

Introduction
Snake venom ophthalmia is caused by venoms of spitting elapid and other snakes. The cobra is one of the most venomous snakes of genus Naja. There are more than 20 species of cobra like the King cobra of South Africa, Thailand, Burma, China, India, Malaysia, Philippines; the spitting cobra of Africa and parts of South East Asia; the Indian cobra found in India and Central Asia; and the tree cobra, which is found in Central and Western equatorial Africa.1 Spitting cobras can eject venom into the eyes of their preys or predators. Humans can also be accidentally affected and fear of death or of becoming blind can cause extreme anxiety in the afflicted person. We report an uncommon case of a man who received snake venom in his eye.
Case report
A 28-year-old patient reported to our hospital with complaints of severe burning sensation in left eye associated with redness and watering for about 02 h duration. Individual was opening his garage when two snakes fell over his left elbow from above and as he shrugged his hand some liquid fell into his left eye. He developed severe burning sensation followed by redness and watering in his left eye. He reported to our hospital. Ocular examination revealed normal right eye with visual acuity of 6/6. Best corrected visual acuity in left eye was 6/12. Slit lamp examination revealed conjunctival congestion, few discrete corneal epithelial patches that stained with fluorescein dye (Fig. 1).
Fig. 1.
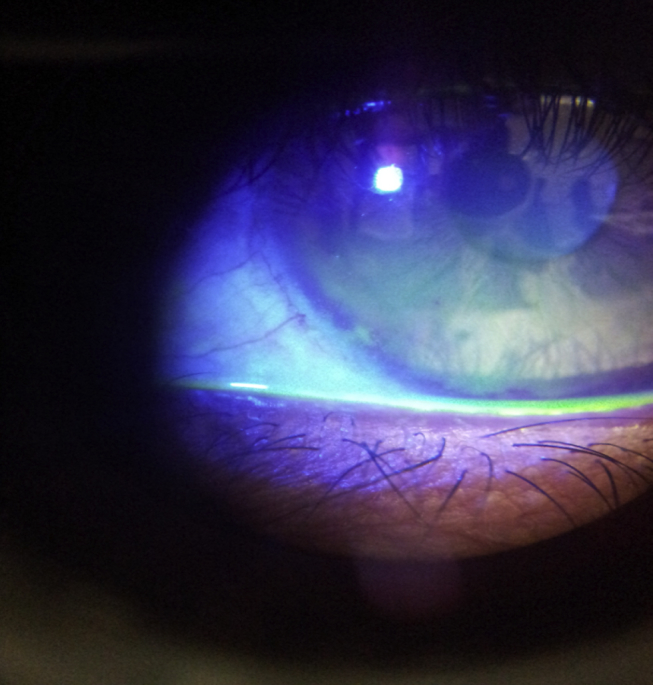
Fluorescein stained corneal epithelial lesions.
Diffuse punctuate staining in other areas of cornea were also seen. There was no anterior chamber reaction. Rest ocular examination did not reveal any abnormality. Intraocular pressure was 16 mmHg (by Non-Contact Tonometer) in each eye. There were no signs/symptoms suggestive of systemic envenomation.
After thorough irrigation with normal saline, individual was started on topical eye drop moxifloxacin 0.5% four times a day, topical eye drop homatropine 2% twice a day, topical heparin (2500 U/ml) three times a day in left eye and oral analgesics. Eye drop homatropine 2% was stopped on 3rd day. On 5th day visual acuity improved to 6/6 in left eye, burning sensation had decreased, corneal lesions had healed. All medications were stopped after one week and individual was discharged from the hospital. He was reviewed after one month and ocular examination was normal. There was no decrease or loss of corneal sensations.
Discussion
Spitting cobras belong to the elapid family of snakes. Of these, Naja siamensis or the Indo–Chinese cobra is found in the South East Asian region and Naja nigricollis and Hemachatus haemachatus are found in Africa. Natural habitats of spitting cobras include hills, lowlands, plains and woodland. They get attracted towards human settlements due to high population of rodents. These can spit venom up to a distance of eight to twelve feet.
