

Abstract
Background
Non-AIDS-defining cancers increasingly contribute to mortality among human immunodeficiency virus (HIV)-infected individuals. However, few studies have compared cancer prognosis by HIV status with adjustment for risk factors.
Methods
We conducted a cohort study of HIV-infected and HIV-uninfected adults in Kaiser Permanente California during 1996–2011, following subjects diagnosed with Hodgkin lymphoma (HL) or anal, prostate, colorectal, or lung cancers. We used Kaplan-Meier curves and Cox regression to assess cancer-related mortality within five years, comparing HIV-infected with HIV-uninfected subjects. Adjusted models included age, race/ethnicity, sex, cancer stage, cancer treatment, and smoking.
Results
Among HIV-infected and HIV-uninfected subjects, there were 68 and 51 cases of HL, 120 and 28 of anal cancer, 150 and 2050 of prostate cancer, 53 and 646 of colorectal cancer, and 80 and 507 of lung cancer, respectively. Five-year cancer-related survival was reduced for HIV-infected compared with HIV-uninfected subjects, reaching statistical significance for lung cancer (10% vs. 19%, P=0.002) but not HL (83% vs. 89%, P=0.40) or anal (64% vs. 74%, P=0.38), prostate (86% vs. 92%, P=0.074), or colorectal cancers (49% vs. 58%, P=0.55). Adjusted results were similar, with lung cancer (hazard ratio [HR] 1.3, 95% confidence interval [CI]: 1.0–1.7) and prostate cancer (HR 2.1, 95% CI: 1.1–4.1) reaching significance.
Conclusions
Cancer-related mortality was higher among HIV-infected compared with HIV-uninfected individuals for prostate and lung cancers, but not HL, anal cancer, or colorectal cancer.
Impact
Our findings emphasize the need for a focus on prevention, early detection, and adequate treatment of cancer among HIV-infected individuals.
Keywords: cancer, prognosis, human immunodeficiency virus (HIV), immunodeficiency, anal cancer, lung cancer, colorectal cancer, Hodgkin lymphoma, prostate cancer
INTRODUCTION
Advances in combination antiretroviral therapy (ART) have precipitated a steep decline in AIDS-defining cancers among human immunodeficiency virus (HIV)-infected individuals in developed countries. (1) However, as life expectancy for this population has increased, non-AIDS-defining cancers (NADC)(2–5) increasingly contribute to morbidity and mortality. Incidence of many NADCs is higher among HIV-infected compared with HIV-uninfected individuals, particularly for cancers associated with viral infections, such as anal cancer and Hodgkin lymphoma (HL), or cancers associated with smoking, such as lung cancer. (2,3,5–7) Although several studies have described survival after NADC diagnosis in cohorts of HIV-infected individuals in the combination ART era, (8–12) few have directly compared cancer survival between HIV-infected and HIV-uninfected individuals with adjustment for risk factors.
Of studies comparing cancer prognosis by HIV status, HIV infection has been associated with increased mortality from multiple NADCs, including HL (13–15) and lung, (13,14,16,17) colorectal, (13,14) anal, (14,18) and prostate (14) cancers. However, while mortality from AIDS and other causes may result in reduced survival for HIV-infected individuals, few studies have examined cancer-specific mortality (16); furthermore, several were conducted among individuals living with AIDS, (13,14) who are at particularly high risk of death from non-cancer causes. Despite differences by HIV status in mortality risk factors, such as smoking (19,20) and cancer treatment (21,22), few studies have had available data or adequate sample size to adjust for these factors in analyses of individual cancers. (16,17) Finally, cancers may be diagnosed at a more advanced stage or earlier age among HIV-infected individuals; (23,24) although most studies of cancer prognosis have adjusted for age at diagnosis, few have adjusted for stage in analyses of individual cancers. (16,17)
In this study, we evaluated the association of HIV infection with age and cancer stage at diagnosis and initial cancer treatment among HIV-infected and HIV-uninfected individuals diagnosed with NADCs within the same healthcare system, focusing on cancers that are commonly observed among HIV-infected individuals. We then assessed the role of HIV infection in cancer-related mortality after adjustment for age and cancer stage at diagnosis, cancer treatment, smoking, and other mortality risk factors.
MATERIALS AND METHODS
Study Design, Setting, and Population
The study population of HIV-infected and HIV-uninfected subjects with cancer diagnoses was ascertained from a previously described cohort. (25) Briefly, the source cohort consisted of 24,768 HIV-infected and 257,600 demographically matched HIV-uninfected individuals within Kaiser Permanente (KP) Northern and Southern California (KPNC and KPSC, respectively), identified and followed from 1996 through 2011. HIV-infected subjects were identified using HIV registries including all known cases of HIV/AIDS since the early 1980s for KPNC and 2000 for KPSC, with HIV-infected status confirmed by review of medical charts or medical center case lists. Individuals not included in the registries were considered HIV-uninfected. HIV-uninfected subjects were frequency-matched 10:1 to HIV-infected subjects on year and age at start of follow-up (five-year age groups), sex, and medical center.
