

Highlights
-
•
There are rare reports of small intestinal intussusceptions caused by metastatic lung carcinosarcoma.
-
•
Medical treatment, chemotherapy, and radiotherapy are not active in this kind of tumor, so surgery is the treatment of choice.
-
•
Surgical treatment plays an important role in lung cancer patients with GI metastasis that cause bowel obstruction, perforation, or massive hemorrhage.
-
•
This presentation shows the third case in literature.
Keywords: Sarcomatoid carcinoma, Lung, Small intestinal intussusceptions, Small intestinal obstruction, Gastrointestinal metastasis, Metastatic pulmonary tumors
Abstract
Introduction
Sarcomatoid carcinoma is an extremely rare, biphasic tumor characterized by a combination of malignant epithelial and mesenchymal cells. Limited data showed that most cases occurred with advanced local disease and metastasis.
Presentation of case
We present a rare case of a 60-year-old man with three small intestinal intussusceptions due to metastatic pulmonary carcinosarcoma. He was explored for chest pain and hemoptysis in Emergency room. Due to his chest symptoms he had a computed tomography (CT) scan of the chest which showed a lesion about 60 mm in diameter in the inferior lobe of the left lung. After 2 weeks physical examination demonstrated a distended abdomen and auscultation was indicated by hyperactive bowel sounds. Further imaging studies with abdominal computed tomography (CT) scan, showed multiple protruding small bowel tumors with entero enteric intussusceptions at three sites requiring a massive bowel resection at surgery. The pathology showed that it was positive for cytokeratin, vimentin, CD-34, and LIS; CK7 was focally positive; and CD117, CD20, and desmine were negative. The final diagnosis was metastatic small bowel carcinosarcoma with a lung primary.
Discussion
Lung carcinosarcoma is a high grade biphase neoplasm. The survival rate at 6 months is only around 27%.
Conclusion
There are rare reports of small intestinal intussusceptions caused by metastatic lung carcinosarcoma, this presentation shows the third case in literature. Physicians should be more alert to symptoms or signs indicating GI metastais in patients with a history of lung cancer.
1. Introduction
Sarcomatoid carcinoma is an extremely rare, biphasic tumor characterized by a combination of malignant epithelial and mesenchymal cells. Limited data on sarcomatoid carcinoma showed that most cases occurred with advanced local disease and metastasis, and paraneoplastic syndromes were rare [1]. Fishback et al. [2] designated sarcomatoid carcinomas as pleomorphic (spindle/giant cell) carcinomas of the lung because both spindle and giant cell components often are found in the same tumors [3]. In 2004, WHO classified sarcomatoid carcinomas into pleomorphic carcinoma, spindle cell carcinoma, giant cell carcinoma, carcinosarcoma, and pulmonary blastoma [3,4].
It is a rare lung malignancy with aggressive characteristics. Lung carcinosarcoma occurs mainly in elderly men, smokers, with a male-to-female ratio of 7.25:1 and a median age at onset of 65 years. The average tumor size at diagnosis is 7 cm It accounts for only 1.3% of lung malignancies. The 5-year survival rate is around 21% [5]. There is no specific clinical presentation and typical symptoms include chest pain,cough, hemoptysis, dyspnea, fever, and weight loss [6,7].
It is usually metastasized at diagnosis and the reported incidence of GI metastasis from lung cancer varies from 0.5–10%, and mainly depends on the evaluation method used (endoscopy, surgical specimens, or autopsy) [8–10]. The typical presentations of GI metastases are abdominal pain, bleeding, obstruction, perforation, and small intestinal intussusception caused by metastatic lung carcinosarcoma.
Medical treatment, chemotherapy, and radiotherapy are not active in this kind of tumor, so surgery is the treatment of choice. Prognosis is poor with a median survival time of 9–12 months after potentially curative surgical resection [11]. We present a very rare case of a 60-year-old man with three small intestinal intussusceptions due to metastatic pulmonary carcinosarcoma (Figs. 1 and 2).
Fig. 1.
