

Highlights
-
•
This is a case report of hepatic artery injury during left hepatic trisectionectomy for colorectal liver metastasis treated by portal vein arterialization (PVA).
-
•
Fatal liver failure after hepatectomy was avoided by PVA.
-
•
Subsequential portal hypertension was successfully treated by coil embolization of the PVA.
-
•
PVA seems to be the only way to rescue a patient when hepatic artery reconstruction is impossible, it is important for hepatopancreatobiliary surgeons to know this procedure.
Keywords: Portal vein arterialization, Hepatectomy, Colorectal liver metastasis
Abstract
Portal vein arterialization (PVA) has been applied as a salvage procedure in hepatopancreatobiliary surgeries, including transplantation and liver resection, with revascularization for malignancies. Here we describe the use PVA as a salvage procedure following accidental injury of the hepatic artery to the remnant liver occurred during left hepatic trisectionectomy for colorectal liver metastases (CRLM). A 60-year-old man with cancer of the sigmoid colon and initially unresectable CRLM received 11 cycles of hepatic arterial infusion chemotherapy with 5-fluorouracil (1500 mg/week), after which CRLM was downstaged to resectable. One month after laparoscopic sigmoidectomy, a left trisectionectomy and wedge resection of segment 6 were performed. The posterior branch of the right hepatic artery, the only feeding artery to the remnant liver, was injured and totally dissected. Because microsurgical reconstruction of the artery was impossible, PVA was used; PVA is the sole known procedure available when hepatic artery reconstruction is impossible. The patient then suffered portal hypertension, and closure of arterio-portal anastomosis using an interventional technique with angiography was eventually performed on postoperative day 73. Therefore, it is considered that because PVA is associated with severe postoperative portal hypertension, closure of the arterio-portal shunt should be performed as soon as possible on diagnosing portal hypertension.
1. Introduction
Liver resection for colorectal liver metastases (CRLM) provides the only chance of long-term survival, with a 5-year survival rate of 38–58% in selected patients [1–3]. CRLM is initially unresectable in approximately 80–90% of patients [4], but recent improvements in surgical techniques and response rates to chemotherapy have expanded its resectability [5]. However, in such advanced cases, radical liver resection with revascularization of the liver is often required.
Portal vein arterialization (PVA) was originally established as an alternative strategy for preventing liver failure in patients with severe cirrhosis in conjunction with portacaval shunt placement [6]. It has been reported that PVA increases oxygen supply to the portal vein, prevents liver failure, and promotes liver regeneration [7–9]. PVA also has been applied as a salvage procedure in various types of hepatopancreatobiliary surgeries, including transplantation and liver resection, with revascularization for malignancies [10–13]. However, these studies have only included a small number of cases, and very few publications have reported the use of PVA in patients with CRLM who underwent hepatectomy.
Therefore, in this report we describe a case of an accidental injury of the hepatic artery to the remnant liver that occurred during left hepatic trisectionectomy for CRLM and was successfully treated using PVA as a salvage procedure.
2. Case report
A 60-year-old man, in whom multiple liver tumors had been detected by abdominal ultrasonography, was admitted to our hospital. Colonoscopy revealed cancer of the sigmoid colon, and computed tomography (CT) and magnetic resonance imaging (MRI) revealed more than 20CRLMs with the involvement of the root of the left and middle hepatic veins (Fig. 1A, B). We initially diagnosed the patient with unresectable CRLM, and hepatic arterial infusion (HAI) chemotherapy with 5-fluorouracil (1500 mg/week) was initiated. After 11 cycles of HAI, a partial response was achieved (Fig. 1C, D); therefore, we planned resection of the primary sigmoid colon cancer as the first step and hepatectomy as the second step.
Fig. 1.

(A, B) Representative images of abdominal computed tomography (CT) prior to treatment. More than 20 metastatic liver tumors were identified, with involvement of the root of the hepatic veins; (C, D) Representative images of abdominal CT after 11 cycles of hepatic arterial infusion chemotherapy. Tumors in the root of the hepatic veins were diminished, and tumors around the porta hepatis were smaller.
