

Abstract
Background
GATS India 2009–10 revealed that more than one-third (35%) of adults in India use tobacco in some form: 21% use smokeless tobacco, 9% smoke, and 5% are mixed users (they smoke and use smokeless tobacco), and the quit rate is very low. In an effort to decrease prevalence of tobacco use, it is thus important to understand the factors that are related to intention to quit among Indian tobacco users. Research has shown consistently that intention to quit is a strong predictor of future quitting. The present study reports the factors encouraging quitting tobacco products in India.
Methods
Cross-sectional data from Wave 1 of the International Tobacco Control Policy Evaluation (TCP) India Survey conducted in four cities and surrounding rural areas [i.e. Mumbai (Maharashtra), Patna (Bihar), Indore (Madhya Pradesh), and Kolkata (West Bengal)] between August 2010 and December 2011 were analyzed. A total of 8,051 tobacco users (15+ years) were randomly sampled from 8,586 households: 1,255 smokers, 5,991 smokeless users, and 805 mixed (smoke and smokeless) users. Validated, standardized questions were asked about current tobacco use, intention to quit, and factors encouraging quitting.
Results
Overall, 19.6% of tobacco users intended to quit. Smokers had less intention to quit as compared to smokeless tobacco users whereas mixed users had more intention to quit (OR = 1.48, 95% CI = 1.12–1.97) compared to smokeless tobacco users. Highly educated people were more likely to report intention to quit (OR = 1.82, 95% CI = 1.09–3.02) compared to less educated. Advice by doctors to quit tobacco had a strong impact on intention to quit (OR = 1.68, CI = 1.29–2.15). Tobacco users who were exposed to anti-tobacco messages at work places (OR = 1.74, CI = 1.23–2.46), at restaurants (OR = 1.65, CI = 1.12–2.43), bars (OR = 1.81, CI = 1.07–3.06), on public transportation (OR = 2.14, CI = 1.49–3.08) and on tobacco packages (OR = 1.77, CI = 1.29–2.14) also expressed greater intention to quit tobacco use.
Conclusion
Around one-fifth of tobacco users in India intended to quit tobacco use. Higher education, doctor’s advice, and anti-tobacco messages were positively associated with users’ intention to quit tobacco.
Keywords: Intention to quit, TCP India, Reasons for quitting, factors associated with quitting, doctor’s advice, anti-tobacco messages
Introduction
One of the leading preventable causes of death is tobacco use. Worldwide, it will kill more than eight million people by 2030.1 Still, in India, around two in every five adults from rural areas and one in every four adults from urban areas use tobacco in some form.1
Quitting tobacco use at any age will help in improving the quality of health. After quitting tobacco, the risk of death decreases immediately. The survival rate becomes about the same as that for non-smokers, if a tobacco user quits before the age of 35 years. Former smokers live longer than ongoing smokers, no matter at what age they stop smoking, though the impact is greatest for quitting at younger ages.2
Despite the clear benefits of quitting, according to India Global Tobacco Adult Survey (GATS) 2009–10 results, the quit rate is very low in India, with only two out of five tobacco users having made any attempts to quit tobacco.3 Evidence shows that tobacco users are aware of the health benefits of quitting tobacco and express a desire to quit, but the majorities are unsuccessful in their quit attempts.4 Earlier research shows that intention to quit is a strong predictor of future quitting.5 Because of the strength of quit intentions as a precursor to an actual quit attempt, many studies have focused on identified variables that are related to quit intentions.5 Also, most studies reported thus far have been from high-income countries6, and it is unclear to what extent those findings can be generalized to developing nations that show different patterns of tobacco use and socio-cultural influences. For example, findings from the International Tobacco Control (ITC) Survey in Malaysia and Thailand show that the determinants of quitting were only partially consistent with those found in Western countries.7 It is therefore questionable whether the same factors would apply to India.
