunt chest trauma [(area under curve was 0.775 (0.540-1.00) and P=0.015].
The cut-off values of NT-pro BNP levels for predicting chest trauma were determined by Receiver operating characteristic ROC analysis (Figure 2).
Figure 2.
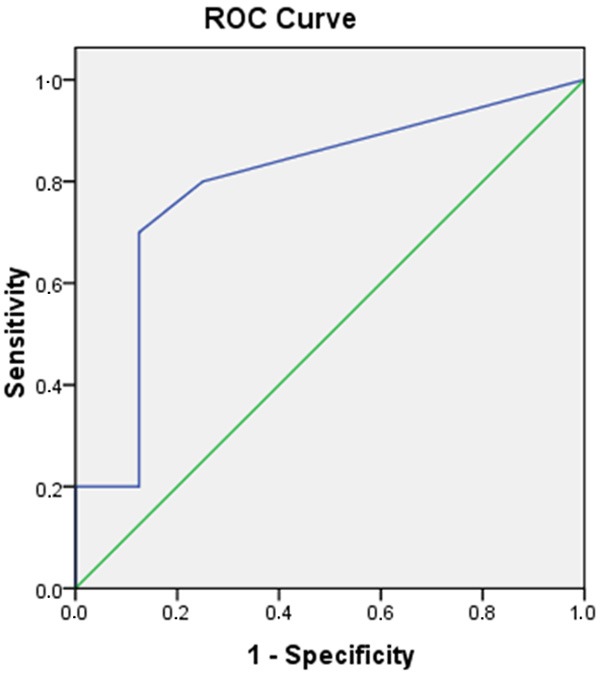
Receiver operating characteristic (ROC) curve showing the ability of N-terminal pro-brain natriuretic peptide (NT-proBNP) to identify patients with chest trauma. Area under curve: 0.788.
NT-pro BNP levels more than 13 had a sensitivity of 87.5%, a specificity of 70%, a positive predictive value of 70%, and a negative predictive value of 87.5% in predicting blunt chest trauma (area under curve was 0.794 and P=0.037) (Table 1).
Table 1.
Diagnostic Values of the pro-BNP
| AUC | Cut-off | Sensitivity | Specificity | PPV | NPV | Accuracy | |
|---|---|---|---|---|---|---|---|
| Prob-BNP | 0.788 | 13 | 87.5 | 70 | 70 | 87.5 | 77.7 |
| Prob-BNP | 0.775 | 11 | 80 | 75 | 80 | 75 | 77.7 |
AUC: Area under curve, PPV: Positive Predictive Value, NPV: Negative Predictive Value, Prob-BNP: N-terminal pro-B-type natriuretic peptide.
There was no a significant difference between the groups (control and blunt chest trauma) in terms of the serum h-FABP (P>0.05) (Figure 3).
Figure 3.
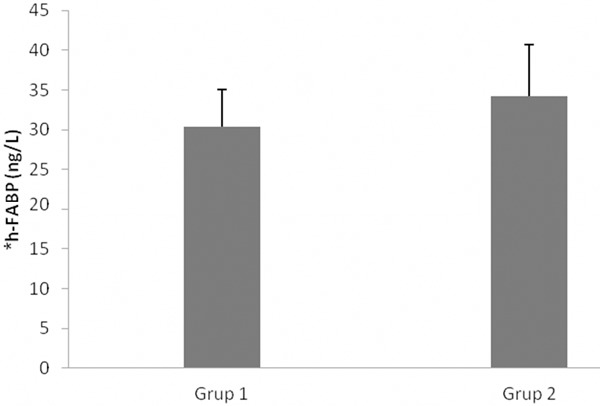
Serum h-FABP levels of the study groups. *h-FABP: Heart fatty acid-binding protein.
There was no significant difference between the groups (control and blunt chest trauma) in terms of the serum CK, CK-MB and c Tn-I (P>0.05).
Histopathological analysis of the rat heart showed moderate injury of the heart. The cardiac tissues removed from the blunt chest trauma group had moderate histopathological changes including hemorrhage (Figure 4).
Figure 4.
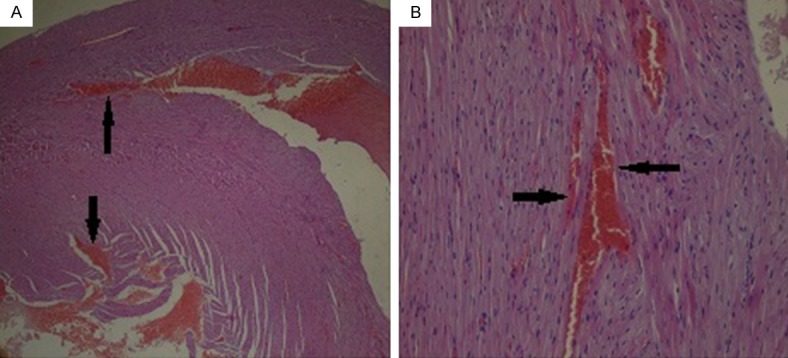
Histopathological evaluation; There is moderate haemorrhage between myocardiocytes (arrow) A: ×20, B: ×200.