One month after laparoscopic sigmoidectomy, the left trisectionectomy and wedge resection of segment 6 were performed. Intraoperative findings revealed the metastatic liver tumors to be very close to the porta hepatis; furthermore, the separation of the anterior and posterior branches of the right hepatic artery was notably difficult. Finally, the posterior branch of the right hepatic artery, which was the only feeding artery to the remnant liver, was injured and totally dissected. The posterior branch of the portal vein and bile duct were also injured at the same time, and the injured wall of the portal vein was promptly repaired using a 5–0 monofilament nylon needle. A good blood flow in the portal vein to the remnant liver was subsequently confirmed. We then inserted a plastic stenting tube from the stump of the cystic duct to the distal side of the injured portion of the bile duct, and the injured wall of the bile duct was repaired using a 6–0 absorbable monofilament needle. After parenchymal transection, microsurgical reconstruction of the artery by end-to-end anastomosis was attempted. However, injury to the intima on the distal side of the artery was so severe that anastomosis was impossible. To avoid critical postoperative liver failure and subsequent patient death without reconstruction of the feeding artery to the remnant liver, we performed PVA by anastomosis of the right hepatic artery to the portal vein. The right hepatic artery was dissected again at the proximal side from the injured portion and then anastomosed to the frontal side of the portal vein using a 7–0 monofilament nylon needle (Fig. 2A, B). After anastomosis, ultrasonography confirmed an increase in the blood flow of the portal vein (Fig. 2C). The portal venous pressure, which was measured by the insertion of a catheter from the mesenteric vein to the portal vein, was 19 mmHg, which revealed portal hypertension that was not severe enough to require splenectomy. The operative time was 547 min and blood loss was 2141 ml.
Fig. 2.

(A) View of intraoperative findings, showing that the stump of the right hepatic artery was anastomosed to the frontal side of the portal vein with a 7-0 monofilament nylon needle; (B) Schema of intraoperative findings; (C) Pulse Doppler ultrasonography findings for portal vein in the remnant liver. Upper: The right hepatic artery was clamped, and blood flow was observed only in the portal vein. Middle: The portal vein was clamped, and blood flow was observed only from the right hepatic artery. Lower: The right hepatic artery and portal vein were not clamped, and blood flow was observed from the portal vein and the right hepatic artery; (D) Angiography on postoperative day 73. The portal vein was enhanced by blood flow from the right hepatic artery and hepatopetal blood flow was observed.
Patient’s serum aspartate aminotransferase level was elevated to 4500 IU/L on postoperative day (POD) 1, but decreased to less than 100 IU/L immediately thereafter. Portal venous thrombosis in the remnant liver occurred on POD 14 and disappeared gradually after anticoagulant therapy. Total bilirubin (T-bil) increased until POD 20 to a level of 20 mg/dL and then decreased gradually (Fig. 3B). CT on POD 30 revealed splenomegaly, and thrombocytopenia became increasingly severe each day. The platelet count decreased to less than 5 × 104/μL after POD 60 (Fig. 3C).
Fig. 3.

Levels of aspartate aminotransferase (AST), total bilirubin (T-bil), and platelet (PLT) counts in peripheral blood. (A) Level of AST was highest on postoperative day (POD) 1 (4500 IU/L), and it then decreased gradually. On POD 14, thrombosis of the portal vein in the remnant liver occurred, and the level of AST again increased (479 IU/L), after which the level of AST was stable, and there was no increase after the closure of the arterio-portal shunt (APS); (B) Level of T-bil was highest on POD 20 (15.9 mg/dl), after which it decreased gradually, and did not increase after the closure of APS. (C) Platelet count in the peripheral blood was highest on POD 20 (12.2 × 104/μL), after which it decreased gradually because of portal hypertension and splenomegaly; it was less than 5.0 × 104/μL by POD 67. After closure of the APS on POD 73, the PLT count increased gradually and by POD 85 it was 8.5 × 104/μL.
We planned closure of the arterio-portal anastomosis using an interventional technique with angiography. However, before performing the closure, we confirmed collateral blood flow from the subphrenic artery to the remnant liver (Fig. 4A). Following this, the anastomosis was closed by coil embolization (Fig. 4B). The platelet count increased gradually and reached to more than 9 × 104/μL by 3 weeks after the closure of the arterio-portal anastomosis.
Fig. 4.