There has been little research on quit intentions and the predictors of successful tobacco cessation in India. Two studies have reported self-motivation as an important predictor to successful tobacco cessation.8–9 Further, an intervention study of tobacco users in rural areas in Kerala, India demonstrated that an educational intervention program that used personal and mass media communication was effective in helping the users to quit their habit with the quit rate higher among women and among those with shorter duration of tobacco habits. The effect of the intervention, however, differed according to the type of use.8 From the GATS data, it was observed that the quit rate was 5% in daily smokeless tobacco users and 13% among daily smokers.3 However, a study of tobacco users in rural districts of India found quit rates of only 1.9% to 2.1% among tobacco smokers at one-year follow up, compared to 5.2%–10% among tobacco chewers.10
To fill in this crucial knowledge gap, the International Tobacco Control Policy Evaluation Project in India (the TCP India Project) was started in 2006 with an aim to rigorously evaluate the behavioral effects of tobacco control legislation in four states in India: Maharashtra, Bihar, Madhya Pradesh, and West Bengal. The Wave 1 TCP India Survey is a cross-sectional study of adult (aged 15 years and older) tobacco users and non-users conducted between August 2010 and December 2011. The project’s objective is to provide evidence to guide policies enacted under the FCTC and to systematically evaluate the effectiveness of these legislative efforts. A pilot study of TCP India Survey at 2006 in two Indian states (Maharashtra and Bihar) demonstrated that awareness of damage to one’s health, and exposure to anti-tobacco messages in the media, in restaurants, and in public transportation are predictors for intention to quit tobacco.11
This paper reports on the prevalence of past quit attempts, current intentions to quit, and reasons for intention to quit among tobacco users in four Indian states, as per the findings of the TCP India Wave 1 Survey results.
Subjects and Methods
Sampling design
Respondents for the survey were selected through a multi-stage sampling. In each state, the principal or capital city (Mumbai in Maharashtra, Patna in Bihar, Indore in Madhya Pradesh, and Kolkata in West Bengal) and the surrounding rural areas within 50 kilometers diameter were chosen for sampling, stratified by urban-rural area.
In urban areas, the first stage of sampling was a ‘ward’ and 10 wards were selected by probability proportionate to the size. In the second stage, from each ward, four enumeration blocks (EB) were selected using random sampling, each with an intended number of households for enumeration such that the total for four enumeration blocks was 150 households. Households were approached systematically, and household level information on each member was collected through the key informant in that household.
From rural areas, two or three sub-districts were chosen purposively and from a list of all villages in those sub-districts, four villages were selected with probability proportional to size of respective villages. Each village chosen was mapped and households enumerated. The intended sample size in each village was 125 households. Households were approached systematically, and surveyed by similar procedure as those followed in urban wards.
A maximum of four tobacco users in each enumerated household were interviewed with priority given to female adult tobacco users. One adult non-user of tobacco was selected by random sampling from every third enumerated household.
Household surveys and detailed interviews were conducted face-to-face in the local languages. In the household enumeration process, information on gender, age, and current tobacco use were collected for all household members. Written informed consent was obtained from all respondents at the time of recruitment. A maximum of four attempts were made to complete an interview of a respondent unless that individual refused. Each respondent was given a token of appreciation for their time. More detail on the sampling design is available in “TCP India Project Report”.12
Sample Size
At least 2,000 households (1,500 urban households and 500 rural households) were enumerated in each state to recruit at least 2,000 adult tobacco users and 600 non-users of tobacco per state. Approximately equal numbers of respondents were sampled in each state, with a higher proportion sampled in urban areas as compared to the rural areas, with the ratio of 3:1. The intended total sample size of the survey was 8,000 adult tobacco users and 2,400 adult tobacco non-users aged 15 and older. The final sample size was 8,051 adult tobacco users and 2,534 non-users, although the present study reports only on the tobacco users.
Measures
The outcomes assessed in this study were: (a) quit attempts; (b) intention to quit among those who made a past quit attempts in last six months; (c) intention to quit among all tobacco users; (d) reasons for intention to quit and (e) other factors like health care provider (HCP)/doctor’s advice and anti-tobacco messages associated with intention to quit. All data were based on self-report. In addition, demographic parameters and type of tobacco use were also measured.
In the survey, respondents who smoked cigarettes or bidis in the last thirty days were considered as smokers, respondents who used any smokeless tobacco product in last thirty days were considered as smokeless tobacco users, and respondents who used both forms of tobacco were consider as mixed tobacco users. Respondents who said they were planning to quit their tobacco use either in the next month, next six months, or sometime in the future, were categorized as having an intention to quit, and all others were categorized as having no intention to quit.
In the survey, education was divided into three categories: low, moderate, and high. Low education category includes the respondents who were illiterate or completed primary or middle school education. Moderate educational category includes the respondents who completed secondary school and/or Industrial Training Institute (ITI) course, and high education category includes the respondents who completed college and above education.
Similarly, income level was divided into 3 categories: low, moderate, and high. Low income category includes the respondents who earned less than 5,000 INR per month, moderate income category includes the respondents who earned an income between 5,000 and 15,000 INR per month and high income category includes the respondents who earned an income more than 15,000 INR.
