

Highlights
-
•
Gastrostomy can be a necessity in a variety of clinical situations either for nutrition or for gastrointestinal discharge.
-
•
There are two major techniques: open gastrostomy and minimally invasive gastrostomy.
-
•
We describe herein a technique of laparoscopic-assisted percutaneous endoscopic gastrostomy (LAPEG) in 2 cases with different primary pathologies and unsuccessful attempt of Percutaneous endoscopic gastrostomy as the first intention.
-
•
LAPEG might be an interesting option by minimizing the risk of intestinal injury and might be a faster and easier procedure than laparoscopic gastrostomy, and should be considered for selected cases.
Keywords: Gastroscopy, Gastrostomy, PEG, Laparoscopy
Abstract
Introduction
Percutaneous endoscopic gastrostomy (PEG) is a common procedure to obtain a feeding tube. However, this technique might imply several difficulties and complications. The inability to transilluminate the abdominal wall may occur frequently, especially in obese or multi-operated patients. With the emergence of minimally invasive surgery, laparoscopic-assisted percutaneous endoscopic gastrostomy (LAPEG) might provide a safe and efficient alternative.
Presentation of cases
We report hereby two cases of patients having undergone LAPEG in our institution. Conventional PEGs were deemed impossible because of the absence of transillumination and motivated a surgical approach.
Two obese patients with a Body Mass Index (BMI) of 31 and 45 kg/m2 respectively presented neurological condition (stroke and Parkinson’s disease) requiring a feeding tube. While a PEG was unsuccessful (impossibility to transilluminate), a LAPEG was attempted. The procedure and the recovery were uneventful.
Discussion
There are different techniques for gastrostomy tube placement: open gastrostomy, PEG and radiologic procedure. The PEG is associated with a significant risk of bowel perforation.
LAPEG seems to be an interesting option in order to avoid an open gastrostomy in patients in whom a PEG cannot be performed. This is especially true in obese patients, where a transillumination cannot be performed. It offers an endoscopic view of the stomach simultaneously to the laparoscopic approach that allows a potential decrease of major complications.
Conclusion
While the literature reports mainly pediatric cases, we present herein two successful LAPEG in adult obese patients. In case of impossibility to perform PEG, this technique allows a safe direct visualization of the stomach and other adjacent organs.
1. Introduction
Gastrostomy can be a necessity in a variety of clinical situations either for nutrition or for gastrointestinal discharge [1]. Indeed, there are multiple indications for gastrostomy whether temporary or definitive, in case of swallowing disorders, poor nutritional status requiring long-term nutritional support, or chronic intestinal obstruction necessitating discharge [2,3]. In these situations, the most frequent indications are palliative for example in case of obstructive tumors of the head and the body of the pancreas, laryngeal cancers, cerebral vascular accidents, cranial traumas, and neurodegenerative syndromes [4].
There are two major techniques: open gastrostomy (OG) and minimally invasive gastrostomy, which includes: percutaneous endoscopic gastrostomy (PEG), percutaneous fluoroscopic-guided gastrostomy [5] and more recently laparoscopic gastrostomy and laparoscopic-assisted percutaneous endoscopic gastrostomy (LAPEG) (Fig. 1).
Fig. 1.
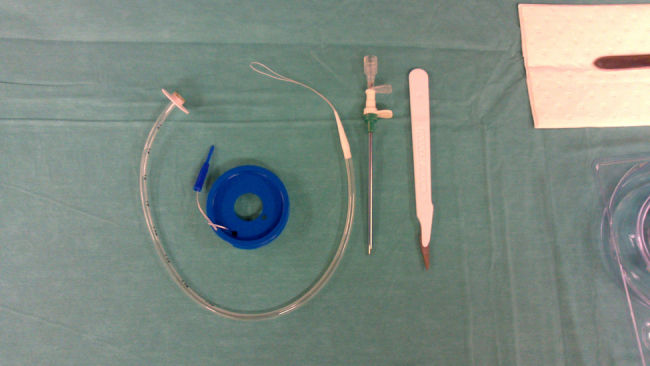
The set used for the LAPEG, consist: a lancet, a guidewire (17 Fr), the gastrostomy catheter (14 Fr/17 cm) and a needle guide with a dilatator (17Fr).
