

Abstract
Objective
Over the past decade, clinical data have accumulated showing that inflammation might contribute to the pathophysiology of suicide. To evaluate the associations and to identify the support for pathways linking inflammatory processes with suicidal behaviour, a comprehensive review of the literature was undertaken.
Method
The search terms ‘cytokine’, ‘risk factors’, ‘kynurenine’, ‘asthma’, ‘allergy’, ‘autoimmunity’, ‘traumatic brain injury’, ‘infection’ along with the terms ‘inflammation’ and ‘suicide’ were entered into PubMed, and a thorough analysis of the publications and their reference lists was performed.
Results
The effects of inflammation on mood and behaviour could partially be mediated by kynurenine pathway metabolites, modulating neuroinflammation and glutamate neurotransmission. At the same time, the triggers of the inflammatory changes documented in suicidal patients may be attributed to diverse mechanisms such as autoimmunity, neurotropic pathogens, stress or traumatic brain injury.
Conclusion
Targeting the inflammatory system might provide novel therapeutic approaches as well as potential biomarkers to identify patients at increased risk. For the goal of improved detection and treatment of suicidal individuals to be achieved, we need to develop a detailed understanding of the origin, mechanisms and outcomes of inflammation in suicidal behaviour.
Keywords: suicide, neuroimmunology, neuroendocrinology, neurobiology, glutamate, inflammation, cytokine, kynurenine, asthma, allergy, autoimmunity, traumatic brain injury, infection
Clinical recommendations.
Clinicians should be aware that medical conditions associated with inflammation and infections can be linked to symptoms of depression and suicidality.
Clinicians should attempt to establish whether any underlying potentially treatable condition is present in patients presenting with suicidal ideation or history of suicidal behaviour.
Treatable somatic conditions linked to depressive and suicidal symptoms include chronic infections, autoimmune disease and certain vitamin deficiencies.
Additional comments.
While there is evidence from both clinical and experimental settings that inflammation can lead to depressive and suicidal symptoms in both clinical and experimental settings, there is still not sufficient data from placebo‐controlled trials indicating that eradicating inflammation will actually reduce the risk of suicide.
The paucity of trials, utilizing available anti‐inflammatory, anticytokine and antibiotic drugs (approved for other indications), may require non‐profit agency sponsorship.
Repurposing of drugs already approved for other conditions might be an important path forward, with the potential of aiding psychiatric patients suffering from treatment‐resistant depressive and suicidal symptoms.
Introduction
Suicide is defined as the intentional termination of one's own life and constitutes the 14th leading cause of global years of life lost 1. According to a recent report by the World Health Organization, over 800 000 deaths by suicide occur around the world each year, but the actual number may be higher 2. Cultural taboos and the fact that suicide is considered a criminal act in some countries may affect the statistical reporting of such events 3. Suicide attempts are estimated to be 10 to 20 times more frequent than the number of completed suicides. Both deaths by suicide and attempts are signs of severe psychological suffering, and a completed suicide carries with it an emotional burden that can impact family for years to come.
The pharmacological treatment of depressed and suicidal individuals has increased over the past decades, but the incidence rates of suicide and suicide attempts are still increasing. A total of 1.5 million people will die from suicide in 2020, if the current trends remain unaltered 4. Accurate suicide risk determination is a very difficult task for clinicians, considering that a patient at high risk for suicide is likely to minimize this symptom. The healthcare system is in many cases unable to accurately detect suicidality, in spite of the fact that almost half of the suicidal patients actually contact healthcare providers in the months prior to their attempt 5. Consequently, there is a great need for both improved methods for the detection of suicide risk and for effective, novel pharmacological treatment options for suicidal patients.
The pharmacological treatment options for suicidal patients today are likely to depend on the patient's primary psychiatric diagnosis and often include antidepressants and anxiolytic medications 6. The positive effects of pharmacotherapy on symptoms of depression take weeks to months to develop, and moreover, there may be an increased risk for suicidal behaviour during this initial period of treatment, especially in children, adolescents and adults up to age 25 7. Besides the conventional antidepressant drugs, clozapine (in schizophrenia) and lithium (in patients with mood disorders) are sometimes indicated specifically for reduction of suicide risk. So‐called treatment‐resistant depression, which often includes symptoms of suicidality, can be treated with electroconvulsive therapy in many countries, in addition to pharmacological treatment. Accumulating studies suggest that subanesthetic doses of intravenous ketamine exerts rapid antidepressant and antisuicidal effects 8, 9. The underlying biological mechanisms by which these treatment options modulate suicidal symptoms are not fully understood.