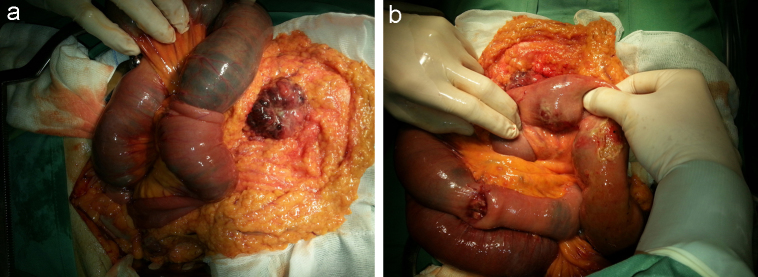
Intra-operative findings. (A) One of three intussusceptions found; (B) the small bowel loops are grossly distended.
Fig. 2.
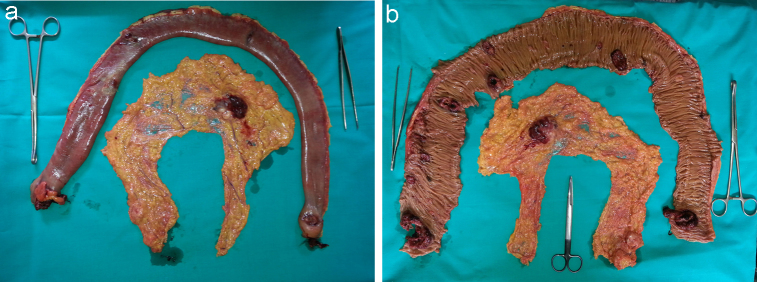
The largest segment of bowel resected, about 80 cm long, contained ten polypoid lesions.
2. Presentation of case
A 60-year-old man, 2 weeks before the access to our surgical department, was explored for chest pain, hemoptysis, and fever in Emergency room. His previous medical history revealed that he was a heavy smoker and no occupational exposures were reported. Due to his chest symptoms he had a chest X-ray followed by Computed Tomography (CT) scan of the chest which showed a lesion about 60 mm in diameter in the inferior lobe of the left lung with mediastinal and left hilar lymphadenopathy, an enlargement of thyroid gland; so the patient underwent a surgical biopsy of a lymph node and the pathology showed a tumor that was partly epithelial in origin and partly derived from mesenchyma, and it confirmed the primary lung cancer.
After 2 weeks, he was admitted to our Department complaining about a completely different symptoms, abdominal pain, and vomiting, he described the absence of gas and feces for 2 days. Physical examination demonstrated a distended abdomen, auscultation was indicated by hyperactive bowel sounds and the rectal examination revealed empty ampulla recti. Based on these observations, the patient was monitored for a mechanical intestinal obstruction in patient with a previous diagnosis of pulmonary cancer.
Further imaging studies with abdominal computed tomography (CT) scan, showed multiple protruding small bowel tumors with entero enteric intussusceptions at three sites, a large omentum metastasis and three liver lesions at III, VII, VIII liver-segments about 22.5 mm, 38 mm, 32 mm in diameter.
The patient underwent emergency laparotomy. Intussusceptions were found in three different regions of the small bowel loops.
Three intestinal resections were performed. The largest one, about 80 cm long, contained ten polypoid lesions found by palpation before resection. The other two sections of bowel (5 and 4 cm long, respectively) showed other two polypoid lesions with a diameter of 3.5 cm and 3 cm. The duration of surgery it was been 1 h and 30 min.
Pathology showed tumor cell infiltration through the whole thickness of the bowel wall in all ten tumors. They contained both epithelial and mesenchymal elements. The immunohistochemical staining results showed that it was positive for cytokeratin (CK), vimentin, CD-34, and LIS; CK7 was focally positive; and CD117, CD20, and desmine were negative. The final diagnosis was metastatic small bowel carcinosarcoma with a lung primary.
Unfortunately, our patient had a complicated postoperative course in the intensive care unit, he has developed pneumonia with Acinetobacter.
He was died 8 days after the surgery.
3. Discussion
Adult intussusceptions are rare and it constitute 5% of all invaginations and less then 1% of all mechanical bowel obstruction [12,13]. The types of intussusception were classed in according to their benign or malignant etiology.
Benign causes included: ileum polyp (41%), idiopathic (13%), parasite (2%), Merkel’s diverticula (2%).
Malignant causes included: cecal adenocarcinoma (26%), sigmoid adenocarcinoma (4%), ileum adenocarcinoma (2%), rhabdomyosarcoma (2%), ileum mucinous adenocarcinoma (2%).
