

Abstract
Background:
Scoliosis is a three-dimensional spinal deformity characterized by lateral curvature and rotational deformity of the spine. Various methods have been used to investigate the performance of the subjects during walking with an orthosis, but nobody study the biomechanics of orthotic use by understanding the length of the muscles and the force produced by them. Therefore, the aim of this research is to test the effect of the orthosis on the muscular force, tendon length during walking with and without orthosis.
Materials and Methods:
A 12-year-old scoliosis subject was recruited in this study. The forces produced by trunk musculature, joint reaction force, length of trunk musculature were some parameters selected in this study. Open SIMM and Visual 3D software were used to model the subject.
Results:
The results of this research showed that the length of erector spine muscles increased follow the use of orthosis. Moreover, the force produced by trunk muscles differed during walking with and without orthosis and also between right and left sides.
Discussion:
It seems that Open SIMM software can be used to predict the length of muscles, active-passive forces produced by muscles in scoliotic subjects. Therefore, it is recommended this research be done on more number of subjects.
Keywords: Biomechanics, Opens Simm, orthosis, scoliosis
INTRODUCTION
Adolescent idiopathic scoliosis is a spinal deformity demonstrated by the lateral curvature of the spine associated with the rotational deformity. [1,2] The etiology of this deformity is still controversial. The incidence of this deformity varies between 0.93 in Singapore and 0.12 in Finland. [1,3] Although this disease was reported a long time ago, its etiology is still controversial. A cerebral asymmetry or developmental abnormalities in the central nervous system or weakness of the trunk musculature unilaterally are the mentioned reasons. [1,2,3,4,5] However, unilateral weakness of trunk muscles and/or other abnormalities in trunk muscles have been said to be the main cause of this disorder. [4,5,6] Depends on the severity of this disease, various kinds of treatment have been used including exercise, orthosis, and surgery. [7,8,9,10] The results of some research studies showed that the difference between the mean strength of normal trunks and trunk of patients with idiopathic scoliosis is not significant. Asymmetric trunk muscle activity is also a reason in this regard. [6] The performance of scoliotic subjects has been evaluated in various studies by stability analysis during quiet standing, gait analysis, and by energy consumption. [11,12,13,14] Moreover, various methods are being used to represent the severity of this deformity.
Based on the results of various studies, although there is some asymmetry between the force and moments applied on the right and left legs during walking, there is not any correlation between the severity of scoliosis and gait asymmetry. [4,11] Moreover, the difference between muscles force, length, and myoelectric activities between normal subjects and those with scoliosis has not been supported.
Various orthosis such as Milwaukee, Boston, Rosenberg, Miami, Chenue, symmetric patient-oriented rigid three-dimensional brace, progressive active short brace, and Maastricht orthosis have being used as one of the conservative treatment of scoliosis. [7,10,15,16,17,18,19,20,21,22] The efficacy of these devices on reducing and controlling curve progression is evaluated by taking X-ray and by obtaining Cobb angle. However, there is no research done to check their influences on the trunk muscles function, fiber length and forces, which seems to be the main reasons for this deformity.
Recently we can see lots of improvement in the field of biomechanics, which provide this opportunity to check the performance of muscles during walking, length of muscles fibers and tendon and also the magnitude of power and force produced by different muscles. The use of this method has been reported to evaluate the gait performance of subjects with various musculoskeletal disorders such as osteoarthritis, cerebral palsy, spinal cord injury, and amputees. However, there is no research on scoliotic subjects, which was done by this method of analysis. Therefore, the aim of this research was to evaluate the performance of trunk main musculature during walking with and without orthosis.
MATERIALS AND METHODS
A 12-year-old girl with scoliosis disorder was recruited in this study. She had a double curves scoliosis (a curve between T11-L4 with Cobb angle of 37 in the left side and another curve between T5-T10 with Cobb angle of 34°). The subject was asked to walk with and without Milwaukee brace with a comfortable speed on a level surface. An ethical approval was obtained from Isfahan University of Medical Sciences, Ethical Committee. A consent form was obtained from subject's parent before data collection.
A motion analysis system with 7 high-speed cameras and a Kistler force plate were used to record kinematic and kinetic parameters. Twenty markers were attached on the anterior superior iliac spine, posterior superior iliac spine, medial and lateral epicondyle on both sides (ME, LE), lateral and medial malleolus on both sides (MM, LM), heel, first and fifth metatarsal heads (MT1, MT 5), and acromioclavicular joint on both sides [Figure 1]. The data were collected with 120 Hz and was filtered with a low pass filter (10 Hz). The motion of the markers was recorded by Qualisys Track Manager Software (version 2.7). Visual 3D (produced by C-motion Company, USA) was used to produce a musculoskeletal model of the subject. The output of visual 3D was exported to Open SIMM software (version 3 produced by Stanford University, USA) to check the fiber length, tendon force, and passive force of trunk musculature.[23]
Figure 1.