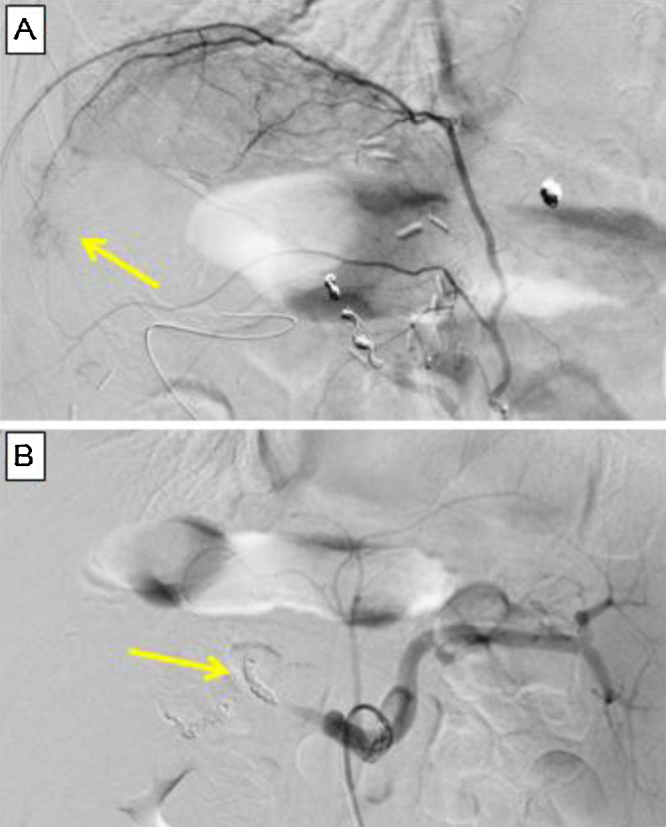
(A) Angiography of the right subphrenic artery. Collateral blood flow to the remnant liver was observed (arrow); (B) Angiography after closure of the arterio-portal anastomosis. The right hepatic artery was occluded by coil embolization (arrow).
Furthermore, the injured wall of the bile duct was repaired using a 6–0 absorbable monofilament needle, and the stenting tube was inserted. After the operation, a culture of the discharge from the stenting tube was checked weekly, and appropriate antibiotics were administered when cholangitis occurred. A cholangiography from the stenting tube revealed a diffuse biliary stricture. The stenting tube was removed on POD 94, after which cholangitis occurred frequently. The patient was eventually discharged on POD 159.
3. Discussion
Since the first report of PVA use in conjunction with portacaval shunting for patients with severe cirrhosis [6], this procedure has been applied as a salvage procedure in various types of hepatopancreatobiliary surgeries. However, although a few publications have reported the use of PVA in auxiliary liver transplantation [14–16], there have been very few reports on the use of PVA in patients with hepatopancreatobiliary malignancies. For example, Kondo et al. [11] reported 10 cases of the use of PVA to achieve complete resection for biliary cancers, with no cases of postoperative mortality. In addition, a group in France recently reported nine cases of hepatopancreatobiliary malignancies treated with the use of PVA [13]. We previously reported a case in which PVA was used after left trisectionectmy for hilar cholangiocarcinoma with the involvement of the right hepatic artery [17]. However, these reports have only included reference to a small number of patients; therefore, the effectiveness and potential risks of this procedure remain unclear. Several experimental studies have reported that PVA increases the oxygen supply to the portal vein, prevents liver failure, and even promotes liver regeneration [8,18].
In contrast to these postitive reports, it has been reported that PVA is associated with postoperative portal hypertension [17]. Careful attention should be paid to the portal venous pressure during surgery using PVA to avoid postoperative portal hypertension. It has been reported that 90-day mortality is significantly associated with an intraoperative portal vein pressure greater than 21 mmHg after major hepatic resection on a noncirrhotic liver [18], and rebleeding after pericardial devascularization is significantly associated with an intraoperative portal vein pressure that is greater than 22 mmHg [19]. In patients with portal hypertension, splenectomy reduces portal venous pressure by eliminating splenic blood flow [20]. In our case, the intraoperative portal vein pressure was 19 mmHg; however, if the pressure had exceeded 23 mmHg, splenectomy would have been considered. Several clinical and experimental studies have indicated an increased risk of portal hypertension after PVA, which further led to liver failure, ascites, and esophageal varices. Bhangui et al. [13] reported two cases of postoperative portal hypertension after PVA with massive ascites, variceal bleeding, and hyperbilirubinemia. In addition, Iseki et al. [22] reported portal hypertension and esophageal varices after PVA. A recent publication has indicated the complication rate caused by portal hypertension to be as high as 44% after PVA [13]. Portal hypertension is generally observed for 1–2 months after PVA, and it is not resolved until the closure of the arterio-portal shunt. Because there have been only a limited number of reports, the optimal timing of shunt closure remains unknown. Kondo et al. [11] reported that hepatopetal arterial collaterals were confirmed within 1 month, and concluded that the shunt could be closed safely before the appearance of portal hypertension. Young et al. [10] recommended that shunt closure should be performed within 6 weeks after surgery because adequate liver regeneration is likely to have been achieved until that time. We monitored portal venous pressure by inserting a catheter from the mesenteric vein to the portal vein, and because our patient suffered from severe portal hypertension, the closure of the arterio-portal shunt was performed on POD 73.
