

Abstract
Background
It is important to educate families of pediatric patients with atopic dermatitis (AD) so that they have a correct understanding of AD.
Objective
The purpose of this study is to introduce, evaluate, and improve our family-engaged educational program.
Methods
Children suffering from AD and their families have participated in a half-day educational program called "AD school" with catchy slogans such as "Enjoy with AD Families!" every year since 2005. Educational lectures were conducted for parents. For children with AD, various entertaining programs were provided. A feedback survey about AD school was administered for the purpose of evaluation.
Results
A total of 827 people (376 patients and 451 family members) participated in this program over 7 years. On-site surveys showed a positive response (i.e., "excellent" or "good") for the prick test (95.1%), emollient education (78.4%), educational lecture (97.0%), drawing contest and games (90.2%), and recreation (magic show; 99.0%) respectively. Telephone surveys one year later also elicited a positive response.
Conclusion
We herein introduce the experience of a half-day, family-engaged educational program for AD. Family-engaged education programs for AD such as this AD school encourage and validate family participation in the treatment of their children's AD.
Keywords: Atopic dermatitis, Education, Family, Survey
INTRODUCTION
Atopic dermatitis (AD) is a common, chronically relapsing inflammatory skin disease caused by multiple genetic and environmental factors1. Long-term and persistent management of AD is necessary; therefore, AD families and society experience a significant economic burden2. The chronically relapsing nature of this disease and unsatisfactory treatment experiences cause frustration and disappointment in patients and their family members, which in turn may negatively influence the course of the disease3. However, AD families frequently do not know much about the illness or its consequences. From this point of view, one of the most important considerations is family education in the proper treatment of AD. In addition, children with AD have a fear of hospitals. Therefore, for children, it is important to reduce the fear of hospital visits.
We herein introduce an annual half-day, family-engaged educational program entitled "AD School in Daegu-Gyeongbuk, South Korea" with the slogan, "Enjoy with AD Families!" Our AD school has three characteristics that differentiate it from other AD educational programs. First, not just one organization but all of the local university hospitals came together for this program. This enabled us to easily recruit patients with AD and their family members, and to develop a sense of cooperation. Second, for maximum efficiency, educational sessions were conducted for parents only and entertainment was designed specifically for children with AD. Third, we performed on-site surveys and follow-up telephone surveys (years later) for the purpose of evaluating and improving our program. The purpose of this study is to introduce our half-day educational program for pediatric patients with AD and their family members, and to evaluate the impact of our program based on the on-site and telephone surveys.
MATERIALS AND METHODS
Participants
Children with AD (between 3 and 10 years of age) and their family members participated. All participants were asked for their verbal informed consent. AD was diagnosed by dermatologists and the severity of AD was not considered. A total of 827 people (376 patients and 451 family members) took part in this program over 7 years (2005~2011).
AD school programs
AD school was held as an annual continuing educational program on a Saturday afternoon. The program composed of eight sessions, including a skin prick test, emollient education, educational lectures, and recreation (Fig. 1, Table 1).
Fig. 1. Composition of our atopic dermatitis (AD) school program. (A) Dermatology residents explain the appropriate application method for emollients. (B) Dermatology residents conduct skin prick tests and explain the results of these tests. (C) While parents listen to educational lectures, children with AD play games in another room. (D) A professional magician performs a magic show.

Table 1. An overview of activities including guides, participants, and durations.
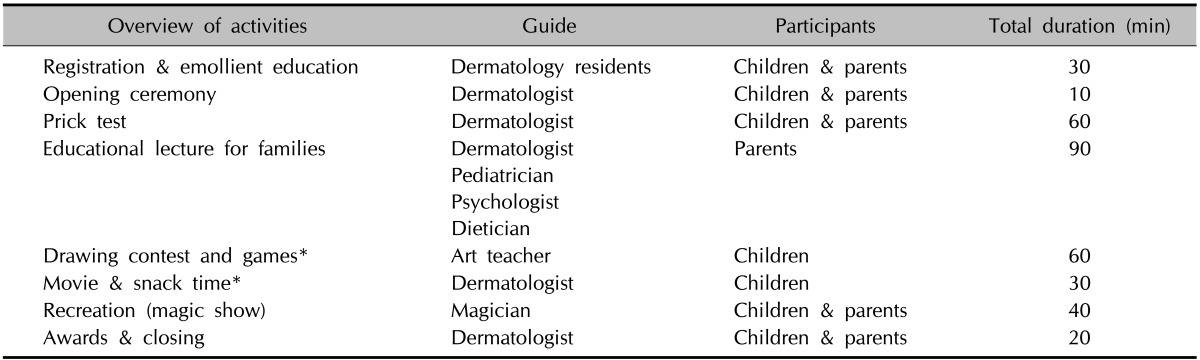
*While parents listened to educational lectures, children participated in a drawing contest, watched a movie, and had snacks in another room.