For the present study, subjects with incident diagnoses of HL or anal, prostate, colorectal, or lung cancers were selected from the source cohort. We focused on these cancers because they are the most commonly diagnosed NADCs among HIV-infected KP members; (25) there were insufficient cases to analyze cancers that are less prevalent in this population, such as melanoma, oral cancer, or liver cancer. For each cancer of interest, individuals were selected at the time of their first cancer diagnosis during the study period. Individuals with any of the five cancer diagnoses in the two years prior to study entry were considered prevalent cases and excluded. Analyses of age, stage at diagnosis, and treatment included all cases diagnosed during 1996–2011. For survival analyses, subjects were followed from cancer diagnosis until the earliest of cancer-related death, death from other causes, five years past the cancer diagnosis, or December 31, 2010 (the latest date for which data were available on cause of death).
The institutional review boards at KPNC and KPSC approved this study with a waiver of written informed consent.
Data Sources
Cancer registries
Cancer diagnoses were ascertained from the KP cancer registries, which are contributing sites to the Surveillance, Epidemiology, and End Results (SEER) program registry. KP cancer registries use standardized methods for verifying and coding all new reportable cancers to ensure accuracy and completeness for reporting to SEER-affiliated regional registries. (26) Data were also extracted on tumor, nodes, metastasis (TNM) stage, SEER summary stage, histologic type, and cancer treatments initiated within six months after diagnosis.
HIV registries
The primary exposure of interest was HIV status, obtained from the KP HIV registries. Other data obtained from the HIV registries included race/ethnicity, CD4 count, and HIV-transmission risk factor.
Electronic medical record (EMR)
The primary outcome of interest was cancer-related death within five years after cancer diagnosis (International Classification of Disease codes, version 9: 140–239; ICD-10: C00-D489), obtained from the clinical and administrative databases constituting KP’s EMR. Dates and causes of death were extracted from hospital records, California death certificates, and Social Security Administration datasets, with complete ascertainment of deaths regardless of KP membership status. Given the limitations of death certificate data, our outcome included deaths from any cancer to account for the potential misclassification of deaths attributed to another cancer site (e.g., death from metastatic disease). This method has been used previously to account for the underestimation of mortality that may occur when only site-specific cancer deaths are analyzed. (27) Other data extracted from the EMR included age; race/ethnicity; health plan enrollment periods; and clinical diagnoses of smoking/tobacco use (ICD-9: 305.1, V15, V65, 649, internal social history codes). Subjects without a smoking diagnosis were considered non-smokers.
Statistical Analysis
Variables considered in the analysis included age (<40, 40–49, 50–64, ≥65 years), race/ethnicity (white, black/African American, Hispanic/Latino, Asian/Pacific Islander, other), smoking (ever/never), TNM stage (Stage I–IV), SEER summary stage (localized, regional, distant), and cancer treatment (radiation, chemotherapy, surgery, or any treatment). Among HIV-infected subjects, we considered HIV-transmission risk factor (men who have sex with men [MSM], heterosexual sex, injection drug use, unknown) and CD4 count from the six months prior to cancer diagnosis.
We compared demographic and clinical characteristics of HIV-infected and HIV-uninfected cancer cases, using t-tests for continuous variables and chi-square or Fisher exact tests for categorical variables. For analyses of anal and prostate cancers, TNM stage was categorized as Stage I–III vs. IV to reflect the staging commonly used in clinical practice at KP. Surgery is rarely used for treatment of HL and chemotherapy is not a standard treatment for prostate cancer; thus, those treatments were not assessed for those cancer types. We compared five-year survival by HIV status using Kaplan-Meier curves and log-rank tests. Subjects were censored if they died from non-cancer-related causes; thus, the survival curves are interpreted as the theoretical probability of dying from cancer-related causes if no subjects died of non-cancer-related causes. Hazard ratios (HR) for cancer-related mortality were obtained from Cox regression models comparing HIV-infected to HIV-uninfected subjects. Demographics-adjusted models included variables for age, race/ethnicity, and sex, while fully adjusted models additionally included TNM stage, cancer treatment type, and smoking.
Analyses were conducted in SAS 9.1 (Cary, NC). Statistical tests were two-sided and statistical significance was defined as P<0.05.
RESULTS
Study Population
Among HIV-infected and HIV-uninfected subjects, there were 120 and 28 cases of anal cancer, 150 and 2050 of prostate cancer, 53 and 646 of colorectal cancer, 80 and 507 of lung cancer, and 68 and 51 of HL, respectively. Subjects were mostly men overall, with a higher proportion of men among HIV-infected compared with HIV-uninfected subjects with anal cancer (P<0.001), and a lower proportion among HIV-infected subjects with colorectal cancer (P=0.032; Table 1). The distribution of race/ethnicity differed by HIV status for prostate cancer (P=0.003) and lung cancer (P=0.006), with a higher proportion of white subjects among HIV-infected compared with HIV-uninfected individuals. Among HIV-infected subjects, MSM was the most common HIV-transmission risk factor for all cancers, reflecting the epidemic in California.
Table 1.