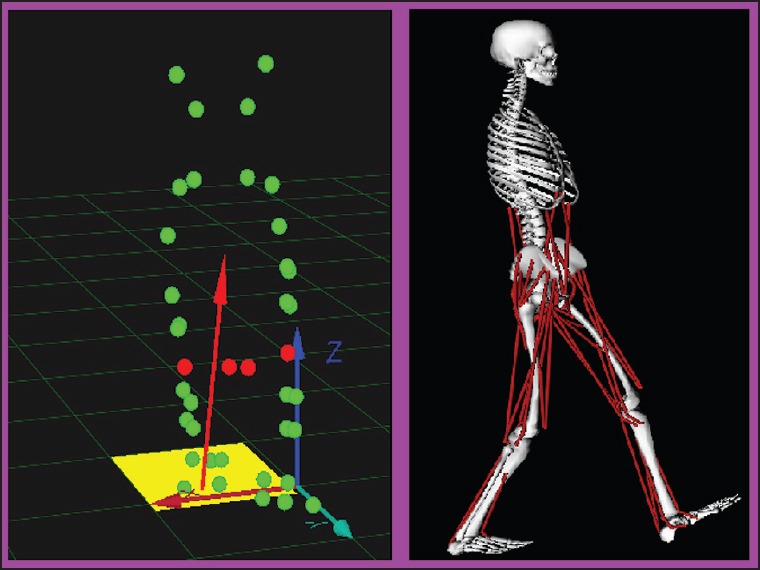
The location of the markers in Qualisys tract manager and the produced Open SIMM model
Some parameters such as spatiotemporal gait parameters (walking speed, stride length, and cadence), joint reaction forces of the hip joint and lumbar, tendon length, fiber length, muscular force, passive force of spinal muscles were evaluated in this study. The difference between mean values of the aforementioned parameters during walking with and without orthosis was evaluated by two sample t-test (the test was repeated to collect 5 successful trials for each condition).
RESULT
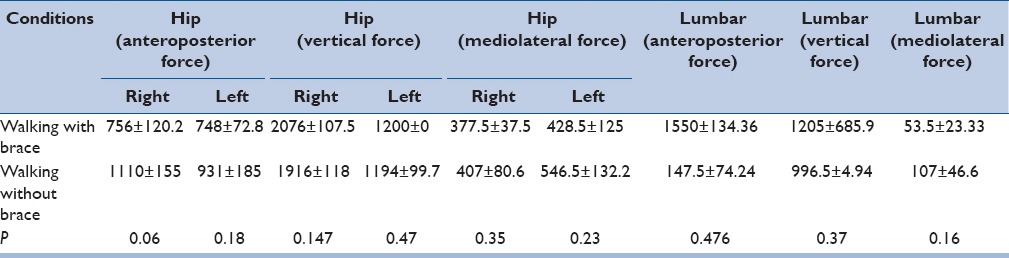
The mean values of walking speed, cadence, and stride length of the subject during walking with and without orthosis were 85 m/min, 104 step/min, and 1.39 m, respectively, compared to 79.2 m/min, 98 step/min, and 1.26 m while walking with brace (the difference between the walking speeds was significant, P < 0.05). The force applied on the hip joint and lumbar was the other selected parameter. There was a significant difference between the anteroposterior shear force of the hip joint in walking with and without orthosis (756 ± 120.2N and 1110 ± 155N in walking with and without orthosis, respectively). Although the vertical force applied on the hip joint decreased in walking with the orthosis, the difference was not significant. Table 1 summarizes the force applied on the hip joint and lumbar in two conditions of walking.
Table 1.
The joint reaction force and hip joint and lumbar during walking with and without orthosis
The fiber length of erector spine was 136 ± 2.8 mm and 135 ± 2.4 mm for walking with orthosis in right and left sides; respectively, compared to 118.7 ± 8.8 mm and 122.2 ± 14.6 mm for walking without the orthosis (the orthosis seems to stretch the erector spine muscles). Table 2 shows the fiber length of trunk musculature while walking with and without the orthosis.
Table 2.
The fiber length of trunk muscles during walking with and without orthosis

The muscle length of erector spine in the right side was 169 ± 4.2 mm and 149.2 mm in walking with and without the orthosis, respectively (P < 0.05). The fiber length in the left side was 163.6 ± 0.919 mm and 152.27 ± 16.6 mm in walking with and without the orthosis, respectively. As can be seen, using the orthosis increased the muscle lengths in the right side and decreased them in the left side [Table 3].