Statistical Analysis
Analyses were done with weighted data using the complex samples function of SPSS version 20. Multivariate logistic regression was used to examine the association between intention to quit and the demographic variables. In the logistic regression model, intention to quit tobacco was the dependent variable (intention to quit tobacco =1 and no intention to quit =0). State, location, age, gender, education, health care provider and/or doctor’s advice, and anti-tobacco messages were categorical variables taken as independent variables in the model. The multivariate model also included the covariates: age, gender, state, education and type of tobacco use status.
Results
The sample characteristics were calculated using un-weighted data set so are not representative of the population.
The socio-demographic characteristics of the sample are presented in Table 1. Most of the respondents were between the age group of 25–39 years (33.3%). Majority of the respondents practiced Hindu religion (82.3%). Overall, 60.2% of the sample was reported as having a low education level and 56.2% of the sample reported a moderate income.
Table 1.
Sample characteristics of the tobacco users: TCP India Wave I Survey.
| Category | State | ||||
|---|---|---|---|---|---|
|
| |||||
| Bihar N = 2,008 | Maharashtra N = 2,051 | Madhya Pradesh N = 1992 | West Bengal N = 2,000 | Total N = 8,051 | |
| Urban/Rural (%) | |||||
|
| |||||
| Urban | 73.6 | 67.9 | 75.5 | 74.6 | 72.9 |
| Rural | 26.4 | 32.1 | 24.5 | 25.4 | 27.1 |
|
| |||||
| Gender (%) | |||||
|
| |||||
| Female | 39.2 | 39.8 | 22.3 | 27.7 | 32.3 |
| Male | 60.8 | 60.2 | 77.7 | 72.3 | 67.7 |
|
| |||||
| Age (in years) (%) | |||||
|
| |||||
| 15–17 | 5.6 | 0.6 | 1.8 | 0.8 | 2.2 |
| 18–24 | 16.3 | 8.7 | 11.2 | 9.3 | 11.4 |
| 25–39 | 34.5 | 33.8 | 30.3 | 34.4 | 33.3 |
| 40–54 | 25.3 | 30.8 | 31.4 | 32.7 | 30.1 |
| 55+ | 18.3 | 26.0 | 25.3 | 22.9 | 23.1 |
|
| |||||
| Marital Status (%) | |||||
|
| |||||
| Single | 22.1 | 10.7 | 15.2 | 13.5 | 15.4 |
| Married | 71.9 | 75.0 | 73.9 | 77.5 | 74.5 |
| Other | 6.1 | 14.3 | 10.9 | 9.1 | 10.1 |
|
| |||||
| Religion (%) | |||||
|
| |||||
| Hindu | 83.1 | 81.3 | 90.7 | 74.2 | 82.3 |
| Others | 16.9 | 18.7 | 9.3 | 25.8 | 17.7 |
|
| |||||
| Occupation (%) | |||||
|
| |||||
| Workers | 49.8 | 52.1 | 71.2 | 60.0 | 58.2 |
| Students | 11.9 | 0.8 | 2.1 | 1.3 | 4.0 |
| Unemployed | 6.8 | 5.9 | 10.3 | 8.5 | 7.8 |
| Housewife | 29.8 | 32.8 | 13.9 | 16.9 | 23.5 |
| Other | 1.7 | 8.4 | 2.5 | 13.3 | 6.5 |
|
| |||||
| Education** (%) | |||||
|
| |||||
| Low | 52.6 | 56.3 | 64.0 | 68.0 | 60.2 |
| Moderate | 28.4 | 39.8 | 28.2 | 21.0 | 29.4 |
| High | 18.9 | 3.9 | 7.7 | 11.0 | 10.3 |
|
| |||||
| Income*** (%) | |||||
|
| |||||
| Low | 28.8 | 10.7 | 28.1 | 44.1 | 27.8 |
| Moderate | 52.3 | 70.4 | 60.0 | 41.7 | 56.2 |
| High | 17.0 | 15.7 | 7.5 | 12.7 | 13.3 |
| Not Stated | 1.9 | 3.1 | 4.4 | 1.5 | 2.7 |
The sample characteristics were calculated using un-weighted data set so are not representative of the population.
Education category: low (illiterate or primary or middle school), moderate (secondary school or ITI course), or high (college or above) education.
Income category: a) Low: Less than 5,000 INR/month, b) Moderate: 5,000–15,000 INR/month, c) High: 15,000+ INR/month.