Liver failure was avoided in the present case by the use of PVA after accidental injury of the hepatic artery to the remnant liver, and subsequential portal hypertension was successfully treated by coil embolization of the PVA. However, liver function did not recover to its preoperative state, and liver regeneration after hepatectomy was extremely poor, with only a 238 ml increase over 3 months. Furthermore, it was not possible to administer adjuvant chemotherapy for CRLM because of repeated episodes of cholangitis. Theoretically, because the main blood supply to the bile duct depends on the hepatic artery, the intrahepatic bile duct may have become ischemic after PVA.
It is considered that PVA is the only available procedure for use in rescuing a patient when hepatic artery reconstruction is impossible; therefore, it is important for the hepatopancreatobiliary surgeons to be familiar with this procedure. In addition, as PVA is associated with severe postoperative portal hypertension, closure of the arterio-portal shunt should be considered as soon as possible if portal hypertension is diagnosed.
Conflict of interest
Daisuke Hokuto and other co-authors have no conflicts of interest.
Funding
None
Ethical approval
This case report is not a research study.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Daisuke Hokuto is first author of this paper. He has written the paper and he was attending surgeon of the patient.
Takeo Nomi is corresponding author of this paper.
Ichiro Yamato, Satoshi Yasuda, Shinsaku Obara, Takatsugu Yamada, Hiromichi Kanehiro are members of medical team of hepatic surgery in Nara medical university, and they have taken charge of management of the patients.
Yoshiyuki Nakajima is a professor of department of surgery, Nara medical university, and he has supervised other authors.
Guarantor
None
Contributor Information
Daisuke Hokuto, Email: hokuto@naramaed-u.ac.jp.
Takeo Nomi, Email: t.nomi45@gmail.com.
Ichiro Yamato, Email: yamato@naramed-u.ac.jp.
Satoshi Yasuda, Email: yasuda@naramed-u.ac.jp.
Shinsaku Obara, Email: shinsaku.o@gmail.com.
Takatsugu Yamada, Email: highnet@naramed-u.ac.jp.
Hiromichi Kanehiro, Email: kanehiro@naramed-u.ac.jp.
Yoshiyuki Nakajima, Email: nakayosh@naramed-u.ac.jp.
References
- 1.Abdalla E.K., Vauthey J.N., Ellis L.M. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Ann. Surg. 2004;239:818. doi: 10.1097/01.sla.0000128305.90650.71. 825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Martin L.W., Warren R.S. Current management of colorectal liver metastases. Surg. Oncol. Clin. N. Am. 2000;9:853–876. [PubMed] [Google Scholar]
- 3.Penna C., Nordlinger B. Colorectal metastasis (liver and lung) Surg. Clin. N. Am. 2002;82:1075–1090. doi: 10.1016/s0039-6109(02)00051-8. [DOI] [PubMed] [Google Scholar]
- 4.Evrard S. Limits of colorectal liver metastases resectability: how and why to overcome them? For progress in cancer research. Recent Results Cancer Res. 2014;203:213–229. doi: 10.1007/978-3-319-08060-4_15. [DOI] [PubMed] [Google Scholar]
- 5. Pawlik T.M., Schulick R.D., Choti M.A. Expanding criteria for resectability of colorectal liver metastases. Oncologist. 2008;13:51–64. doi: 10.1634/theoncologist.2007-0142. [DOI] [PubMed] [Google Scholar]
- 6.Otte J.B., Reynaert M., De Hemptinne B. Arterialization of the portal vein in conjunction with a therapeutic portacaval shunt. Hemodynamic investigations and results in 75 patients. Ann. Surg. 1982;196:656–663. doi: 10.1097/00000658-198212001-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nardo B., Montalti R., Puviani L. Portal vein arterialization in a patient with acute liver failure. Transplantation. 2005;79:851–852. doi: 10.1097/01.tp.0000151629.94726.e1. [DOI] [PubMed] [Google Scholar]