Table 3.
The muscle length (including fiber and tendon lengths) of trunk muscles during walking with and without orthosis

The force produced by trunk musculature was the other parameter selected in this study. Nearly 425 ± 247.5N and 505 ± 275.7N force were produced by right and left erector spine musculatures. The force of other trunk musculature are shown in Table 4 (the difference between the mean values in walking with and without the orthosis was not significant).
Table 4.
The force produced by trunk muscles (passive and active forces) during walking with and without orthosis

The passive forces of erector spine, external oblique, and internal oblique are summarized in Table 5. Although, the orthosis influenced the passive forces of trunk musculature the difference was not significant (P > 0.05).
Table 5.
The passive force of trunk muscles during walking with and without orthosis

DISCUSSION
A lot of reasons have been mentioned regarding the etiology of scoliosis. Unilateral weakness of trunk muscles has been said to be a cause of scoliosis. The results of various research studies showed no consistent difference in the mean strength of trunk musculature in the right and left sides and also between treated and untreated trunk. [24] Type of fiber of trunk musculature (multifidus) also differs between convex and concave sides. Various methods have been used to study scoliosis, however, there is no research done with the use of Open SIMM software. Open SIMM is a new method developed to analysis the performance of the neuromuscular system. It is possible to measure the tendon length of muscles, active and passive force produced by muscle and also to measure the fiber length of muscles. [23] Therefore, the aim of this study was to analysis the aforementioned parameters by use of this method.
Table 1 summarized the force applied on the hip and lumbar in walking with and without the orthosis. The results showed that the shearing force decreased follow the use of the orthosis (it should be mentioned that this is a case study). It means that use of orthosis improved the symmetry of load applied on the structure.
The active and passive forces of trunk muscles were also measured in this study. As can be seen from Tables 4 and 5, the force produced by erector spine in both sides increased but the force of internal oblique and external oblique decreased. It may be concluded that use of the orthosis could influence the action of trunk musculature.
One of the performances of scoliosis braces mentioned in the literature is stretching the spine structure. In other words, they produce a traction force. As can be seen from Tables 2 and 3 the length of fiber of trunk muscles was influenced by the use of the orthosis. The length of erector spine increased in both sides. In contrast, the length of internal oblique and external oblique abdominalis increased in the right side and decreased in left side follow the use of the orthosis. This may represent that the orthosis stretched the back muscles and influenced the anterior side muscles due to their role on improving the rotation symmetry of the spine.
There are some limitations, which need to be acknowledged. The first limitation is that this is a case study and only one orthosis was selected. The second limitation is that the performance on the orthosis was only evaluated during walking. Therefore, it is recommended that a new study is done on a big number of subjects and with the various orthosis.
CONCLUSION
This is the first study done with Open SIMM. The results of this study showed that use of orthosis may influence the length of trunk musculature and the force produced by the trunk muscles.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Rogala EJ, Drummond DS, Gurr J. Scoliosis: Incidence and natural history. A prospective epidemiological study. J Bone Joint Surg Am. 1978;60:173–6. [PubMed] [Google Scholar]
- 2.Nachemson A, Sahlstrand T. Etiologic factors in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 1977;2:176–84. [Google Scholar]
- 3.Ma X, Zhao B, Lin QK. Investigation on scoliosis incidence among 24,130 school children. Zhonghua Liu Xing Bing Xue Za Zhi. 1995;16:109–10. [PubMed] [Google Scholar]
- 4.Mahaudens P, Banse X, Mousny M, Detrembleur C. Gait in adolescent idiopathic scoliosis: Kinematics and electromyographic analysis. Eur Spine J. 2009;18:512–21. doi: 10.1007/s00586-009-0899-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Reuber M, Schultz A, McNeill T, Spencer D. Trunk muscle myoelectric activities in idiopathic scoliosis. Spine (Phila Pa 1976) 1983;8:447–56. doi: 10.1097/00007632-198307000-00002. [DOI] [PubMed] [Google Scholar]