Table 2 represents the distribution of tobacco use status according to gender and state.
Table 2.
Distribution of adult tobacco use status by gender and state
| Type of tobacco use | States | ||||
|---|---|---|---|---|---|
|
| |||||
| Bihar | Maharashtra | Madhya Pradesh | West Bengal | Total | |
| Overall (N) | 2008 | 2051 | 1992 | 2000 | 8051 |
| (%) | 100 | 100 | 100 | 100 | 100 |
|
| |||||
| Smoked Tobacco Users | 5.5 | 9.5 | 19.2 | 32.7 | 17.1 |
| Mixed Tobacco Users | 12 | 6.5 | 10 | 15.8 | 10.9 |
| Smokeless Tobacco Users | 82.5 | 84 | 70.8 | 51.5 | 72 |
|
| |||||
| Male (N) | 1221 | 1234 | 1548 | 1446 | 5449 |
| (%) | 100 | 100 | 100 | 100 | 100 |
|
| |||||
| Smoked Tobacco Users | 5.9 | 15 | 23.9 | 43.2 | 24 |
| Mixed Tobacco Users | 17 | 10.2 | 12.4 | 20.9 | 15.6 |
| Smokeless Tobacco Users | 77.1 | 74.8 | 63.7 | 35.9 | 60.4 |
|
| |||||
| Female (N) | 787 | 817 | 444 | 554 | 2602 |
| (%) | 100 | 100 | 100 | 100 | 100 |
|
| |||||
| Smoked Tobacco Users | 4.7 | 0.2 | 0 | 1.5 | 1.5 |
| Mixed Tobacco Users | 0.6 | 0.1 | 0.5 | 0.3 | 0.3 |
| Smokeless Tobacco Users | 94.7 | 99.7 | 99.5 | 98.1 | 98.3 |
The results were calculated using weighted data set.
Out of the total sample of tobacco users, 72% were smokeless tobacco users, 17.1% were smokers and 10.9% were mixed users. The proportion of smokers and mixed users was highest in West Bengal (32.7% and 15.8%) whereas smokeless tobacco users were highest in Maharashtra (84%) followed closely by Bihar (82.5%).
Females were predominantly smokeless tobacco users (98.3%) although the majority of males were also smokeless tobacco users (60.4%). Smoking was mostly reported by males (24%) and rarely by females (1.5%). Similarly, mixed tobacco use was also higher among males (15.6%) than in females (0.3%).
Figure 1, shows that overall 19.6% of tobacco users had an intention to quit tobacco in future. In the past, 25% had tried to quit but failed and among those, 36.9% still had an intention to quit tobacco. The most objective measure, attempt to quit, was nearly identical (range 22.4% to 26.9%) across the states. However, the intention to quit among those who made a quit attempt varied in different states, from 15% in Madhya Pradesh to 49.3% in Bihar.
Figure 1.
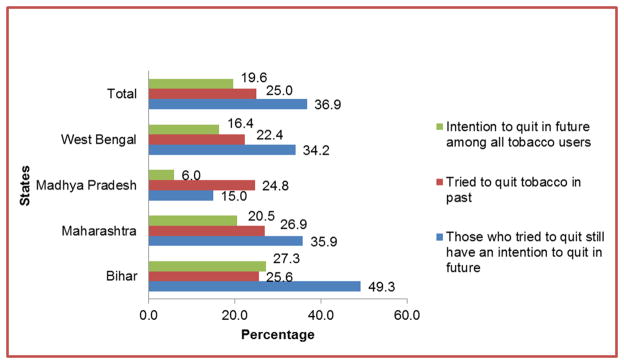
Tried to quit and Intention to quit tobacco
The respondents who intended to quit tobacco were asked about their reasons for thinking about quitting tobacco. Figure 2 shows the percentage of respondents in each state who specified the reasons that led them to think about quitting. The most common reason was concern for personal health (92.5% overall). Across all the four states, the proportion of tobacco users who reported personal health as a most important reason for thinking about quitting varied as follows: Maharashtra 94.8 %, Bihar 91.2%, West Bengal 91%, and Madhya Pradesh 86.8%.
Figure 2.

Reasons for thinking about Quitting Tobacco
Another reason was setting an example for children (60% overall); it was a more common reason in Bihar (84%) and Maharashtra (61.3%) than the other two states. Similarly, close friends and family disapproval was another important predictor (52% overall) which was highest in Bihar (60.3%) followed by Maharashtra (56.6%).