- 8.Shimizu Y., Miyazaki M., Shimizu H. Beneficial effects of arterialization of the portal vein on extended hepatectomy. Br. J. Surg. 2000;87:784–789. doi: 10.1046/j.1365-2168.2000.01382.x. [DOI] [PubMed] [Google Scholar]
- 9.Yang W., Koti R., Glantzounis G. Arterialization of the portal vein improves hepatic microcirculation and tissue oxygenation in experimental cirrhosis. Br. J. Surg. 2003;90:1232–1239. doi: 10.1002/bjs.4209. [DOI] [PubMed] [Google Scholar]
- 10.Young A.L., Prasad K.R., Adair R. Portal vein arterialization as a salvage procedure during left hepatic trisectionectomy for hilar cholangiocarcinoma. J. Am. Coll. Surg. 2008;207:e1–e6. doi: 10.1016/j.jamcollsurg.2008.07.019. [DOI] [PubMed] [Google Scholar]
- 11.Kondo S., Hirano S., Ambo Y. Arterioportal shunting as an alternative to microvascular reconstruction after hepatic artery resection. Br. J. Surg. 2004;91:248–251. doi: 10.1002/bjs.4428. [DOI] [PubMed] [Google Scholar]
- 12.Chen Y.L., Huang Z.Q., Huang X.Q. Effect of arterioportal shunting in radical resection of hilar cholangiocarcinoma. Chin. Med. J. (Engl) 2010;123:3217–3219. [PubMed] [Google Scholar]
- 13.Bhangui P., Salloum C., Lim C. Portal vein arterialization: a salvage procedure for a totally de-arterialized liver. The Paul Brousse Hospital experience. HPB (Oxford) 2014;16:723–738. doi: 10.1111/hpb.12200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cavallari A., Nardo B., Caraceni P. Arterialization of the portal vein in a patient with a dearterialized liver graft and massive necrosis. N. Engl. J. Med. 2001;345:1352–1353. doi: 10.1056/NEJM200111013451819. [DOI] [PubMed] [Google Scholar]
- 15.Erhard J., Lange R., Giebler R. Arterialization of the portal vein in orthotopic and auxiliary liver transplantation. A report of three cases. Transplantation. 1995;60:877–879. [PubMed] [Google Scholar]
- 16.Shimizu K., Tani T., Takamura H. Partial portal arterialization in living-donor liver transplantation for hepatic artery occlusion. Transplantation. 2004;77:954–955. doi: 10.1097/01.tp.0000116561.66472.77. [DOI] [PubMed] [Google Scholar]
- 17.Ko S., Nakajima Y., Kanehiro H. Successful management of portal hypertension following artificial arterioportal shunting: report of a case. Surg. Today. 1995;25:557–559. doi: 10.1007/BF00311316. [DOI] [PubMed] [Google Scholar]
- 18.Suzuki O., Takahashi T., Kitagami H. Appropriate blood flow for arterio-portal shunt in acute hypoxic liver failure. Eur. Surg. Res. 1999;31:324–332. doi: 10.1159/000008709. [DOI] [PubMed] [Google Scholar]
- 19.Allard M.A., Adam R., Bucur P.O. Posthepatectomy portal vein pressure predicts liver failure and mortality after major liver resection on noncirrhotic liver. Ann. Surg. 2013;5:822–829. doi: 10.1097/SLA.0b013e3182a64b38. [DOI] [PubMed] [Google Scholar]
- 20.Sun Y.W., Chen W., Luo M. Evaluation of surgical procedure selection based on intraoperative free portal pressure measurement in patients with portal hypertension. Hepatobiliary Pancreat Dis. Int. 2010;3:269–274. [PubMed] [Google Scholar]
- 22.Iseki J., Touyama K., Noie T. Partial portal arterialization for the prevention of massive liver necrosis following extended pancreatobiliary surgery: experience of two cases. Surg. Today. 1992;22:568–571. doi: 10.1007/BF00308907. [DOI] [PubMed] [Google Scholar]