Adult intestinal intussusceptions attributed to metastasize Lung’s Carcinoma are extremely rare; from 1965 to 2012 were reported 16 cases and only two of these was related to sarcomatoid carcinoma of the lung.
This presentation shows the third case in literature.
In the present case, initial symptoms were chest pain, hemoptysis, and fever that allowed the diagnosis of lung cancer and only later was presented with an intestinal obstruction by G-I metastasis. However it is not uncommon that the early symptoms of lung cancer are associated to metastasis. Every type of lung cancer can result in GI metastasis and the most common site of metastatic lung cancer in the GI tract is small bowel [14]. In generally the lung carcinoma can metastasize to the small intestine via the hematogenous or lymphogenous paths (via the thoracic duct probably) and the immunohistochemical stains has an important role in the diagnosis, the positivity with vimentin, cytokeratin AE1/AE3 and CK7 are important in differential diagnosis from other malignant pathologies [15]; in our case the intestinal intussusceptions were caused by metastasis from lung carcinosarcoma, which was positive for CK7, vimentin, CD34, and LIS.
Lung carcinosarcoma is a high grade biphase neoplasm with both epithelial and mesenchimal components. It usually affect men with a smoking history in the fifth and eighth decade of life and is often refractory to chemioradiation therapy. It account for less that 1% of all primary pulmonary neoplasm [16,17]. The diagnosis is often made at a late stage when there are multiple metastasis. The survival rate at six months is only around 27% [18]. However, intussusception is a rare presentation of metastatic pulmonary carcinosarcoma.
In our case of small bowel metastasis, our patient required surgery to relieve the obstruction, in presence of malignity, resection and primary anastomosis is the treatment of choice. Due to the tendency of metastasis to occur at multiple sites, the palpation of all intestinal segments is important to identify the intraluminal lesions and to resect the affected bowel segments like our case.
Consequently, surgical treatment still plays an important role in lung cancer patients with GI metastasis that cause bowel obstruction, perforation, or massive hemorrhage.
4. Conclusion
In summary, there are rare reports of small intestinal intussusceptions caused by metastatic lung carcinosarcoma [19] and surgical treatment is worthwhile in a select group of patients with bowel obstruction or perforation. Physicians should be more alert to symptoms or signs indicating GI metastasis in patients with a history of lung cancer because early suspect and diagnosis may allow elective and less aggressive surgical approaches.
Contributor Information
Angela Romano, Email: angelaromano_ar@libero.it.
Michele Grassia, Email: michelegrassia@live.it.
Amalia Rosaria Rita Rossetti, Email: amaliarosariarita.rossetti@gmail.com.
Giuseppe Esposito, Email: g-expo@libero.it.
Bartolomeo Braccio, Email: braccio.bartolomeo@email.it.
Modestino Pezzella, Email: ninopezze@gmail.com.
Francesco Torelli, Email: francesco.torelli@unina2.it.
Giuseppe Izzo, Email: giuseppe.izzo@unina2.it.
Roberto Alfano, Email: roberto.alfano@unina2.it.
Natale Di Martino, Email: angelaromano_ar@libero.it.