1) Registration and emollient education
At the registration area, children with AD and their families received nametags and token gifts such as colored pencil sets. After registration, families participated in an emollient education program, in which dermatologists explained the appropriate application method for an emollient.
2) Opening ceremony
After the emollient education, participants attended the opening ceremony, which conveyed a positive image of the event. During the opening ceremony, the goal of the program and its connections to the academic community (and thus its reliability) were described to participants.
3) Skin prick test
Dermatology residents conducted skin prick tests and explained the results. Skin prick tests were performed using a battery of the four common allergens (milk, egg, peanut, and house dust mite). Skin prick tests can be helpful for daily functioning in that they provide information about substances that patients should avoid. Emergency medical kits were prepared in case of accidents during the skin prick tests. However, the emergency situation did not occur even once.
4) Educational lecture
Educational lectures were presented to parents on general topics pertaining to AD, such as "Causes, management, treatment, and symptoms of AD." Special topics, such as "Psychological approaches to AD" were also presented.
5) Drawing contest and games
While parents participated in educational lectures, children participated in a drawing contest in another room. Kindergarten teachers were present to supervise playtime.
6) Movie and snack time
After the drawing contest, children watched animated movies and had snacks.
7) Recreation (magic show)
A professional magician was invited to present a magic show to help parents and children relax.
8) Awards and closing
Awards were presented for the drawing contest and a photo was taken.
On-site and telephone surveys
During AD school, an on-site survey was conducted using questionnaires assessing satisfaction with AD school as well as with each specific session. In addition, after more than a year had passed, a telephonic interview assessed satisfaction with AD school, disease progression, overall effect on life (comprehension/improvement/management of the disease), and willingness to participate again in AD school.