Discussion
Due to lack of clear diagnostic criteria and reliable diagnostic tests for BCC, various diagnostic modalities have been used to aid in the diagnosis to prevent its potential life-threatening complications, including cardiac arrhythmias, hypotension, cardiogenic shock, hemopericardium, coronary vessel and valvular injury, and cardiac rupture [14-16].
Electrocardiography, echocardiography, angiography, and CT imaging methods are frequently used in clinical practice and also cardiac enzymes, such as CK, CK-MB, c Tn-I, and c Tn-T were used in previous studies to demonstrate the BCC [6,17]. However, these diagnostic methods alone are not effective in determining BCC.
The incidence of BCC varies from 29-56% in studies utilizing ECG as the diagnostic criteria, 3-56% in studies utilizing echocardiogram and 15-24% in studies utilizing cardiac biomarker measurements [5]. Hayes et al. has been reported that ECG results were not very specific but were sensitive enough in identifying potential problems in blunt thoracic injury [18]. There is general agreement for the use of troponins in ruling out myocardial contusion. While the specificities of troponins are generally low, the sensitivities are statistically acceptable in BCC [19,20].
Fabian et al. has demonstrated that the CK, CK-MB and cTn-I levels would be the most relevant test in determining myocardial injury but another study by Drs. Peer and Firmin concluded that only ECG abnormalities could accurately identify myocardial trauma sites and therefore cardiac enzymes and echocardiogram were not useful in predicting which patient required further care [21,22].
Pretre et al. has demonstrated in ischemic heart disease that cellular death occurs slowly after malperfusion, and elevated troponin I levels are not detected until 6 hours after the onset of myocardial injury and may persist for 3 weeks, depending on the extent of permanent cell damage [1].
Meier R. et al. has reported an elevation of serum troponin I levels immediately after the trauma and a return to the baseline levels after 20 min. This early increase of troponin I levels can be explained by the direct myocardial cell damage caused by the BCC and it correlates with clinical observations of early elevated troponin levels in patients with cardiac trauma [19,23,24].
Some studies introduced serum h-FABP as a marker for early evaluation of myocardial damage [8,25]. Due to the advantage of this protein’s features such as being low-molecular weight and cytosolic localization, it leaks out easily from the injured myocardium and immediately enters the blood circulation [8,10].
In this study, we detected that CK, CK-MB, c Tn-I and h-FABP were not useful in determining BCC in the first 5 hours after blunt chest trauma. More time may be required for significant increase of these markers.
In this study, a significant increase was observed in the serum NT-proBNP level in the BCC group during the first 5 hours after BCC. BNP is secreted mainly from the left ventricle in healthy adults as well as in patients with conditions that cause left ventricular dysfunction and ventricular pressure overload status such as pulmonary embolism, corpulmonale, and primary pulmonary hypertension [10,25,26].Increased wall tension of the left ventricle results in an increase the rate of BNP secretion [10,26].
Several studies have shown that BNP values less than 100 pg/mL are very specific for normal heart function [10,27].
Regarding the issue of BNP alteration in trauma patients, Kia and colleagues reported that BNP levels were below normal as an initial marker of bleeding, considering this an indicator of intravascular volume loss [28]. In contrast, Stewart and colleagues found no correlation of BNP and cardiac dysfunction [29].
Few studies have attempted to define the normal value of NT-pro BNP or to find the cut-off value that allows the best balance between sensitivity and specificity for predicting BCC [10,27]. But a relation between NT-Pro BNP and BCC has not been noted previously.
In this study, a significant increase was observed in the serum NT-pro BNP level in BCC group. In addition, ROC analysis showed that NT-pro BNP level as a cut-off value of >13 ng/mL is a good predictor of BCC.
This early increase of NT-pro BNP level may be explained by the direct myocardial cell damage caused by the BCC, and it may be used in the diagnosis of BCC.
In conclusion, a relation between NT-Pro BNP and BCC has not been noted previously. We observed a statistically significant relation between BCC and serum NT-Pro BNP level. Serum NT-pro BNP levels significantly correlate with BCC 5 hours after blunt chest trauma. As such, the use of NT-pro BNP as an adjunct to other diagnostic tests such as troponins, ECG, chest x-ray and echocardiogram may be beneficial for diagnosis of BCC.
Acknowledgements
We thank to Rana Konyalioglu for statistical analysis and Hakan Kocoglu who provided medical writing support.