Demographic characteristics of cancer cases by HIV status, 1996–2011.
| Anal cancer | Prostate cancer | Colorectal cancer | Lung cancer | Hodgkin lymphoma | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HIV+ | HIV− | P | HIV+ | HIV− | P | HIV+ | HIV− | P | HIV+ | HIV− | P | HIV+ | HIV− | P | |
| N | 120 | 28 | 150 | 2050 | 53 | 646 | 80 | 507 | 68 | 51 | |||||
| Men, % | 99 | 79 | <0.001 | 100 | 100 | – | 85 | 93 | 0.032 | 95 | 93 | 0.52 | 93 | 94 | 0.75 |
| Mean age, years | 52 | 56 | 0.019 | 59 | 60 | 0.17 | 53 | 58 | 0.002 | 56 | 61 | <0.001 | 47 | 45 | 0.45 |
| Race/ethnicity, % | 0.12 | 0.003 | 0.16 | 0.006 | 0.58 | ||||||||||
| White | 70 | 79 | 56 | 51 | 62 | 47 | 74 | 53 | 62 | 63 | |||||
| African American/Black | 16 | 4 | 31 | 23 | 19 | 16 | 17 | 15 | 10 | 12 | |||||
| Hispanic | 13 | 14 | 12 | 14 | 15 | 17 | 4 | 12 | 25 | 20 | |||||
| Asian/Pacific Islander | 0 | 4 | 1 | 9 | 4 | 17 | 5 | 18 | 1 | 6 | |||||
| Other | 1 | 0 | 0 | 2 | 0 | 3 | 0 | 2 | 1 | 0 | |||||
| HIV-transmission risk factor, % | |||||||||||||||
| MSM | 76 | – | 65 | – | 55 | – | 65 | – | 59 | – | |||||
| Heterosexual sex | 5 | – | 11 | – | 15 | – | 16 | – | 18 | – | |||||
| Injection drug use | 2 | – | 4 | – | 6 | – | 5 | – | 1 | – | |||||
| Other/unknown | 18 | – | 21 | – | 25 | – | 14 | – | 22 | – | |||||
MSM, men who have sex with men.
Age and Stage at Diagnosis by HIV Status
Compared with HIV-uninfected subjects, HIV-infected subjects were younger when diagnosed with anal (52 vs. 56 years, P=0.019), colorectal (53 vs. 58 years, P=0.002), and lung cancers (56 vs. 61 years, P<0.001), while age was similar by HIV status for prostate cancer and HL (Table 1). TNM and SEER summary stage were similar by HIV status for anal, colorectal, and lung cancers (Table 2). However, compared with HIV-uninfected subjects, HIV-infected subjects with HL were more frequently diagnosed with Stage IV disease (54% vs. 28%, P=0.007). For prostate cancer, HIV-infected subjects were more frequently diagnosed with localized disease (89% vs. 83%, P=0.023), but there were no differences in TNM stage by HIV status.
Table 2.
Clinical characteristics of cancer cases by HIV status, 1996–2011.
| Anal cancer | Prostate cancer | Colorectal cancer | Lung cancer | Hodgkin lymphoma | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HIV+ | HIV− | P | HIV+ | HIV− | P | HIV+ | HIV− | P | HIV+ | HIV− | P | HIV+ | HIV− | P | |
| Cancer cases, N | 120 | 28 | 150 | 2050 | 53 | 646 | 80 | 507 | 68 | 51 | |||||
| Deaths, n | |||||||||||||||
| Cancer-related causes | 27 | 5 | 9 | 71 | 12 | 156 | 58 | 298 | 9 | 4 | |||||
| Other causes | 17 | 1 | 5 | 59 | 7 | 36 | 11 | 54 | 14 | 2 | |||||
| TNM stage, % among known | 0.69 | 0.77 | 0.28 | 0.41 | 0.007 | ||||||||||
| I | 93 | 96 | 95 | 94 | 37 | 25 | 11 | 16 | 9 | 24 | |||||
| II | 22 | 26 | 4 | 6 | 16 | 32 | |||||||||
| III | 16 | 25 | 22 | 25 | 21 | 16 | |||||||||
| IV | 7 | 4 | 5 | 6 | 24 | 24 | 63 | 54 | 54 | 28 | |||||
| Unknown TNM stage, % | 11 | 18 | 0.31 | 7 | 10 | 0.31 | 8 | 7 | 0.84 | 5 | 3 | 0.46 | 1 | 2 | 0.84 |
| SEER summary stage | 0.40 | 0.023 | 0.78 | 0.21 | 0.004 | ||||||||||
| Localized | 58 | 70 | 89 | 83 | 45 | 41 | 10 | 14 | 9 | 24 | |||||
| Regional | 36 | 22 | 6 | 14 | 31 | 36 | 17 | 23 | 18 | 32 | |||||
| Distant | 6 | 7 | 5 | 3 | 24 | 23 | 73 | 63 | 74 | 44 | |||||
| Any cancer treatment | 95 | 93 | 0.65 | 57 | 59 | 0.54 | 92 | 93 | 0.98 | 64 | 76 | 0.023 | 81 | 86 | 0.44 |
| Radiation | 49 | 61 | 0.27 | 31 | 18 | <0.001 | 21 | 15 | 0.27 | 24 | 28 | 0.43 | 7 | 27 | 0.003 |
| Chemotherapy | 66 | 64 | 0.88 | – | – | – | 42 | 47 | 0.44 | 39 | 49 | 0.08 | 81 | 82 | 0.84 |
| Surgery | 45 | 50 | 0.63 | 25 | 42 | <0.001 | 70 | 86 | 0.002 | 16 | 28 | 0.027 | – | – | – |
| Mean CD4 cells/μL | 427 | – | – | 554 | – | – | 418 | – | – | 400 | – | – | 294 | – | – |
SD, standard deviation; TNM, tumor, nodes, metastasis; SEER, Surveillance, Epidemiology, and End Results. TNM stage was categorized as Stage I-III vs. IV for anal and prostate cancers to reflect the staging most commonly used in clinical practice. Surgery is not used for treatment of Hodgkin lymphoma, and chemotherapy is not used for treatment of prostate cancer; thus, those treatments were not assessed for those cancer types.