Only half of the smokers from Bihar and Maharashtra were concerned about the effect of their tobacco smoke on non-smokers, and about the restrictions of smoking in public places. The price of tobacco, cost of living, and workplace restrictions were the least important reasons for thinking about quitting.
Table 3 represents the factors associated with intention to quit tobacco in multivariate logistic regression analyses after adjusting for age, gender, state, education and type of tobacco use.
Table 3.
Factors associated with Intention to quit tobacco
| Variables | N | % | Adjusted Odds Ratio | 95% Confidence Interval |
|---|---|---|---|---|
| State | ||||
|
| ||||
| Madhya Pradesh | 1992 | 6 | Reference | |
| Bihar | 2008 | 23.3 | 3.98 | 1.52–10.41 |
| West Bengal | 2000 | 13.9 | 2.67 | 1.42–5.01 |
| Maharashtra | 2051 | 19.9 | 3.74 | 1.79–7.80 |
|
| ||||
| Type of tobacco use | ||||
|
| ||||
| Smokeless users | 5991 | 72 | Reference | |
| Smoker | 1255 | 17.1 | 0.86 | 0.63–1.18 |
| Mixed users | 805 | 10.9 | 1.48 | 1.12–1.97 |
|
| ||||
| Location | ||||
|
| ||||
| Rural | 2185 | 16.6 | Reference | |
| Urban | 5866 | 15.5 | 0.87 | 0.36–2.13 |
|
| ||||
| Age | ||||
|
| ||||
| 55+ | 1863 | 13.3 | Reference | |
| 40–54 | 2421 | 14.6 | 1.09 | 0.85–1.41 |
| 25–39 | 2677 | 17.4 | 1.27 | 0.95–1.68 |
| 18–24 | 914 | 18.4 | 1.31 | 0.94–1.84 |
| 15–17 | 176 | 22.7 | 1.48 | 0.88–2.50 |
|
| ||||
| Gender | ||||
|
| ||||
| Female | 2602 | 14.8 | Reference | |
| Male | 5449 | 16.3 | 0.92 | 0.67–1.25 |
|
| ||||
| Education | ||||
|
| ||||
| Low | 4839 | 13.1 | Reference | |
| Moderate | 2366 | 19 | 1.59 | 1.30–1.94 |
| High | 831 | 22.6 | 1.84 | 1.11–3.06 |
|
| ||||
| Advice by doctor/HCP to quit tobacco | ||||
|
| ||||
| No | 1395 | 18.6 | Reference | |
| Yes | 910 | 25.7 | 1.65 | 1.28–2.13 |
|
| ||||
| Exposure to anti-tobacco messages on Public Transportation Vehicles | ||||
|
| ||||
| No | 4525 | 10.6 | Reference | |
| Yes | 3524 | 22.5 | 2.13 | 1.49–3.08 |
|
| ||||
| Exposure to anti-tobacco messages at bars | ||||
|
| ||||
| No | 7517 | 15.1 | Reference | |
| Yes | 532 | 25.4 | 1.81 | 1.07–3.06 |
|
| ||||
| Exposure to anti-tobacco messages on tobacco packages | ||||
|
| ||||
| No | 2723 | 11.2 | Reference | |
| Yes | 5325 | 18.2 | 1.77 | 1.30–2.41 |
|
| ||||
| Exposure to anti-tobacco messages at work places | ||||
|
| ||||
| No | 5981 | 13.4 | Reference | |
| Yes | 2069 | 22.8 | 1.73 | 1.23–2.44 |
|
| ||||
| Exposure to anti-tobacco messages at Restaurants | ||||
|
| ||||
| No | 6068 | 14 | Reference | |
| Yes | 1981 | 21.3 | 1.63 | 1.11–2.40 |
|
| ||||
| Exposure to anti-tobacco messages on Radio | ||||
|
| ||||
| No | 5675 | 14.4 | Reference | |
| Yes | 2374 | 19.1 | 1.34 | 0.93–1.92 |
|
| ||||
| Exposure to anti-tobacco messages on print media | ||||
|
| ||||
| No | 4880 | 13.3 | Reference | |
| Yes | 3170 | 19.7 | 1.3 | 0.96–1.77 |
|
| ||||
| Exposure to anti-tobacco messages on Television | ||||
|
| ||||
| No | 2526 | 13.5 | Reference | |
| Yes | 5523 | 16.9 | 1.13 | 0.82–1.55 |
|
| ||||
| Exposure to anti-tobacco messages on Cinema halls | ||||
|
| ||||
| No | 6469 | 15.1 | Reference | |
| Yes | 1579 | 18.7 | 1.06 | 0.72–1.55 |
adjusted with age, gender, state, education and by type of tobacco use
Effect of state, type of tobacco use, residence, age, gender, and educational status on intention to quit tobacco
Compared to Madhya Pradesh, the respondents from Bihar (adjusted OR=3.98, CI=1.52–10.41), Maharashtra (adjusted OR=3.74, CI=1.79–7.80) followed by West Bengal (adjusted OR=2.67, CI=1.42–5.01) had significantly higher intention to quit tobacco. Smokers had less intention to quit as compared to smokeless tobacco users whereas mixed users had more intention to quit (OR = 1.48, 95% CI = 1.12–1.97) compared to smokeless tobacco users. Type of residence (urban or rural area), age group, and gender were not significant predictors of intentions to quit. Those with moderate or high education were more likely to intend to quit (adjusted OR=1.84, 95% CI=1.11–3.06) compared to the less educated people.