Aims of the study
The aim of this literature review was to evaluate the associations and to identify the support for pathways linking inflammatory processes with suicidal behaviour, and on the basis of the findings, provide guidance on how to relate to this emerging scientific evidence in clinical practice.
Material and methods
The search terms ‘risk factors’, ‘cytokine’, ‘kynurenine’, ‘asthma’, ‘allergy’, ‘autoimmunity’, ‘traumatic brain injury’, ‘infection’ along with the terms ‘inflammation’ and ‘suicide’ were entered into PubMed, and a thorough analysis of the publications and their reference lists was performed.
Results
Risk factors for suicide
Suicidal behaviour is thought to be driven by complex interactions between genetic predisposition and environmental factors 10. Up to 90% of individuals who complete suicide have an underlying psychiatric disorder, frequently major depressive disorder (MDD) and bipolar disorder 11. Men and women with major depression have a 20.9 and 27.0 standardized mortality ratio for suicide, respectively, and the suicide mortality is approximately 20 fold higher than in the general population 12. However, for the determination of suicide risk in the clinic, the psychiatric history is still of limited value. Currently, a previous suicide attempt is the best predictor of a future completed suicide 13. Certain personality traits, such as impulsivity, aggression 14, 15 and hopelessness 16, are also coupled to an increased risk of suicide. The genetic component of suicidal behaviour has been estimated to be as high as 43% 17. Still, the neurobiological mechanisms involved in suicidal behaviour are poorly characterized. To date, some of the most frequently reported neurobiological changes in suicidal individuals and suicide victims are abnormalities in serotonergic neurotransmission 18 and hypothalamic–pituitary–adrenal (HPA) axis activity 19. As the topic of this review suggests, accumulating evidence indicate that inflammation contributes to the pathophysiology of suicidality.
Evidence of inflammation in suicidality
Treatment with interferon (IFN) for patients with certain forms of cancer and infections is known to induce depression around 1 month after the beginning of medication 20. Such immunotherapy trials indicate a causal relationship between the induced inflammation and subsequent onset of depression. They also provide neurobiological proof of principle that peripheral inflammatory factors can transmit to the central nervous system (CNS), and their levels correlate with depressive symptoms 21, 22. Several case reports also describe the development of suicidal ideation and suicide attempts in this patient population 23, 24. Similarly, suicidal ideation and attempts have been documented in previously psychiatrically healthy patients with multiple sclerosis (MS) during and after treatment with interferon‐β (IFN‐β) 25. In a blinded study that directly confirmed the causality, Reichenberg et al. 26 administered a low dose of lipopolysaccharide (LPS, bacterial endotoxin) or placebo to healthy subjects and found significantly increased depressive symptoms in the LPS‐injected subjects. Over the past years, converging lines of evidence point to inflammation as a possible causal factor, underlying the pathophysiology of suicidality in primary psychiatric patients.
In 1992, an early study discovered increased levels of the soluble interleukin‐2 receptor (IL‐2R) in blood samples from suicide attempters 27. It took more than 15 years for new reports on the topic to follow. Steiner et al. 28 examined the brains of suicide victims for inflammatory changes and found significantly increased microgliosis in the brains of suicide victims with depression and schizophrenia compared to subjects with the same diagnoses who died from other causes. The same year, another group demonstrated increased levels of mRNA transcription for the cytokines interleukin‐4 (IL‐4) and IL‐13 in the orbitofrontal cortical area of suicide victims 29. Supporting these key observations, Lindqvist et al. found elevated cerebrospinal fluid (CSF) levels of IL‐6 in patients who attempted suicide (5.3 ± 3.2; mean ± SEM) compared with healthy controls (0.6 ± 0.1; mean ± SEM). Higher levels of CSF IL‐6 were associated with increasing severity of depression, as evaluated using the Montgomery–Asberg Depression Rating Scale (MADRS; Pearson's r = 0.3; P = 0.016) 30. Recently, increased levels of IL‐1β, IL‐6 and tumor necrosis factor‐α (TNF‐α) at both the mRNA and protein levels were shown in the anterior prefrontal cortex (Brodmann area 10) of teenage suicide victims 31.