Cancer Treatment by HIV Status
The proportion receiving any cancer treatment within six months of diagnosis was lower for HIV-infected compared with HIV-uninfected subjects with lung cancer (64% vs. 76%, P=0.023), but similar by HIV status for all other cancers (Table 2). There were no differences in cancer treatment type by HIV status for anal cancer. However, for prostate cancer, HIV-infected subjects more frequently received radiation compared with HIV-uninfected subjects (31% vs. 18%, P<0.001). Compared with HIV-uninfected subjects, HIV-infected subjects less frequently received surgery for prostate cancer (25% vs. 42%, P<0.001), colorectal cancer (70% vs. 86%, P=0.002), and lung cancer (16% vs. 28%, P=0.027). For HL, HIV-infected subjects less frequently received radiation compared with HIV-uninfected subjects (7% vs. 27%, P=0.003).
Cancer Mortality by HIV Status
The number of deaths from cancer-related and other causes is shown in Table 2. Compared with HIV-uninfected subjects, five-year survival was reduced for HIV-infected subjects with cancer, reaching statistical significance for lung cancer (10% vs. 19%, P=0.002), but not anal cancer (64% vs. 74%, P=0.38), prostate cancer (86% vs. 92%, P=0.074), colorectal cancer (49% vs. 58%, P=0.55), or HL (83% vs. 89%, P=0.40; Figure 1). After adjustment for age, race/ethnicity, sex, TNM stage, cancer treatment type, and smoking, cancer-related mortality was higher among HIV-infected compared with HIV-uninfected subjects for all cancers, reaching statistical significance for prostate cancer (HR 2.1, 95% confidence interval [CI]: 1.1–4.1) and lung cancer (HR 1.3, 95% CI: 1.0–1.7), but not anal cancer (HR 1.6, 95% CI: 0.4–6.6), colorectal cancer (HR 1.4, 95% CI: 0.8–2.7), or HL (HR 2.1, 95% CI: 0.7–6.4; Table 3).
Figure 1. Five-year survival after cancer diagnosis by HIV status, 1996–2010.
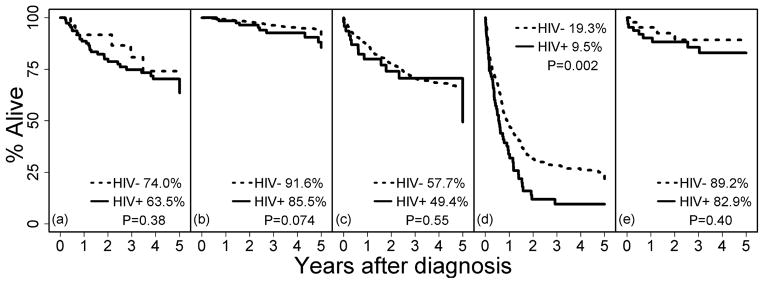
Kaplan-Meier curves show the cumulative proportion alive in the five years after cancer diagnosis by HIV status, with subjects censored if they died of non-cancer-related causes. Overall, 3,342 HIV-infected and 2,911 HIV-uninfected individuals contributed to the plots. Panels are as follows: (a) anal cancer, (b) prostate cancer, (c) colorectal cancer, (d) lung cancer, and (e) Hodgkin lymphoma. P-values are from log-rank tests.
Table 3.
Hazard ratios for cancer-related mortality within five years of cancer diagnosis by HIV status, 1996–2010.
| Unadjusted | Demographics-adjusted | Fully adjusted | ||||
|---|---|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | HR (95% CI) | P | |
| Anal cancer | 2.2 (0.7–7.4) | 0.2 | 1.8 (0.5–6.8) | 0.37 | 1.6 (0.4–6.6) | 0.52 |
| Prostate cancer | 1.8 (0.9–3.4) | 0.08 | 1.9 (1.0–3.6) | 0.06 | 2.1 (1.1–4.1) | 0.02 |
| Colorectal cancer | 1.2 (0.7–2.0) | 0.52 | 1.3 (0.7–2.2) | 0.37 | 1.4 (0.8–2.7) | 0.26 |
| Lung cancer | 1.5 (1.2–2.0) | 0.002 | 1.6 (1.2–2.2) | <0.001 | 1.3 (1.0–1.7) | 0.046 |
| Hodgkin lymphoma | 1.6 (0.5–5.3) | 0.40 | 1.6 (0.5–5.0) | 0.44 | 2.1 (0.7–6.4) | 0.21 |
HRs from Cox models with HIV-uninfected reference group. Demographics-adjusted models included age, race/ethnicity, and sex. Fully adjusted models additionally included tumor, nodes, metastasis stage; cancer treatment type; and smoking.