Effect of doctors and/or health professional’s advice on intention to quit tobacco
The intention to quit (adjusted OR=1.65, CI=1.28–2.13) was significantly higher among those who were advised by doctors/HCP to quit tobacco compared to non-advised respondents.
Effect of anti-tobacco messages on intention to quit
Tobacco users who were exposed to anti-tobacco messages at workplaces (adjusted OR=1.73, CI=1.23–2.44), at restaurants (adjusted OR=1.63, CI=1.11–2.40), bars (adjusted OR=1.81, CI=1.07–3.06), on public transportation vehicles (adjusted OR=2.13, CI=1.49–3.08), and on tobacco packages (adjusted OR=1.77, CI=1.30–2.41) had a higher intention to quit tobacco compared to those who were not exposed to such messages in the last six months. Exposure to anti-tobacco messages on television, on radio, and in cinema halls did not have any significant impact on intention to quit tobacco.
Discussion
The present study reports the prevalence of past quit attempts, current intentions to quit, and the reasons for considering quitting in four Indian states. Consistent with the GATS India 2009–10 report, the rate of quit attempts in the TCP India sample was found to be very low. It is thus important to understand the factors that are related to future quitting among Indian tobacco users. Three main findings emerge from this study: (a) About one fifth of the tobacco users intended to quit tobacco; (b) Concern for personal health was the most important reason for considering quitting; (c) Higher education, doctor’s advice, and anti-tobacco messages have a positive influence on users’ intention to quit tobacco.
Intention to quit tobacco as assessed through this study is found to be low at 19.6 % in comparison to evidence from previous studies. GATS had estimated this figure to be 40%. This was also low compared to the estimates from other low- and middle-income countries in the ITC Project such as Malaysia (57.8%) and Thailand (40.2%).7
Looking at the predictors of quit intention, it was found that socio demographic factors such as age and gender did not significantly predict intention to quit tobacco, which is consistent with the findings of previous research.9–13 In Malaysia and Thailand, independent predictors of staying quit were being older (55+), urban residence, smoking abstinence for six months or more in the past and less smoking frequency per day, higher level of self-efficacy, and having had an intention to quit within one month.7 Past experience with quitting,14 having a positive attitude toward quitting,15 higher self-efficacy, and high level of readiness to quit16 were positively associated with intentions. Similarly, in the current study, the individuals who had tried to quit in the past also had a stronger intention to quit in future. Among those who had tried to quit, higher education17 has been shown to be the most important demographic predictor which is consistent with the findings from the current study. The study by Siahpush et al. also examined the association of socioeconomic position with cigarette consumption, intention to quit, and self-efficacy to quit among male smokers in Thailand and Malaysia using the ITC Southeast Asia (SEA) Survey. It was found that higher level of education was not associated with consumption of cigarettes or with intention to quit in Malaysia and Thailand18. These findings differ from the present study where a higher level of education was predictive of making quit attempts but income was not associated with quitting.
Previous studies have also demonstrated that intention to quit tobacco is observed more in users who felt that the tobacco use has damaged their health.11 The current study confirms this finding; concern for personal health was the most common reason for considering quitting.
Previous studies show the positive impact of exposure to anti-tobacco messages via television on the intention to quit11; however the current study shows the impact of anti-tobacco messages on public transportation, at bars, restaurant, tobacco packages, and work places had an impact on intention to quit tobacco, whereas television did not have a significant impact.