Snake venom ophthalmia due to Naja atra has been reported from China and Hong Kong.2 “Venom spitting” is a reflex mechanism aimed at ejecting venom forcefully into the eyes of its victims.3 Spitting cobra venom contains a mixture of neurotoxins, cytotoxins, phospholipases and cardiotoxins. Cardiotoxins with membrane lytic properties are thought to be responsible for corneal erosions and conjunctival chemosis.4 The ocular effects of the venom depend on duration of contact of ocular surface with venom. Ocular contact with snake venom results in pain, diminution of vision, blepharospasm, conjunctival inflammation and chemosis. Initially there may be small fluorescein staining corneal epithelial defects. The epithelial cells lyse to form large epithelial defects or erosions. Fortunately the venom enzymes do not penetrate the corneal stroma made up of collagen therefore protecting cornea from permanent stromal opacification. Systemic effects of snake venom ophthalmia have not been reported.5
Copious irrigation of the eyes with water at the earliest is single most important step in management of this condition. This removes venom from the eyes and hence prevents corneal damage due to various toxins present in it. Prophylactic broad spectrum topical antibiotics may be started in case of corneal erosions to prevent keratitis.
Heparin has been used to treat snake venom ophthalmia. Its use is based on the fact that the cardiotoxin in snake venom readily binds to the acidic sites in the heparin molecule and renders the cardiotoxin inactive in experimental models.6 Topical vasoconstrictors or patching of the eyes helps to reduce pain. However, the WHO guidelines published in 2010 advised against the use of topical or intravenous anti-venom and topical corticosteroids. Corneal collagenase activity is enhanced by topical steroids and in the presence of epithelial defects may cause corneal melting. The use of dilute anti-venom has not been found useful.7
Conclusion
In conclusion, snake venom ophthalmia is rare form of envenoming which presents as intensely painful blurred vision associated with blepharospasm, conjunctival congestion, corneal epithelial defects and chemosis. There is no evidence of systemic involvement following ocular envenoming in the literature.
Conflicts of interest
All authors have none to declare.
References
- 1.Raja Sajid Adhi, Kok Kenneth Yuh Yen. Snake venom ophthalmia. Brunei Int Med J. 2011;7(6):332–335. [Google Scholar]
- 2.Fung H.T., Lam K.K., Wong O.F., Lam T.S. Local antivenom treatment for ophthalmic injuries caused by a Naja atra. J Med Toxicol. 2010;6:147–149. doi: 10.1007/s13181-010-0068-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Young B.A., Boetig M., Westhoff G. Functional bases of the spatial dispersal of venom during cobra “spitting””. Physiol Biochem Zool. 2009;82:80–89. doi: 10.1086/595589. [DOI] [PubMed] [Google Scholar]
- 4.Kao P.H., Wu M.J., Chang L.S. Membrane-bound conformation of Naja nigricollis toxin gamma affects its membrane-damaging activity. Toxicon. 2009;53:342–348. doi: 10.1016/j.toxicon.2008.12.003. [DOI] [PubMed] [Google Scholar]
- 5.Chu E.R., Weinstein S.A., White J., Warrell D.A. Venom ophthalmia caused by venoms of spitting elapid and other snakes: report of ten cases with review of epidemiology, clinical features, pathophysiology and management. Toxicon. 2010;56:259–272. doi: 10.1016/j.toxicon.2010.02.023. [DOI] [PubMed] [Google Scholar]
- 6.Cham G., Pan J.C., Lim F., Earnest A., Gopalakrishnakone P. Effects of topical heparin, antivenom, tetracycline and dexamethasone treatment in corneal injury resulting from the venom of the black spitting cobra (Naja sumatrana) in a rabbit model. Clin Toxicol. 2006;44:287–292. doi: 10.1080/15563650600584451. [DOI] [PubMed] [Google Scholar]
- 7.Warrell D.A. Guidelines for the Management of Snake-bites: Management of Cobra Spit Ophthalmia. WHO Library Cataloguing-in-Publication Data; 2010. pp. 123–124. [Google Scholar]