Among individuals with lung cancer, the most common histologic subtype was adenocarcinoma (40%), followed by squamous carcinoma (17%) and large cell carcinoma (11%), with no difference in the distribution of histologic type by HIV status (P=0.76). Among the 535 (92%) individuals with non-small cell carcinoma, five-year survival was lower among HIV-infected compared with HIV-uninfected individuals (8.5% vs. 21%, P=0.001). Five-year survival was similar among HIV-infected compared with HIV-uninfected individuals with small-cell carcinoma (33% vs. 0%, P=0.95); however, there were only 6 cases of this histologic type among HIV-infected individuals.
DISCUSSION
In this large cohort study, HIV-infected individuals were diagnosed at an earlier age for anal, colorectal, and lung cancers, and a more advanced stage for HL, compared with HIV-uninfected individuals from the same healthcare system. Five-year survival was lower for HIV-infected compared with HIV-uninfected individuals for all NADCs examined, reaching statistical significance for lung cancer. After adjustment for age, race/ethnicity, sex, stage, cancer treatment, and smoking, HIV-infected individuals were at significantly higher risk of cancer-related mortality after diagnosis with lung cancer or prostate cancer, but not HL, anal cancer, or colorectal cancer.
Our study is consistent with prior studies finding reduced survival among HIV-infected individuals diagnosed with lung and prostate cancers, (13,14,16,17) with several finding increased mortality independent of disease stage at diagnosis. (16,17) Among injection drug users, Shiels et al. found a nearly four-fold higher risk of death after diagnosis with lung cancer among HIV-infected compared with HIV-uninfected individuals after adjustment for SEER summary stage and smoking, although with 29 cases this did not reach statistical significance. (16) Sigel et al. also found an association of HIV infection and non-small cell lung cancer mortality after adjustment for SEER summary stage and competing risks of death. (17) While Rengan et al. found no differences in non-small cell lung cancer survival by HIV status in the same study population after adjustment for TNM stage, (28) HIV status may have been misclassified in this study such that differences in survival were attenuated; furthermore, Rengan et al. did not adjust for smoking, which is more prevalent among HIV-infected individuals compared with the general population. (19,20) In our study, reduced survival for lung and prostate cancers among HIV-infected individuals was not fully explained by TNM stage, smoking, or the other risk factors evaluated, and survival curves demonstrated higher cancer-related mortality for HIV-infected individuals for all NADCs examined. These results suggest an independent effect of HIV infection on cancer survival. The mechanisms for reduced survival after lung and prostate cancer diagnosis among HIV-infected individuals may be similar to those that explain higher NADC incidence in this population, including immunodeficiency, (29,30) chronic immune activation and inflammation, (31,32) activation of proto-oncogenes, (33) inhibition of tumor suppressor genes, (34) or endothelial abnormalities that enhance tumor development and progression. (35)
While several studies have identified an earlier age at NADC diagnosis for HIV-infected individuals compared with the general population, (36–39) few have accounted for differences in the underlying age distributions of these two populations. Shiels et al. adjusted for age in a registry-based study, (39) while our study matched HIV-uninfected to HIV-infected subjects on age. Similar to our study, Shiels et al. found that individuals with AIDS were younger when diagnosed with anal and lung cancers compared with the general population; these comparable results are reassuring, given that our studies used different analytical approaches to remove the potential age bias. In addition to HIV-associated mechanisms that increase incidence and progression of NADCs, earlier age at diagnosis among HIV-infected individuals may be attributable to increased medical surveillance. In this study population, we previously found higher rates of prostate-specific antigen testing, and lower-stage prostate cancers at diagnosis as also presented here, among HIV-infected compared with HIV-uninfected individuals, suggesting an effect of increased cancer screening on the timing of cancer diagnosis among HIV-infected individuals. (40) However, we found no differences in stage by HIV status for cancers detected at a younger age among HIV-infected individuals, suggesting that earlier diagnosis may be attributable to a biological effect rather than differences in screening.
We observed less treatment for HIV-infected individuals with lung cancer, as well as differences in treatment type by HIV status for prostate cancer and HL. These findings are consistent with previous studies finding less treatment among HIV-infected compared with HIV-uninfected individuals with lung cancer, prostate cancer, and HL, with disparities persisting in more recent years. (21,22) In a registry-based study, Suneja et al. found treatment disparities by HIV status for HL, lung, prostate, and colorectal cancers, (21) while we only identified an overall disparity for lung cancer. It may be that treatment disparities by HIV status are explained in part by differences in access to cancer treatment, and were thus less apparent in our study setting of equal access to care. The difference we observed in treatment for lung cancer may be attributable to provider-level factors, such as perceiving HIV-infected individuals as having lower cancer treatment efficacy or tolerability compared with HIV-uninfected individuals. (21) In our study, adjustment for treatment attenuated the elevated cancer mortality risk we observed among HIV-infected individuals with lung cancer, suggesting that treatment disparities may play a role in reduced survival for this cancer.