Properly designed anti-smoking messages shown in the cinema halls increase the awareness about harms of smoking and in Australia have been shown to increase intention to quit among smokers.19 Anti-smoking mass media campaigns can help reduce the prevalence of smoking by encouraging current smokers to quit and discouraging young persons from starting20, in the current study the effect of anti-smoking media messages on the people to quit tobacco is low compared to other studies20.
There were some limitations to this study. The present study was restricted to four states in India; therefore, the results are not representative of tobacco users in India as a whole. The data collected from this study was dependent on respondents’ self-reporting and may be subject to recall bias.
Nevertheless, the study has brought forward some crucial findings. There is a strong and urgent need for skilled cessation support via the health care providers/doctors in India. This can be judged from the finding that a quarter of the current tobacco users had made quit attempts in the past and many among them expressed a wish to quit tobacco in the future. It can be reasonably assumed that if skilled systematic support could be provided during the abstinence period, then the successful quit rate might increase in the future. Thus, there is a need to have cessation centers with trained counsellors to provide such support to the tobacco users.
It was observed that concern for personal health is one of the most important factors influencing the intention to quit. Therefore, stronger anti-tobacco messages and warnings about the health effects of tobacco consumption on tobacco packages may also further strengthen the users’ intention to quit tobacco.
To conclude, one of the main finding of this study was that a low percentage of tobacco users in India made attempts to quit, and those that do attempt are not successful for a variety of reasons. The study also provides insight into tobacco control efforts and intervention strategies that should be emphasized in order to increase the motivation to quit tobacco; cessation centres must be initiated and the cessation programs and the anti-tobacco campaigns must be focus on key messages like concern for personal health and being role model for children. We anticipate that such insights will provide an evidence base for designing further tobacco control policies and programs and contribute towards significantly enhancing cessation rates in India.21
Ethics Approval
All study materials and procedures used in the TCP India Survey were reviewed and cleared for ethics by the Office of Research Ethics at the University of Waterloo, Canada and by the Institutional review boards at the Healis-Sekhsaria Institute for Public Health, Mumbai, India.
Key Messages.
If skilled systematic support could provide during the abstinence period, then the successful quit rate might increase in the future. Thus, there is a need to have cessation centres with trained counsellors to provide such support to the tobacco users. The study also provides insight into tobacco control efforts and intervention strategies that should be emphasized in order to increase the motivation to quit tobacco.
Acknowledgments
The TCP India Project was supported by grants from the US National Cancer Institute (P01-CA138389), Canadian Institute of Health Research (79551 and 115216) and Ontario Institute for Cancer Research Senior Investigator Award. GTF was supported by a Senior Investigator Award from the Ontario Institute for Cancer Research and by a Prevention Scientist Award from the Canadian Cancer Society Research Institute. We would like to acknowledge Dr. Lalit Raute and Mr. Sameer Narake for their valuable suggestions on analysis. We would like to thank our field research team and our collaborators for doing the hard work for collecting data.
References
- 1.WHO report on the global tobacco epidemic, 2011: warning about the dangers of tobacco. Geneva: World Health Organization; 2011. ( http://whqlibdoc.who.int/hq/2011/WHO_NMH_TFI_11.3_eng.pdf) [Google Scholar]
- 2.Edwards R. The problem of tobacco smoking. BMJ. 2004;328(7433):217–9. doi: 10.1136/bmj.328.7433.217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ministry of Health and Family Welfare, G.o. I. Global Adult Tobacco Survey - India 2009–2010, 2010. Ministry of Health and Family Welfare, Government of India, New Delhi; New Delhi: [Google Scholar]