Disclosure of conflict of interest
None.
References
- 1.Sybrandy KC, Cramer MJ, Burgersdijk C. Diagnosing cardiac contusion: old wisdom and new insights. Heart. 2003;89:485–489. doi: 10.1136/heart.89.5.485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mascaro M, Trojian TH. Blunt cardiac contusions. Clin Sports Med. 2013;32:267–271. doi: 10.1016/j.csm.2012.12.004. [DOI] [PubMed] [Google Scholar]
- 3.Swaanenburg JC, Klaase JM, DeJongste MJ, Zimmerman KW, ten Duis HJ. Troponin I, troponin T, CKMB-activity and CKMB-mass as markers for the detection of myocardial contusion in patients who experienced blunt trauma. Clin Chim Acta. 1998;272:171–181. doi: 10.1016/s0009-8981(98)00014-x. [DOI] [PubMed] [Google Scholar]
- 4.Bognolo DA, Rabow FI, Vijayanagar RR, Eckstein PF. Traumatic sinus node dysfunction. Ann Emerg Med. 1982;11:319–321. doi: 10.1016/s0196-0644(82)80133-9. [DOI] [PubMed] [Google Scholar]
- 5.Pretre R, Chilcott M. Blunt trauma to the heart and great vessels. N Engl J Med. 1997;336:626–632. doi: 10.1056/NEJM199702273360906. [DOI] [PubMed] [Google Scholar]
- 6.El-Chami MF, Nicholson W, Helmy T. Blunt cardiac trauma. J Emerg Med. 2008;35:127–133. doi: 10.1016/j.jemermed.2007.03.018. [DOI] [PubMed] [Google Scholar]
- 7.Wisner DH, Reed WH, Riddick RS. Suspected myocardial contusion. Triage and indications for monitoring. Ann Surg. 1990;212:82–86. doi: 10.1097/00000658-199007000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hasegawa T, Yoshimura N, Oka S, Ootaki Y, Toyoda Y, Yamaguchi M. Evaluation of heart fatty acid-binding protein as a rapid indicator for assessment of myocardial damage in pediatric cardiac surgery. J Thorac Cardiovasc Surg. 2004;127:1697–1702. doi: 10.1016/j.jtcvs.2004.02.006. [DOI] [PubMed] [Google Scholar]
- 9.Okamoto F, Sohmiya K, Ohkaru Y, Kawamura K, Asayama K, Kimura H, Nishimura S, Ishii H, Sunahara N, Tanaka T. Human heart-type cytoplasmic fatty acid-binding protein (H-FABP) for the diagnosis of acute myocardial infarction. Clinical evaluation of H-FABP in comparison with myoglobin and creatine kinase isoenzyme MB. Clin Chem Lab Med. 2000;38:231–238. doi: 10.1515/CCLM.2000.034. [DOI] [PubMed] [Google Scholar]
- 10.Kirchhoff C, Leidel BA, Kirchhoff S, Braunstein V, Bogner V, Kreimeier U, Mutschler W, Biberthaler P. Analysis of N-terminal pro-B-type natriuretic peptide and cardiac index in multiple injured patients: a prospective cohort study. Crit Care. 2008;12:R118. doi: 10.1186/cc7013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Qian A, Zhang M, Zhao G. Dynamic detection of N-terminal pro-B-type natriuretic peptide helps to predict the outcome of patients with major trauma. Eur J of Trauma Emerg Surg. 2014;41:57–64. doi: 10.1007/s00068-014-0406-7. [DOI] [PubMed] [Google Scholar]
- 12.Raghavendran K, Davidson BA, Woytash JA, Helinski JD, Marschke CJ, Manderscheid PA, Notter RH, Knight PR. The evolution of isolated bilateral lung contusion from blunt chest trauma in rats: cellular and cytokine responses. Shock. 2005;24:132–138. doi: 10.1097/01.shk.0000169725.80068.4a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Raghavendran K, Davidson BA, Helinski JD, Marschke CJ, Manderscheid P, Woytash JA, Notter RH, Knight PR. A rat model for isolated bilateral lung contusion from blunt chest trauma. Anesth Analg. 2005;101:1482–1489. doi: 10.1213/01.ANE.0000180201.25746.1F. [DOI] [PubMed] [Google Scholar]
- 14.Vougiouklakis T, Peschos D, Doulis A, Batistatou A, Mitselou A, Agnantis NJ. Sudden death from contusion of the right atrium after blunt chest trauma: case report and review of the literature. Injury. 2005;36:213–217. doi: 10.1016/j.injury.2004.03.029. [DOI] [PubMed] [Google Scholar]