RESULTS
Participant surveys
1) On-site survey
The on-site survey was conducted with a subset of the participants. One of the family members (a caregiver) participated in the on-site survey. Therefore, results were obtained from 102 participants. The satisfaction rate (i.e., "excellent" or "good" responses) was 95.1% for the skin prick test session, 78.4% for the emollient education session, 97.0% for the educational lecture, 90.2% for the drawing contest and games session, and 99.0% for the recreational session (magic show). When compared to the other sessions, the satisfaction rate for the emollient education session was relatively low (Table 2).
Table 2. Satisfaction with atopic dermatitis school: on-site survey (n=102).

Values are presented as participant number (%).
2) Follow-up telephone survey
We obtained telephone survey results from 96 family members.
Satisfaction with AD school
In terms of overall satisfaction with AD school, 99.0% found it helpful, and 94.8% found it enjoyable (Table 3).
Table 3. Satisfaction with atopic dermatitis school: follow-up telephone survey (n=96).
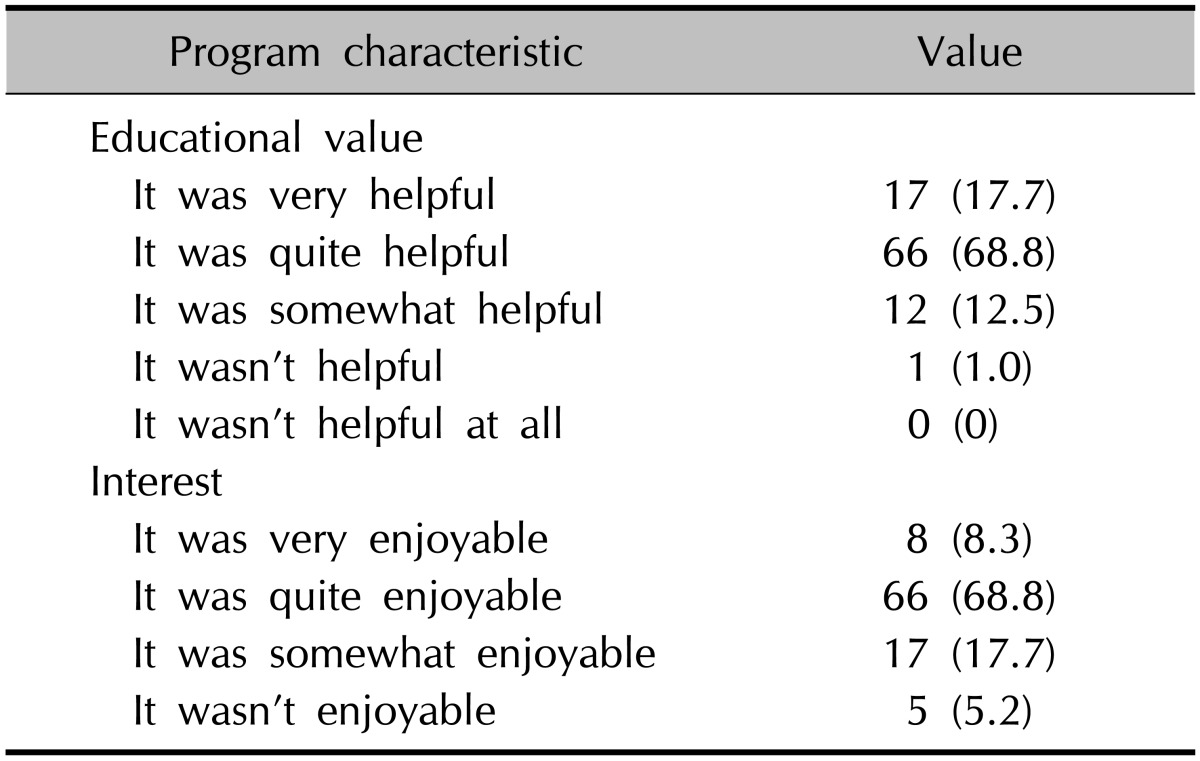
Values are presented as participant number (%).
Disease progression and overall effect on life
In terms of disease progression and effects on life since AD school, 69.8% of parents agreed that their understanding of the disease had improved, 34.4% agreed that they had changed their frequency of using complementary and alternative medicine, and 56.3% agreed that they had tried to improve their home environment after AD school. Of the children, 55.3% agreed that their disease had improved since AD school, and 50.0% agreed that their attitude toward hospital treatment had improved. However, most children with AD chose a neutral response about the improvement of relationships with friends (75.0%) and learning ability (77.1%). In terms of whether they were trying to apply the ointment/emollient adequately, 83.2% of parents and patients agreed that they did. However, most responded neutrally about whether there were better relationships between family members (Table 4).
Table 4. Comprehension, improvement, and management of the disease: follow-up telephone survey (n=96).
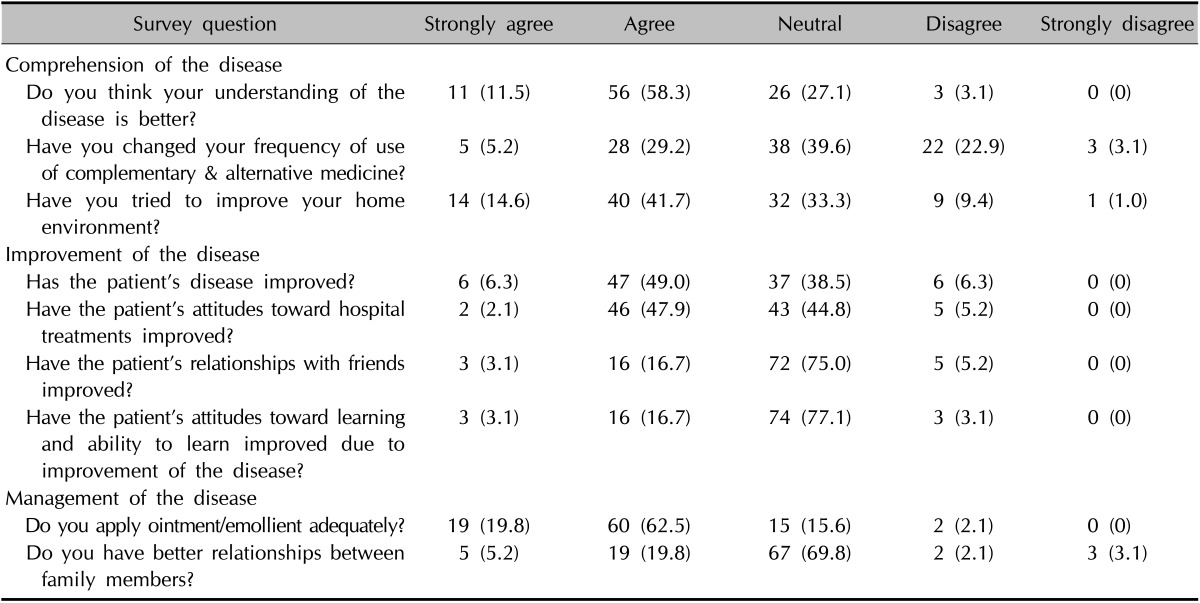
Values are presented as participant number (%).