With the increasing acceptance of minimally invasive technique, a substantial decrease of OG was observed. As a consequence, the complication rate associated to laparotomy was reduced as well (pain, abscesses, hematoma, evisceration or incisional hernia) [6]. The LAPEG is a relatively recent option and was first described in 1993 by Raaf et al. [7]. While majority of reports of this technique concerns pediatric patients [2], LAPEG might be an interesting alternative in patients in whom a PEG could not be performed safely (difficulty to transilluminate, risk of intestinal interposition).
We describe herein a technique of LAPEG in 2 cases with different primary pathologies and unsuccessful attempt of PEG as the first intention.
2. Presentation of cases and technique
2.1. Case one
Our first case was a 83-year old male patient presenting a cerebral vascular accident with major swallowing disorder. The endoscopic team attempted a PEG who unfortunately failed because of the absence of transillumination of the abdominal wall. Of note the patient's Body Mass Index (BMI) was 31 kg/m2.
2.2. Case two
Our second patient was a 66-year old female patient, with a past medical history significant for a Parkinson’ disease. The PEG was indicated for a continuous pump of Madopar®. Unfortunately, PEG insertion failed (absence of transillumination). Of note, the patient’s BMI was 45 kg/m2. In these two situations, we decided to perform a LAPEG.
2.3. Technique
Patients were under general anesthesia, in dorsal decubitus. The first 12 mm optical port was inserted by the open technique, through the umbilicus (Fig. 2). The stomach was visualized and positioned correctly for PEG insertion (Fig. 3A). The gastroenterologist proceeded to the gastroscopy simultaneously with insufflation of the stomach. The abdominal insufflation pressure was decreased from 15 mmHg to 10 mmHg. A needle was inserted at the entry point for the PEG (Fig. 3B) (Russel Gastrostomy Set: C-GAST-1700-RFS). A guidewire was placed through the needle (Fig. 4A) and a dilator was placed over the guidewire to create a tract wide enough for the gastrostomy tube (Fig. 4B). The placement of the gastrostomy was checked by laparoscopy and endoscopy (Fig. 4C).
Fig. 2.

A 12-mm umbilical trocar is placed for the laparoscope. After having stomach repair, we perform an abdominal incision opposite the illuminating site.
Fig. 3.

A. Insuflation of the stomach through the endoscope.
B. Direct visualization of the needle into the stomach after a repair of the good localization by transillumination.
Fig. 4.

A. The guidewire is placed through the needle and a dilator is placed over the guidewire.
B. The guidewire allows creating a tract wide enough for the gastrostomy tube.
C. Final result.
The operative time was 35 and 42 min, respectively. There was no intra-operative complication. The postoperative course was uneventful. The length of stay was 1 and 2 days, respectively.
3. Discussion
There are different techniques for gastrostomy tube placement: open gastrostomy, PEG and radiologic procedure. The PEG is associated with a significant risk of bowel perforation. However, the main reason of a failure of the procedure is an inadequate transillumination through the abdominal wall. Moreover, there are also many other factors that could limit PEG insertion such as anatomic variations secondary to gastric surgery, adhesions from previous abdominal surgery, or severe scoliosis [8].
While not completely new, LAPEG seems to be an interesting option in order to avoid an open gastrostomy in patients in whom a PEG cannot be performed. This is especially true in obese patients, where a transillumination cannot be performed. This technique allows viewing the peritoneal cavity and the stomach; firstly to recognize the ideal gastrostomy site and to avoid a potential intestinal perforation; secondly to guarantee a good placement of the gastrostomy tube in the stomach lumen [9]. Several authors have compared the LAPEG with the other percutaneous techniques [3,5,6]. While the complication rate is similar, the success rate is higher by fluoroguidance or laparoscopic-assisted techniques than endoscopy [10]. While the LAPEG procedure takes a longer operative time, the safety seems to be higher than the PEG technique.
On the other hand, it is important to specify that the contraindication for PEG remains relevant during a LAPEG. These include notably stenosis of the oesophagus, total or subtotal gastrectomy, coagulation disorders, and severe respiratory failure. The LAPEG respect the main advantages of the PEG, a low morbidity procedure for gastrostomy tube placement.