- 15.Kaye P, O'Sullivan I. Myocardial contusion: emergency investigation and diagnosis. Emerg Med J. 2002;19:8–10. doi: 10.1136/emj.19.1.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wang ND, Stevens MH, Doty DB, Hammond EH. Blunt chest trauma: an experimental model for heart and lung contusion. J Trauma. 2003;54:744–748. doi: 10.1097/01.TA.0000052362.40754.F2. [DOI] [PubMed] [Google Scholar]
- 17.Pai M. Diagnosis of myocardial contusion after blunt chest trauma using 18F-FDG positron emission tomography. Br J Radiol. 2006;79:264–265. doi: 10.1259/bjr/17221499. [DOI] [PubMed] [Google Scholar]
- 18.Heyes F, Vincent R. Sternal fracture: what investigations are indicated? Injury. 1993;24:113–115. doi: 10.1016/0020-1383(93)90201-g. [DOI] [PubMed] [Google Scholar]
- 19.Salim A, Velmahos GC, Jindal A, Chan L, Vassiliu P, Belzberg H, Asensio J, Demetriades D. Clinically significant blunt cardiac trauma: role of serum troponin levels combined with electrocardiographic findings. J Trauma. 2001;50:237–243. doi: 10.1097/00005373-200102000-00008. [DOI] [PubMed] [Google Scholar]
- 20.Velmahos GC, Karaiskakis M, Salim A, Toutouzas KG, Murray J, Asensio J, Demetriades D. Normal electrocardiography and serum troponin I levels preclude the presence of clinically significant blunt cardiac injury. J Trauma. 2003;54:45–50. doi: 10.1097/00005373-200301000-00006. discussion 50-41. [DOI] [PubMed] [Google Scholar]
- 21.Fabian TC, Mangiante EC, Patterson CR, Payne LW, Isaacson ML. Myocardial contusion in blunt trauma: clinical characteristics, means of diagnosis, and implications for patient management. J Trauma. 1988;28:50–57. doi: 10.1097/00005373-198801000-00007. [DOI] [PubMed] [Google Scholar]
- 22.Peek GJ, Firmin RK. Isolated sternal fracture: an audit of 10 years’ experience. Injury. 1995;26:385–388. doi: 10.1016/0020-1383(95)00051-a. [DOI] [PubMed] [Google Scholar]
- 23.Adams JE 3rd, Davila-Roman VG, Bessey PQ, Blake DP, Ladenson JH, Jaffe AS. Improved detection of cardiac contusion with cardiac troponin I. Am Heart J. 1996;131:308–312. doi: 10.1016/s0002-8703(96)90359-2. [DOI] [PubMed] [Google Scholar]
- 24.Meier R, van Griensven M, Pape HC, Krettek C, Chawda M, Seekamp A. Effects of cardiac contusion in isolated perfused rat hearts. Shock. 2003;19:123–126. doi: 10.1097/00024382-200302000-00006. [DOI] [PubMed] [Google Scholar]
- 25.Yasue H, Yoshimura M, Sumida H, Kikuta K, Kugiyama K, Jougasaki M, Ogawa H, Okumura K, Mukoyama M, Nakao K. Localization and mechanism of secretion of B-type natriuretic peptide in comparison with those of A-type natriuretic peptide in normal subjects and patients with heart failure. Circulation. 1994;90:195–203. doi: 10.1161/01.cir.90.1.195. [DOI] [PubMed] [Google Scholar]
- 26.Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, Omland T, Storrow AB, Abraham WT, Wu AH, Clopton P, Steg PG, Westheim A, Knudsen CW, Perez A, Kazanegra R, Herrmann HC, McCullough PA Breathing Not Properly Multinational Study Investigators. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347:161–167. doi: 10.1056/NEJMoa020233. [DOI] [PubMed] [Google Scholar]
- 27.Boomsma F, van den Meiracker AH. Plasma A- and B-type natriuretic peptides: physiology, methodology and clinical use. Cardiovasc Res. 2001;51:442–449. doi: 10.1016/s0008-6363(01)00195-x. [DOI] [PubMed] [Google Scholar]
- 28.Kia M, Cooley A, Rimmer G, MacDonald T, Barber K, Manion P, Shapiro B, Socey J, Iddings D. The efficacy of B-type natriuretic peptide for early identification of blood loss in traumatic injury. Am J Surg. 2006;191:353–357. doi: 10.1016/j.amjsurg.2005.10.033. [DOI] [PubMed] [Google Scholar]
- 29.Stewart D, Waxman K, Brown CA, Schuster R, Schuster L, Hvingelby EM, Kam K, Becerra S. B-type natriuretic peptide levels may be elevated in the critically injured trauma patient without congestive heart failure. J Trauma. 2007;63:747–750. doi: 10.1097/01.ta.0000240458.46050.38. [DOI] [PubMed] [Google Scholar]