There are several limitations of our study. First, despite our large cohort, our statistical power was limited. We observed relatively small numbers of HL diagnoses overall and anal cancer diagnoses among HIV-uninfected subjects, which may explain the lack of statistical significance observed for these cancers. Few observed deaths for most cancers may also have limited our ability to detect differences in cancer mortality. Second, because treatment data from the EMR were not comprehensive for all cancer cases and medical centers, we relied on the cancer registries for cancer treatment data. These data may be subject to misclassification and only document treatments initiated within six months after diagnosis. Third, an analysis of cancer recurrence may have strengthened our findings, but these data were not available. Fourth, because data were extracted from the EMR, risk factors such as smoking could not be analyzed in detail. Fifth, diagnosis and surgery may have been more likely to be misclassified for anal cancer than for other cancers because of the high prevalence of precancerous or in situ disease and the use of local treatment for microinvasive disease. Sixth, our survival analysis represented the theoretical scenario in which subjects only died of cancer-related causes; future studies with larger sample sizes should consider approaches accounting for competing risks. However, in this analysis, most deaths were cancer-related. Finally, our subjects were mostly men, limiting the generalizability of our results to women.
Our study also has several strengths. First, cancers were identified from HIV-infected individuals and an internal comparison group of HIV-uninfected individuals from the same healthcare system, in which differences in outcomes were unlikely to be attributable to differential access to care. Second, matching HIV-uninfected to HIV-infected individuals on age allowed us to compare age at diagnosis despite differences in the underlying age distributions of these populations. Third, including data on TNM stage, a more clinically relevant measure of cancer stage than SEER summary stage, we were able to determine that reduced survival for HIV-infected individuals was independent of disease stage. Fourth, the HIV and cancer registries and EMR allowed for near-perfect case ascertainment for HIV infection, cancer, and mortality, with deaths ascertained regardless of KP membership status. Finally, the KP membership mirrors the age, sex, and race/ethnicity distributions of the California statewide population, (41,42) and the demographics of HIV-infected KP members are comparable to those of reported AIDS cases in California. (43) Thus, our results are likely to be generalizable to other individuals with access to healthcare.
In summary, compared with HIV-uninfected individuals in the same healthcare system, HIV-infected individuals were diagnosed at a younger age for anal, colorectal, and lung cancers, and at a more advanced stage for HL. After adjustment for age, sex, race/ethnicity, TNM stage, cancer treatment, and smoking, cancer-related mortality was higher among HIV-infected individuals for lung and prostate cancers. Our findings emphasize the need for a focus on prevention, early detection, and adequate treatment of cancer among HIV-infected individuals, and the evaluation of appropriate cancer screening strategies in this population.
Acknowledgments
Financial support: This work was supported by research grants awarded to M.J. Silverberg by Pfizer Pharmaceuticals and the National Institute of Allergy and Infectious Diseases (K01AI071725).
This work was supported by research grants awarded to Michael J. Silverberg by Pfizer Pharmaceuticals and the National Institute of Allergy and Infectious Diseases (K01AI071725). Parts of this work were previously presented at the 19th Conference on Retroviruses and Opportunistic Infections, Seattle, 2012.
Footnotes
Potential conflicts of interest: This work was supported by a research grant from Pfizer Pharmaceuticals. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
References
- 1.Shiels MS, Pfeiffer RM, Gail MH, Hall HI, Li J, Chaturvedi AK, et al. Cancer burden in the HIV-infected population in the United States. J Natl Cancer Inst. 2011;103:753–62. doi: 10.1093/jnci/djr076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shiels MS, Cole SR, Kirk GD, Poole C. A meta-analysis of the incidence of non-AIDS cancers in HIV-infected individuals. J Acquir Immune Defic Syndr. 2009;52:611–22. doi: 10.1097/QAI.0b013e3181b327ca. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Engels EA, Biggar RJ, Hall HI, Cross H, Crutchfield A, Finch JL, et al. Cancer risk in people infected with human immunodeficiency virus in the United States. Int J Cancer. 2008;123:187–94. doi: 10.1002/ijc.23487. [DOI] [PubMed] [Google Scholar]