References
- 1.Terzi A., Gorla A., Piubello Q. Biphasicsarcomatoid carcinoma of the lung: report of five cases and review of the literature. Eur. J. Surg. Oncol. 1997;23:457. doi: 10.1016/s0748-7983(97)93733-1. [DOI] [PubMed] [Google Scholar]
- 2.Fishback N.F., Travis W.D., Moran C.A. Pleomorphic (spindle/giant cell) carcinoma of the lung. A clinicopathologic correlationof 78 cases. Cancer. 1994;73:2936–2945. doi: 10.1002/1097-0142(19940615)73:12<2936::aid-cncr2820731210>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 3.Kim T.H., Kim S.J., Ryu Y.H., Lee H.J., Goo J.M., Im J.G. Pleomorphic carcinoma of lung: comparison of CT features and pathological findings. Radiology. 2004;232:554–559. doi: 10.1148/radiol.2322031201. (PubMed) [DOI] [PubMed] [Google Scholar]
- 4.Travis W.D. Sarcomatoid neoplasms of the lung and pleura. Arch. Pathol. Lab. Med. 2010;134:1645–1658. doi: 10.5858/2010-0086-RAR.1. (PubMed) [DOI] [PubMed] [Google Scholar]
- 5.Koss M.N., Hochholzer L., Frommelt R.A. Carcinosarcomas of the lung: a clinicopathologic study of 66 patients. Am. J. Surg. Pathol. 1999;23:1514–1526. doi: 10.1097/00000478-199912000-00009. [DOI] [PubMed] [Google Scholar]
- 6.Yoshino N., Kubokura H., Yamauchi S. A true pulmonary carcinosarcoma that required diagnostic differentiation from a pleomorphic adenoma: a case report. Ann. Thorac. Cardiovasc. Surg. 2009;15:42–45. [PubMed] [Google Scholar]
- 7.Kim H.M., Shin B.S., Song Y.W. A case of pulmonary carcinosarcoma with persistent mild fever. Kor. J. Int. Med. 2002;17:78–82. doi: 10.3904/kjim.2002.17.1.78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.McNeill P.M., Wagman L.D., Neifeld J.P. Small bowel metastases from primary carcinoma of the lung. Cancer. 1987;59:1486–1489. doi: 10.1002/1097-0142(19870415)59:8<1486::aid-cncr2820590815>3.0.co;2-w. [DOI] [PubMed] [Google Scholar]
- 9.Berger A., Cellier C., Daniel C., Kron C., Riquet M., Barbier J.P., Cugnenc P.H., Landi B. Small bowel metastases from primary carcinoma of the lung: clinical findings and outcome. Am. J. Gastroenterol. 1999;94:1884–1887. doi: 10.1111/j.1572-0241.1999.01224.x. [DOI] [PubMed] [Google Scholar]
- 10.Antler A.S., Ough Y., Pitchumoni C.S., Davidian M., Thelmo W. Gastrointestinal metastases from malignant tumors of the lung. Cancer. 1982;49:170–172. doi: 10.1002/1097-0142(19820101)49:1<170::aid-cncr2820490134>3.0.co;2-a. [DOI] [PubMed] [Google Scholar]
- 11.Braham E., Rejeb H.B., Aouadi S., Kilani T., El Mezni1 F. Pulmonary carcinosarcoma with heterologous component: report of two cases with literature review. Ann Transl Med. 2014;4(April (2)):41. doi: 10.3978/j.issn.2305-5839.2014.02.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Annual cancer report from Taiwan Cancer Registry database, Department of health. Taipei (Taiwan), (2010) 36–45.
- 13.Woods J.M., Koretz M.J. Emergency abdominal surgery for complications of metastatic lung carcinoma. Arch. Surg. 1990;125:583–585. doi: 10.1001/archsurg.1990.01410170029005. [DOI] [PubMed] [Google Scholar]
- 14.Lee P.C., Lo C. Role of surgical intervention in managing gastrointestinal metastases from lung cancer. World J. Gastroenterol. 2011;17(October (38)):4314–4320. doi: 10.3748/wjg.v17.i38.4314. ISSN: 1007-9327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Reid-Nicholson M., Idrees M., Perino G., Hytiroglou P. Sarcomatoid carcinoma of the small intestine: a case report and review of the literature. Arch. Pathol. Lab. Med. 2004;128(8):918–921. doi: 10.5858/2004-128-918-SCOTSI. [DOI] [PubMed] [Google Scholar]
- 16.Langer F., Wintzer H.O., Werner M. A case of pulmonary carcinosarcoma (squamous cell carcinoma and osteosarcoma) treated with cisplatin and doxorubicin. Anticancer Res. 2006;26:3893–3897. [PubMed] [Google Scholar]
- 17.Goto T., Maeshima A., Tajima A. A resected case of pulmonary carcinosarcoma. Ann. Thorac. Cardiovasc. Surg. 2010;16:190–193. [PubMed] [Google Scholar]
- 18.Vidal-Losada M.J., Bernal-Monterde V., Amores-Arriaga B. Lung carcinosarcoma. Clin. Transl. Oncol. 2010;12:303–305Koss. doi: 10.1007/s12094-010-0508-6. [DOI] [PubMed] [Google Scholar]
- 19.Hochholzer L., Frommelt R.A. Carcinosarcomas of the lung: a clinicopathologic study of 66 patients. Am. J. Surg. Pathol. 1999;23:1514–1526. doi: 10.1097/00000478-199912000-00009. [DOI] [PubMed] [Google Scholar]