One of the main disadvantages of the LAPEG is its costs, which remains higher than the other procedures [4]. Finally there is no study comparing the various minimally invasive approaches for surgical gastrostomy. However, recently, Franken et al. described their experience with laparoscopic gastrostomy (LAG) in children. They showed a significant rate of major complications (2%) including death, postoperative dehiscence of stomach wall, intraoperative bleedings, perforation of adjacent organs, acute intestinal obstruction, volvulus and omental herniation [11]. On the other hand, while requiring two different teams, LAPEG might be not only faster but also safer than the LAG. Indeed, it offers an endoscopic view of the stomach simultaneously to the laparoscopic approach that allows a potential decrease of this kind of complications [4].
4. Conclusion
LAPEG is at present considered as a minimally invasive alternative to the classic percutaneous techniques. It might be safer than the PEG by direct visualization of the inside and the outside of the stomach. And in cases of failure of transillumination, LAPEG might be an interesting option by minimizing the risk of intestinal injury. Finally, LAPEG might be a faster and easier procedure than laparoscopic gastrostomy, and should be considered for selected cases.
References
- 1.Larson D.E.1, Burton D.D., Schroeder K.W. Percutaneous endoscopic gastrostomy: indications, success, complications, and mortality in 314 consecutive patients. Gastroenterology. 1987;93:48–52. [PubMed] [Google Scholar]
- 2.Shimizu Y.1, Okuyama H., Sasaki T. Laparoscopic-assisted percutaneous endoscopic gastrostomy: a simple and efficient technique for disabled elderly patients. JPEN J. Parenter. Enteral. Nutr. 2014;38(May(4)):475–480. doi: 10.1177/0148607113481476. [DOI] [PubMed] [Google Scholar]
- 3.Ozmen M.N.1, Akhan O. Percutaneous radiologic gastrostomy. Eur. J. Radiol. 2002;43(September(3)):186–195. doi: 10.1016/s0720-048x(02)00155-9. [DOI] [PubMed] [Google Scholar]
- 4.Lopes G.1, Salcone M., Neff M. Laparoscopic-assisted percutaneous endoscopic gastrostomy tube placement. JSLS. 2010;14:66–69. doi: 10.4293/108680810X12674612014662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Silas A.M.1, Pearce L.F., Lestina L.S. Percutaneous radiologic gastrostomy versus percutaneous endoscopic gastrostomy: a comparison of indications, complications and outcomes in 370 patients. Eur. J. Radiol. 2005;56(October(1)):84–90. doi: 10.1016/j.ejrad.2005.02.007. [DOI] [PubMed] [Google Scholar]
- 6.Wollman B.1, D’Agostino H.B., Walus-Wigle J.R. Radiologic, endoscopic, and surgical gastrostomy: an institutional evaluation and meta-analysis of the literature. Radiology. 1995;197(December(3)):699–704. doi: 10.1148/radiology.197.3.7480742. [DOI] [PubMed] [Google Scholar]
- 7.Raaf J.H.1, Manney M., Okafor E. Laparoscopic placement of a percutaneous endoscopic gastrostomy (PEG) feeding tube. Laparoendosc. Surg. 1993;3(August(4)):411–414. doi: 10.1089/lps.1993.3.411. [DOI] [PubMed] [Google Scholar]
- 8.Lindberg C.G.1, Ivancev K., Kan Z. Percutaneous gastrostomy: a clinical and experimental study. Acta Radiol. 1991;32:302–304. [PubMed] [Google Scholar]
- 9.Taylor C.A.1, Larson D.E., Ballard D.J. Predictors of outcome after percutaneous endoscopic gastrostomy: a community-based study. Mayo Clin. Proc. 1992;67:1402–1409. doi: 10.1016/s0025-6196(12)61118-5. [DOI] [PubMed] [Google Scholar]
- 10.Barkmeier J.M.1, Trerotola S.O., Wiebke E.A. Percutaneous radiologic, surgical endoscopic, and percutaneous endoscopic gastrostomy/gastrojejunostomy: comparative study and cost analysis. Cardiovasc. Intervent. Radiol. 1998;21(July–August(4)):324–328. doi: 10.1007/s002709900269. [DOI] [PubMed] [Google Scholar]
- 11.Franken J.1, Mauritz F.A., Suksamanapun N. Efficacy and adverse events of laparoscopic gastrostomy placement in children: results of a large cohort study. Surg. Endosc. 2015;29(June(6)):1545–1552. doi: 10.1007/s00464-014-3839-5. [DOI] [PubMed] [Google Scholar]