- 4.Crum-Cianflone N, Hullsiek KH, Marconi V, Weintrob A, Ganesan A, Barthel RV, et al. Trends in the incidence of cancers among HIV-infected persons and the impact of antiretroviral therapy: a 20-year cohort study. Aids. 2009;23:41–50. doi: 10.1097/QAD.0b013e328317cc2d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Patel P, Hanson DL, Sullivan PS, Novak RM, Moorman AC, Tong TC, et al. Incidence of types of cancer among HIV-infected persons compared with the general population in the United States, 1992–2003. Ann Intern Med. 2008;148:728–36. doi: 10.7326/0003-4819-148-10-200805200-00005. [DOI] [PubMed] [Google Scholar]
- 6.Grulich AE, van Leeuwen MT, Falster MO, Vajdic CM. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis. Lancet. 2007;370:59–67. doi: 10.1016/S0140-6736(07)61050-2. [DOI] [PubMed] [Google Scholar]
- 7.Silverberg MJ, Chao C, Leyden WA, Xu L, Tang B, Horberg MA, et al. HIV infection and the risk of cancers with and without a known infectious cause. Aids. 2009;23:2337–45. doi: 10.1097/QAD.0b013e3283319184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Achenbach CJ, Cole SR, Kitahata MM, Casper C, Willig JH, Mugavero MJ, et al. Mortality after cancer diagnosis in HIV-infected individuals treated with antiretroviral therapy. Aids. 2011;25:691–700. doi: 10.1097/QAD.0b013e3283437f77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Worm SW, Bower M, Reiss P, Bonnet F, Law M, Fatkenheuer G, et al. Non-AIDS defining cancers in the D:A:D Study--time trends and predictors of survival: a cohort study. BMC Infect Dis. 2013;13:471. doi: 10.1186/1471-2334-13-471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Long JL, Engels EA, Moore RD, Gebo KA. Incidence and outcomes of malignancy in the HAART era in an urban cohort of HIV-infected individuals. Aids. 2008;22:489–96. doi: 10.1097/QAD.0b013e3282f47082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Spagnuolo V, Galli L, Salpietro S, Gianotti N, Guffanti M, Cossarini F, et al. Ten-year survival among HIV-1-infected subjects with AIDS or non-AIDS-defining malignancies. Int J Cancer. 2012;130:2990–6. doi: 10.1002/ijc.26332. [DOI] [PubMed] [Google Scholar]
- 12.Gotti D, Raffetti E, Albini L, Sighinolfi L, Maggiolo F, Di Filippo E, et al. Survival in HIV-infected patients after a cancer diagnosis in the cART Era: results of an italian multicenter study. PLoS One. 2014;9:e94768. doi: 10.1371/journal.pone.0094768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Maso LD, Suligoi B, Franceschi S, Braga C, Buzzoni C, Polesel J, et al. Survival after cancer in italian persons with AIDS, 1986–2005: a population-based estimation. J Acquir Immune Defic Syndr. 2014;66:428–35. doi: 10.1097/QAI.0000000000000184. [DOI] [PubMed] [Google Scholar]
- 14.Biggar RJ, Engels EA, Ly S, Kahn A, Schymura MJ, Sackoff J, et al. Survival after cancer diagnosis in persons with AIDS. J Acquir Immune Defic Syndr. 2005;39:293–9. doi: 10.1097/01.qai.0000164033.02947.e3. [DOI] [PubMed] [Google Scholar]
- 15.Coghill AE, Newcomb PA, Madeleine MM, Richardson BA, Mutyaba I, Okuku F, et al. Contribution of HIV infection to mortality among cancer patients in Uganda. Aids. 2013 doi: 10.1097/01.aids.0000433236.55937.cb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Shiels MS, Cole SR, Mehta SH, Kirk GD. Lung cancer incidence and mortality among HIV-infected and HIV-uninfected injection drug users. J Acquir Immune Defic Syndr. 2010;55:510–5. doi: 10.1097/QAI.0b013e3181f53783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sigel K, Crothers K, Dubrow R, Krauskopf K, Jao J, Sigel C, et al. Prognosis in HIV-infected patients with non-small cell lung cancer. Br J Cancer. 2013;109:1974–80. doi: 10.1038/bjc.2013.545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Legarth R, Helleberg M, Kronborg G, Larsen CS, Pedersen G, Pedersen C, et al. Anal carcinoma in HIV-infected patients in the period 1995–2009: a Danish nationwide cohort study. Scandinavian journal of infectious diseases. 2013;45:453–9. doi: 10.3109/00365548.2012.737476. [DOI] [PubMed] [Google Scholar]
- 19.Browning KK, Wewers ME, Ferketich AK, Diaz P. Tobacco use and cessation in HIV-infected individuals. Clin Chest Med. 2013;34:181–90. doi: 10.1016/j.ccm.2013.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tesoriero JM, Gieryic SM, Carrascal A, Lavigne HE. Smoking among HIV positive New Yorkers: prevalence, frequency, and opportunities for cessation. AIDS Behav. 2010;14:824–35. doi: 10.1007/s10461-008-9449-2. [DOI] [PubMed] [Google Scholar]
- 21.Suneja G, Shiels MS, Angulo R, Copeland GE, Gonsalves L, Hakenewerth AM, et al. Cancer Treatment Disparities in HIV-Infected Individuals in the United States. J Clin Oncol. 2014;32:2344–50. doi: 10.1200/JCO.2013.54.8644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Suneja G, Shiels MS, Melville SK, Williams MA, Rengan R, Engels EA. Disparities in the treatment and outcomes of lung cancer among HIV-infected individuals. Aids. 2013;27:459–68. doi: 10.1097/QAD.0b013e32835ad56e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cutrell J, Bedimo R. Non-AIDS-defining cancers among HIV-infected patients. Curr HIV/AIDS Rep. 2013;10:207–16. doi: 10.1007/s11904-013-0166-8. [DOI] [PubMed] [Google Scholar]