Further studies have confirmed that suicidal behaviour is also accompanied by changes in peripheral cytokine levels. The levels of plasma IL‐6 and TNF‐α are increased, and IL‐2 levels are decreased, in suicide attempters compared with both non‐suicidal depressed patients and healthy controls 32. In vitro‐stimulated whole blood from suicidal patients with MDD had a decreased production of both IL‐2 and IL‐6 compared to non‐suicidal MDD patients 33. In agreement with the original postmortem data from Steiner et al. 28, these studies suggest that it might be possible to distinguish suicidal depressed patients from non‐suicidal depressed patients based on peripheral inflammatory markers. However, cytokine levels are known to display a large biological spread, and increased levels of inflammatory markers are also seen in other psychiatric and non‐psychiatric disorders, including PTSD, non‐suicidal depression and neurodegenerative disorders. To circumvent these problems, it is likely that a combination of biomarkers will be required to increase sensitivity and specificity rates for clinical prediction of suicide risk. Additional studies on peripheral cytokines in suicidal patients are clearly needed to establish which biomarkers are most useful. The proteins S100B and C‐reactive protein (CRP) are other peripheral markers of inflammation that increase during injury and inflammation in the CNS. Falcone et al. 34 analyzed serum S100B in teenagers with depression and psychosis and found that the levels were related to the intensity of suicidal ideation irrespective of diagnosis. O'Donovan et al. examined the relation of suicidal ideation to a composite inflammatory index, consisting of CRP, IL‐6, IL‐10 and TNF‐α, in patients with depression. They found that suicidal ideation was significantly associated with an elevated inflammatory index, and this was independent of both the severity of depression and whether the patients had recently attempted suicide 35.
Importantly, a novel meta‐analysis on inflammation in suicidal patients concluded that there are aberrant cytokine levels in blood, CSF and postmortem brain samples from suicidal patients 36. The levels of IL‐1β and IL‐6 were most robustly associated with suicidality, and these cytokines may help distinguish suicidal from non‐suicidal patients. In another review of the inflammatory changes in suicidal subjects, Serafini et al. 37 also concluded that most suicide attempters, or subjects with suicidal ideation, show an imbalance in the immune system, although they stress that cross‐sectional studies are not able to demonstrate causal links between inflammation and suicidality. In support of these meta‐analyses, a recent gene expression study showed that biological mechanisms related to stress, inflammation and apoptosis may underlie suicidality, at least in part 38.
Biological mechanisms underlying suicidal ideation and behaviour
As clearly learned from the IFN treatment studies mentioned above, activation of the immune system can exert profound effects on mood and behaviour. The clinical syndrome ‘sickness behaviour’ is well defined and consists of behavioural and emotional changes that occur in patients and animals in conjunction with a known infectious/inflammatory trigger 39. A number of models have demonstrated how peripherally produced cytokines reach and convey signals to the CNS, including active or passive transportation over the blood–brain barrier (BBB) and by vagus nerve‐mediated signaling 40. Cytokines are also secreted locally, by microglia, astrocytes and endothelial cells in the brain, and play an important role in the development and maintenance of brain function (for review, see Ref. 41). Experimental data show that there are several biological mechanisms by which cytokines could contribute to behavioural and emotional symptoms relevant for suicidality. First, cytokine receptors are present on neurons in specific brain regions in both animals and man. For example, IL‐6 receptors are expressed on serotonergic neurons in the medulla oblongata, as well as in the hypothalamus, hippocampus, cerebellum and selective cortical areas 42, 43. IL‐1β receptors are located on hippocampal, amygdaloid and thalamic neurons, on 5‐HT2 receptor‐expressing neurons in the hypothalamus, and on cerebellar Purkinje cells 44. The presence of cytokine receptors on neurons might indicate that they have specific and direct effects on neuronal function. In fact, IL‐6, IL‐1β and TNF‐α have all been implicated in the regulation of synaptic transmission and plasticity 45, 46. Cytokines can also modulate the concentration of monoaminergic neurotransmitters and their metabolites in various regions of the CNS 47.
There are no animal models that directly mimic human suicidal behaviour. However, suicidal behaviour is thought to depend on several critical personality traits and symptoms, for example aggression and helplessness 48. Animal studies have demonstrated that cytokines might actually influence these key behaviours. IL‐1β, injected into the medial hypothalamus or periaqueductal gray (PAG), acts on 5‐HT2 receptors to potentiate aggressive behaviours in cats 49, 50. IL‐2 injected into the PAG promoted aggression through neurokinin NK 1 receptors 51. TNF‐α is also involved in the regulation of aggression, as TNF‐α receptor deficient mice did not exhibit aggressive behaviour in the resident–intruder test 52. Clinical studies have confirmed that peripheral cytokines are associated with aggression and hopelessness. IL‐6 correlates positively with anger 53, and IL‐1β is associated with hostility in patients with self‐harm 54. Correspondingly, increased anger and hostility were observed in patients with hepatitis C that underwent IFN‐α treatment 55. Higher levels of anger in these patients were found linked to a genetic variability in the TNF‐α gene 56.