Willingness to participate again in the AD school
Of all participants, 63.5% were willing to attend the next AD school and 93.8% indicated that they would recommend AD school to their friends or relatives (Table 5).
Table 5. Willingness to participate again in the atopic dermatitis (AD) school: follow-up telephone survey (n=96).
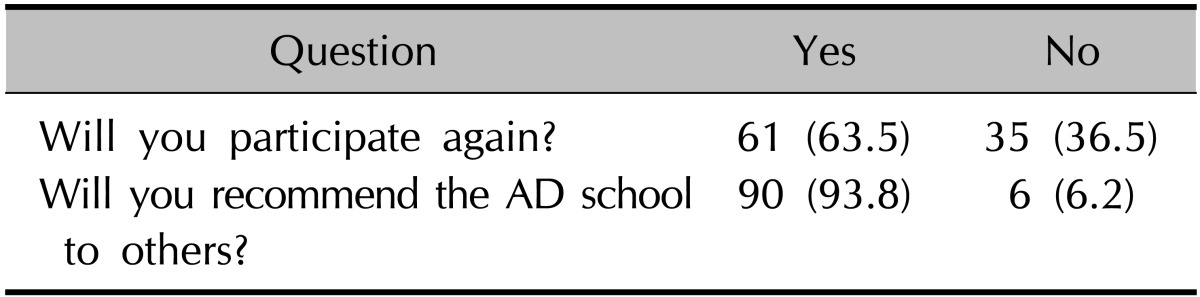
Values are presented as participant number (%).
DISCUSSION
Educational interventions have long been recommended and used as a critical adjunctive treatment method for patients with AD to enhance the effectiveness of therapy2. There are some international studies about educational programs for the management of childhood AD. The Berlin model is a well-known educational program for parents of children with AD. This program aims to improve parents' management skills with regard to their child, and to positively impact the course of the disease as well as the family's quality of life. The program consists of six 2-hour group sessions conducted at weekly intervals. Group sessions are guided by a multi-professional team of pediatricians, psychologists, and dieticians4. The Italian model is another educational program for parents of children with AD. This program consists of six 90-minute weekly meetings involving a pediatric allergist, a dermatologist, and a psychologist5. A 2-hour educational program based on the Australian model was evaluated by comparing a randomized educational intervention group with a control group, with the goal of measuring outcomes of educational interventions including severity of eczema and patient quality of life6. In addition, another Korean study showed positive effects of programmed education delivered by dermatology specialists on the management and knowledge of AD7. Overall, the aforementioned studies are positive because educational programs were shown to contribute toward a comprehensive, family-oriented approach to the management of childhood AD, and are a helpful adjunct to dermatological treatment. However, these programs were family oriented, but not family engaged.
Our AD school is a short half-day educational program for pediatric patients with AD and their families. The main purpose of our AD program is to improve knowledge about the disease, improve parents' management skills with regard to their child with AD, and to positively impact the course of the disease and the family's quality of life. Our AD school became a popular local annual event in Daegu-Gyeongbuk. Through the prick test and emollient education, children with AD and their family members received information about what to avoid and how to correctly use the emollients, which could be helpful in daily life. Educational lectures were provided to adult family members by a multidisciplinary team including dermatologists, pediatricians, psychologists, and dieticians. In contrast with other educational models, we prepared several entertaining programs for children with AD. While parents listened to educational lectures, children enjoyed a drawing contest, a movie, and snacks in another room. Because of this additional program, family members were able to concentrate on the educational lectures and children with AD were able to get to know one another better. The magic show was also prepared to encourage participation and present a positive image for the AD school.