- 24.Deeken JF, Tjen ALA, Rudek MA, Okuliar C, Young M, Little RF, et al. The rising challenge of non-AIDS-defining cancers in HIV-infected patients. Clin Infect Dis. 2012;55:1228–35. doi: 10.1093/cid/cis613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Silverberg MJ, Chao C, Leyden WA, Xu L, Horberg MA, Klein D, et al. HIV infection, immunodeficiency, viral replication, and the risk of cancer. Cancer Epidemiol Biomarkers Prev. 2011;20:2551–9. doi: 10.1158/1055-9965.EPI-11-0777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Adamo M, Dickie L, Ruhl J. Institute NC, editor. 2014 SEER Program Coding and Staging Manual. Bethesda, MD: 2014. [Google Scholar]
- 27.Howlader N, Ries LA, Mariotto AB, Reichman ME, Ruhl J, Cronin KA. Improved estimates of cancer-specific survival rates from population-based data. J Natl Cancer Inst. 2010;102:1584–98. doi: 10.1093/jnci/djq366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rengan R, Mitra N, Liao K, Armstrong K, Vachani A. Effect of HIV on survival in patients with non-small-cell lung cancer in the era of highly active antiretroviral therapy: a population-based study. Lancet Oncol. 2012;13:1203–9. doi: 10.1016/S1470-2045(12)70466-7. [DOI] [PubMed] [Google Scholar]
- 29.Reekie J, Kosa C, Engsig F, Monforte A, Wiercinska-Drapalo A, Domingo P, et al. Relationship between current level of immunodeficiency and non-acquired immunodeficiency syndrome-defining malignancies. Cancer. 2010;116:5306–15. doi: 10.1002/cncr.25311. [DOI] [PubMed] [Google Scholar]
- 30.Kesselring A, Gras L, Smit C, van Twillert G, Verbon A, de Wolf F, et al. Immunodeficiency as a risk factor for non-AIDS-defining malignancies in HIV-1-infected patients receiving combination antiretroviral therapy. Clin Infect Dis. 2011;52:1458–65. doi: 10.1093/cid/cir207. [DOI] [PubMed] [Google Scholar]
- 31.Schottenfeld D, Beebe-Dimmer J. Chronic inflammation: a common and important factor in the pathogenesis of neoplasia. CA Cancer J Clin. 2006;56:69–83. doi: 10.3322/canjclin.56.2.69. [DOI] [PubMed] [Google Scholar]
- 32.Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140:883–99. doi: 10.1016/j.cell.2010.01.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Guo HG, Pati S, Sadowska M, Charurat M, Reitz M. Tumorigenesis by human herpesvirus 8 vGPCR is accelerated by human immunodeficiency virus type 1 Tat. J Virol. 2004;78:9336–42. doi: 10.1128/JVI.78.17.9336-9342.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Harrod R, Nacsa J, Van Lint C, Hansen J, Karpova T, McNally J, et al. Human immunodeficiency virus type-1 Tat/co-activator acetyltransferase interactions inhibit p53Lys-320 acetylation and p53-responsive transcription. J Biol Chem. 2003;278:12310–8. doi: 10.1074/jbc.M211167200. [DOI] [PubMed] [Google Scholar]
- 35.Corallini A, Campioni D, Rossi C, Albini A, Possati L, Rusnati M, et al. Promotion of tumour metastases and induction of angiogenesis by native HIV-1 Tat protein from BK virus/tat transgenic mice. Aids. 1996;10:701–10. doi: 10.1097/00002030-199606001-00003. [DOI] [PubMed] [Google Scholar]
- 36.Brock MV, Hooker CM, Engels EA, Moore RD, Gillison ML, Alberg AJ, et al. Delayed diagnosis and elevated mortality in an urban population with HIV and lung cancer: implications for patient care. J Acquir Immune Defic Syndr. 2006;43:47–55. doi: 10.1097/01.qai.0000232260.95288.93. [DOI] [PubMed] [Google Scholar]
- 37.Demopoulos BP, Vamvakas E, Ehrlich JE, Demopoulos R. Non-acquired immunodeficiency syndrome-defining malignancies in patients infected with human immunodeficiency virus. Arch Pathol Lab Med. 2003;127:589–92. doi: 10.5858/2003-127-0589-NISMIP. [DOI] [PubMed] [Google Scholar]
- 38.Chapman C, Aboulafia DM, Dezube BJ, Pantanowitz L. Human immunodeficiency virus-associated adenocarcinoma of the colon: clinicopathologic findings and outcome. Clin Colorectal Cancer. 2009;8:215–9. doi: 10.3816/CCC.2009.n.036. [DOI] [PubMed] [Google Scholar]
- 39.Shiels MS, Pfeiffer RM, Engels EA. Age at cancer diagnosis among persons with AIDS in the United States. Ann Intern Med. 2010;153:452–60. doi: 10.1059/0003-4819-153-7-201010050-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Marcus JL, Chao CR, Leyden WA, Xu L, Klein DB, Horberg MA, et al. Prostate Cancer Incidence and Prostate-Specific Antigen Testing Among HIV-Positive and HIV-Negative Men. J Acquir Immune Defic Syndr. 2014;66:495–502. doi: 10.1097/QAI.0000000000000202. [DOI] [PubMed] [Google Scholar]
- 41.Koebnick C, Langer-Gould AM, Gould MK, Chao CR, Iyer RL, Smith N, et al. Sociodemographic characteristics of members of a large, integrated health care system: comparison with US Census Bureau data. Perm J. 2012;16:37–41. doi: 10.7812/tpp/12-031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Gordon N. How Does the Adult Kaiser Permanente Membership in Northern California Compare with the Larger Community? [Internet]. 2006 [cited 2015 Jan 29]. Available from: < http://www.dor.kaiser.org/external/uploadedFiles/content/research/mhs/_2011_Revised_Site/Documents_Special_Reports/comparison_kaiser_vs_nonKaiser_adults_kpnc(1).pdf>.
- 43.California Department of Public Health, Office of AIDS. 2010 Quarterly HIV/AIDS Statistics. 2010 [Internet] [cited 2015 Jan 29]. Available from: < http://www.cdph.ca.gov/data/statistics/Pages/OA2010QtrlyStats.aspx>.