- 6.Haderspeck K, Schultz A. Progression of idiopathic scoliosis: An analysis of muscle actions and body weight influences. Spine (Phila Pa 1976) 1981;6:447–55. [PubMed] [Google Scholar]
- 7.Blount WP. Non-operative treatment of scoliosis with the Milwaukee brace. Manit Med Rev. 1965;45:478–80. [PubMed] [Google Scholar]
- 8.Blount WP, Schmidt AC, Keever ED, Leonard ET. The Milwaukee brace in the operative treatment of scoliosis. J Bone Joint Surg Am. 1958;40-A:511–25. [PubMed] [Google Scholar]
- 9.Chow DH, Leung DS, Holmes AD. The effects of load carriage and bracing on the balance of schoolgirls with adolescent idiopathic scoliosis. Eur Spine J. 2007;16:1351–8. doi: 10.1007/s00586-007-0333-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.De Mauroy JC, Lecante C, Barral F. “Brace Technology” thematic series - The lyon approach to the conservative treatment of scoliosis. Scoliosis. 2011;6:4. doi: 10.1186/1748-7161-6-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chen PQ, Wang JL, Tsuang YH, Liao TL, Huang PI, Hang YS. The postural stability control and gait pattern of idiopathic scoliosis adolescents. Clin Biomech (Bristol, Avon) 1998;13:S52–8. doi: 10.1016/s0268-0033(97)00075-2. [DOI] [PubMed] [Google Scholar]
- 12.Chockalingam N, Dangerfield PH, Rahmatalla A, Ahmed el-N, Cochrane T. Assessment of ground reaction force during scoliotic gait. Eur Spine J. 2004;13:750–4. doi: 10.1007/s00586-004-0762-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chockalingam N, Rahmatalla A, Dangerfield P, Cochrane T, Ahmed el-N, Dove J. Kinematic differences in lower limb gait analysis of scoliotic subjects. Stud Health Technol Inform. 2002;91:173–7. [PubMed] [Google Scholar]
- 14.Gelalis ID, Ristanis S, Nikolopoulos A, Politis A, Rigas C, Xenakis T. Loading rate patterns in scoliotic children during gait: The impact of the schoolbag carriage and the importance of its position. Eur Spine J. 2012;21:1936–41. doi: 10.1007/s00586-012-2328-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Aulisa AG, Mastantuoni G, Laineri M, Falciglia F, Giordano M, Marzetti E, et al. Brace technology thematic series: The progressive action short brace (PASB) Scoliosis. 2012;7:6. doi: 10.1186/1748-7161-7-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Aulisa L, Lupparelli S, Pola E, Aulisa AG, Mastantuoni G, Pitta L. Biomechanics of the conservative treatment in idiopathic scoliotic curves in surgical “grey-area”. Stud Health Technol Inform. 2002;91:412–8. [PubMed] [Google Scholar]
- 17.Grivas TB, Bountis A, Vrasami I, Bardakos NV. Brace technology thematic series: The dynamic derotation brace. Scoliosis. 2010;5:20. doi: 10.1186/1748-7161-5-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Negrini S, Marchini G, Tessadri F. Brace technology thematic series - The Sforzesco and Sibilla braces, and the SPoRT (Symmetric, Patient oriented, Rigid, Three-dimensional, active) concept. Scoliosis. 2011;6:8. doi: 10.1186/1748-7161-6-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Noonan KJ, Weinstein SL, Jacobson WC, Dolan LA. Use of the Milwaukee brace for progressive idiopathic scoliosis. J Bone Joint Surg Am. 1996;78:557–67. doi: 10.2106/00004623-199604000-00009. [DOI] [PubMed] [Google Scholar]
- 20.Van Loon PJ, Roukens M, Kuit JDj, Thunnissen FB. A new brace treatment similar for adolescent scoliosis and kyphosis based on restoration of thoracolumbar lordosis. Radiological and subjective clinical results after at least one year of treatment. Scoliosis. 2012;7:19. doi: 10.1186/1748-7161-7-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Weiss HR. “Brace technology” thematic series - The gensingen brace™ in the treatment of scoliosis. Scoliosis. 2010;5:22. doi: 10.1186/1748-7161-5-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Weiss HR, Werkmann M. Soft braces in the treatment of adolescent idiopathic scoliosis (AIS) - Review of the literature and description of a new approach. Scoliosis. 2012;7:11. doi: 10.1186/1748-7161-7-11. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 23.Delp SL, Anderson FC, Arnold AS, Loan P, Habib A, John CT, et al. Open sim: Open-source software to create and analyze dynamic simulations of movement. IEEE Trans Biomed Eng. 2007;54:1940–50. doi: 10.1109/TBME.2007.901024. [DOI] [PubMed] [Google Scholar]
- 24.Portillo D, Sinkora G, McNeill T, Spencer D, Schultz A. Trunk strengths in structurally normal girls and girls with idiopathic scoliosis. Spine (Phila Pa 1976) 1982;7:551–4. doi: 10.1097/00007632-198211000-00007. [DOI] [PubMed] [Google Scholar]