Through on-site surveys, we verified that most participants were satisfied with our program, but that the emollient education session was not perceived as positively as the other sessions. This may be due to people being able to easily get information on how to use emollients correctly, underestimating of its importance, or dis-satisfaction with the explanation. Results from the follow-up telephone survey about overall satisfaction showed that the AD school was helpful, and 94.8% found it enjoyable. Especially in terms of management and comprehension of AD, the disease improved compared to its status before the AD school. This may be because family members not only received information from a variety of professionals, but could also ask any questions about AD. Most of the responses to the follow-up telephone survey about overall effect on life and disease progression were positive, but several parts of the questionnaire showed a pattern of neutral responding (e.g., using complementary and alternative medicine, learning attitude and ability, and the patient's relationship with friends and family members). With regard to the results about complementary and alternative medicines, almost 60% of the total Korean population has been treated by traditional Korean medicine for chronic intractable diseases like AD8. This may be because many Korean people still believe that Oriental medicine is safer than Western medicine.
There are some limitations of our AD school evaluation. First, we did not consider each patient's disease severity, so we could not evaluate improvements in the severity of the disease after AD school. Second, we did not offer a tailored program for each age group, because a relatively wide range of ages (3 to 10 years) participated in the AD school. Third, our educational team, mainly composed of dermatologists, should have been composed of professionals from a greater variety of fields. Adequate educational programs are of great value when offered in cooperation with dermatologists as well as pediatricians, dieticians, psychologists, and nursing staff2. Fourth, the follow-up telephone survey had a low response rate, but we still believe that having this follow-up is valuable. Fifth, because AD school is held only once a year, it may be difficult to change the ingrained habits of families of children with AD. To solve these problems, we are planning to utilize online communication.
In conclusion, even though our AD school for children with AD and their family members is a short half-day program, it contributes to a comprehensive, family-engaged approach to the management of AD and is a helpful adjunct to conventional, stepwise AD treatment.
Our educational program creates an ongoing and comprehensive system for promoting family engagement and improving AD treatment. Therefore, such programs should be considered for integration into routine care.
ACKNOWLEDGMENT
This work was supported by Biomedical Research Institute grant, Kyungpook National University Hospital (2014). This work was supported by The Korean Atopic Dermatitis Association.
References
- 1.James WD, Berger TG, Elston DM. Andrews' disease of the skin: clinical dermatology. 11th ed. Philadelphia, PA: Saunders Elsevier; 2011. pp. 62–70. [Google Scholar]
- 2.Boguniewicz M, Abramovits W, Paller A, Whitaker-Worth DL, Prendergast M, Cheng JW, et al. A multiple-domain framework of clinical, economic, and patient-reported outcomes for evaluating benefits of intervention in atopic dermatitis. J Drugs Dermatol. 2007;6:416–423. [PubMed] [Google Scholar]
- 3.Lambert J, Bostoen J, Geusens B, Bourgois J, Boone J, De Smedt D, et al. A novel multidisciplinary educational programme for patients with chronic skin diseases: Ghent pilot project and first results. Arch Dermatol Res. 2011;303:57–63. doi: 10.1007/s00403-010-1082-z. [DOI] [PubMed] [Google Scholar]
- 4.Wenninger K, Kehrt R, von Rüden U, Lehmann C, Binder C, Wahn U, et al. Structured parent education in the management of childhood atopic dermatitis: the Berlin model. Patient Educ Couns. 2000;40:253–261. doi: 10.1016/s0738-3991(99)00074-9. [DOI] [PubMed] [Google Scholar]
- 5.Ricci G, Bendandi B, Aiazzi R, Patrizi A, Masi M. Three years of Italian experience of an educational program for parents of young children affected by atopic dermatitis: improving knowledge produces lower anxiety levels in parents of children with atopic dermatitis. Pediatr Dermatol. 2009;26:1–5. doi: 10.1111/j.1525-1470.2008.00813.x. [DOI] [PubMed] [Google Scholar]
- 6.Grillo M, Gassner L, Marshman G, Dunn S, Hudson P. Pediatric atopic eczema: the impact of an educational intervention. Pediatr Dermatol. 2006;23:428–436. doi: 10.1111/j.1525-1470.2006.00277.x. [DOI] [PubMed] [Google Scholar]
- 7.Shin JY, Kim do W, Park CW, Seo SJ, Park YL, Lee JR, et al. An educational program that contributes to improved patient and parental understanding of atopic dermatitis. Ann Dermatol. 2014;26:66–72. doi: 10.5021/ad.2014.26.1.66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kim NK, Lee DH, Seo HS, Sun SH, Oh YL, Kim JE, et al. Hwangryunhaedoktang in adult patients with atopic dermatitis: a randomised, double-blind, placebo-controlled, two-centre trial--study protocol. BMC Complement Altern Med. 2011;11:68. doi: 10.1186/1472-6882-11-68. [DOI] [PMC free article] [PubMed] [Google Scholar]