- 4.Abdullah AS, Husten CG. Promotion of smoking cessation in developing countries: a framework for urgent public health interventions. Thorax. 2004;59(7):623–30. doi: 10.1136/thx.2003.018820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hyland A, Borland R, Li Q, Yong H-H, McNeill A, Fong GT, O’Connor RJ, Cummings KM. Individual- level predictors of cessation behaviors among participants in the International Tobacco Control (ITC) Four Country Survey. Tob Control. 2006;15:iii83–iii94. doi: 10.1136/tc.2005.013516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Reid JL, Hammond D, Boudreau C, Fong GT, Siahpush M. Socioeconomic disparities in quit intentions, quit attempts, and smoking abstinence among smokers in four western countries: Findings from the International Tobacco Control Four Country Survey. Nicotine Tob Res. 2010 Oct;12(Suppl 1):S20–S33. doi: 10.1093/ntr/ntq051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Li L, Borland R, Yong HH, Fong GT, Bansal-Travers M, Quah ACK, Sirirassamee B, Omar M, Zanna MP, Fotuhi O. Predictors of smoking cessation among adult smokers in Malaysia and Thailand: Findings from the International Tobacco Control Southeast Asia Survey. Nicotine and Tobacco Research. 2010 Oct;12(Supplement 1):S34–S44. doi: 10.1093/ntr/ntq030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gupta PC, Aghi MB, Bhonsle RB, Murti PR, Mehta FS, Mehta CR, Pindborg JJ. An Intervention study of tobacco chewing and smoking habits for primary prevention of oral cancer among 12,212 Indian villagers. IARC Sci Publ. 1986;(74):307–18. [PubMed] [Google Scholar]
- 9.Pimple S, Pednekar M, Mazumdar P, Goswami S, Shastri S. Predictor of quitting tobacco – Results of a Worksite Tobacco Cessation Service Program among factory workers in Mumbai. Asian Pacific Journal of Cancer Prevention. 2012;13:533–538. doi: 10.7314/apjcp.2012.13.2.533. [DOI] [PubMed] [Google Scholar]
- 10.Mehta FS, Aghi MB, Gupta PC, Pindborg JJ, Bhonsle RB, Jahawalla PN, Sinor PN. An Intervention study of oral cancer and precancerous in rural Indian populations: A preliminary report. Bull World Health Organ. 1982;60:441–446. [PMC free article] [PubMed] [Google Scholar]
- 11.Surani NS, Gupta PC, Fong TG, Pednekar MS, Quak AC, Bansal-Travers M. Intention to quit among India tobacco users: Findings from International Tobacco Control Policy evaluation India pilot survey. Indian J Cancer. 2012;49:431–7. doi: 10.4103/0019-509X.107752. [DOI] [PubMed] [Google Scholar]
- 12.http://www.healis.org/SV/TCP%20IndiaNR-ENG-Sept25v-web.pdf
- 13.Fegan P, Augustson E, Backinger C, Connell M, Vollinger R, Kaufman A, Gibson J. Quit attempts and Intention to quit Cigarette Smoking among young adults in the United States. American Journal of Public Health. 2007 Aug;97(8) doi: 10.2105/AJPH.2006.103697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Haddad L, Petro-Nustas W. Predictors of intention to quit smoking among Jordanian university students. Canadian Journal of Public Health. 2006;97:9–13. doi: 10.1007/BF03405204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Yu D, Wu K, Abdullah A. Smoking cessation among Hong Kong Chinese smokers attending hospital as outpatients: Impact of doctors’ advice, successful quitting and intention to quit. Asia Pacific Journal of Public Health. 2004;16:115–120. doi: 10.1177/101053950401600207. [DOI] [PubMed] [Google Scholar]
- 16.Wang S, Borland R, Whelan A. Determinants of intention to quit: Confirmation and extension of Western theories in male Chinese smokers. Psychology and Health. 2005;20:35–51. [Google Scholar]
- 17.Lee CW, Kahende J. Factors associated with successful smoking cessation in the United States, 2000. American Journal of Public Health. 2007;97:1503–1509. doi: 10.2105/AJPH.2005.083527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Siahpush M, Borland R, Yong H-H, Kin F, Sirirassamee B. Socio-economic variations in tobacco consumption, intention to quit and self-efficacy to quit among male smokers in Thailand and Malaysia: Results from the International Tobacco Control South-East Asia (ITC SEA) survey. Addiction. 2008;103:502–508. doi: 10.1111/j.1360-0443.2007.02113.x. [DOI] [PubMed] [Google Scholar]
- 19.Edward CA, Harris WC, Cook DR, Bedford KF, Zuo Y. Out of the Smokescreen: Does an anti smoking advertisement affect young women’s perception of smoking in movies and their intention to smoke? Tob Control. 2004;13:277–82. doi: 10.1136/tc.2003.005280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.http://www.naquitline.org/news/127076/CDC-Global-Tobacco-Antismoking-Messages-and-Intention-to-Quit-.htm
- 21.Raute LJ, Sansone G, Pednekar MS, Fong GT, Gupta PC, Quah AC, et al. Knowledge of health effects and intentions to quit among smokeless tobacco users in India: Findings from the International Tobacco Policy Evaluation Survey (ITC) India Pilot Survey. Asia Pacific J Cancer Prev. 2011;12:1233–8. [PubMed] [Google Scholar]