A second biological mechanism, which could have profound impact on emotion and behaviour, is the activation of the kynurenine pathway of tryptophan catabolism (Fig. 1). Aberrations in this pathway could constitute a particular pathogenic mechanism linking inflammation and suicidal/depressive symptoms 57. Tryptophan degradation along the enzymatic kynurenine pathway produces several neuroactive compounds, including quinolinic acid (QUIN) and kynurenic acid (KYNA) 58. The pro‐inflammatory cytokines, especially IFN‐γ but also IL‐1β and IL‐6, are potent inducers of indoleamine 2,3 dioxygenase (IDO‐1) and tryptophan 2,3‐dioxygenase (TDO2), two enzymes regulating the first step of the kynurenine pathway 59, 60. As tryptophan is also the precursor of serotonin, inflammation might cause a decrease in serotonin levels by shifting the catabolism of tryptophan to breakdown via the kynurenine pathway 61. This mechanism could potentially contribute to the lowered levels of monoamine metabolites found in CSF of suicide attempters 62. However, it has not yet been firmly established if inflammation does indeed cause depletion of brain tryptophan and serotonin levels in patients with primary depression or suicidality.
Figure 1.
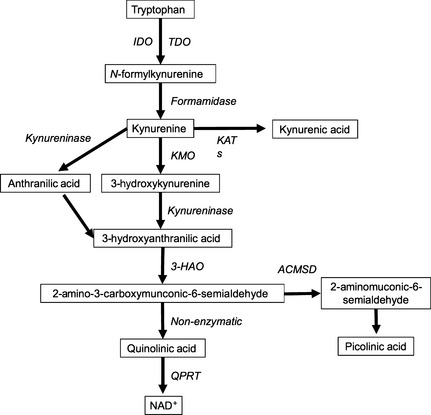
Simplified diagram of the kynurenine pathway. Enzymes in italics and metabolites boxed. Abbreviations: IDO, indoleamine‐2,3‐dioxygenase; TDO, tryptophan‐2,3‐dioxygenase; KAT, kynurenine aminotransferase; KMO, kynurenine‐3‐monooxygenase; 3‐HAO, 3‐hydroxyanthranilate‐3,4‐dioxygenase; ACMSD, aminocarboxymuconate‐semialdehyde decarboxylase; QPRT, quinolinate phosphoribosyltransferase; NAD, nicotinamide adenine dinucleotide.
Interestingly, the kynurenine pathway accounts for over 90% of tryptophan degradation in the periphery 63, and enzymes of this pathway are found in many organs/cell types, including liver, kidney, brain and immune cells. In the brain, the two main branches of the kynurenine pathway are segregated into astrocytes and microglia, with a differential production of metabolites 64. QUIN is an N‐methyl‐d‐aspartic acid (NMDA) receptor agonist, acting through NMDA receptors containing the NR1 + NR2A and the NR1 + NR2B subunits 65, 66. It is formed to a large extent in microglial cells in the brain. KYNA, on the other hand, antagonizes the glycine site of the NMDA receptor, blocks the cholinergic α7 nicotinic receptor (α7nAChR) and is produced by astrocytes 65, 67. QUIN is a potent excitotoxin with pro‐inflammatory and immunoregulatory properties. In addition to being a direct NMDA receptor agonist, QUIN increases neuronal glutamate release and decreases glutamate uptake and recycling by astrocytes 68. KYNA has neuroprotective and anticonvulsive properties, although elevated levels may be associated with the development of psychotic symptoms and are observed in patients with schizophrenia 69, 70.
Evidence of kynurenine pathway alterations in suicidality
In 2011, Sublette et al. 71 reported that the blood level of kynurenine, the first metabolite produced along the kynurenine pathway, is significantly elevated in suicide attempters with depression compared to non‐suicidal patients with depression, t(58) = 2.1, P = 0.04. This suggests that the activation of the kynurenine pathway in the periphery may serve as a marker, potentially distinguishing suicidal from non‐suicidal depressed patients. Kynurenine can freely pass through the BBB, and while in the brain, it can initiate inflammation and lead to further production of the secondary kynurenine metabolites 58. It has not been firmly established whether peripheral QUIN, KYNA and several other metabolites cross the BBB, and therefore, central measures of these markers in psychiatric patients are currently highly relevant to increase our understanding of their contribution to psychiatric illness. In a study where we measured KYNA and QUIN in the CSF of suicide attempters, QUIN levels were found to be more than twice as high as those in healthy controls, while KYNA levels were unaltered 72. This gave rise to an increased QUIN/KYNA quotient, indicative of a potential net positive effect on NMDA receptor transmission in suicidality. Moreover, CSF QUIN correlated with CSF IL‐6 levels, suggesting that the kynurenine pathway and the generation of QUIN had been induced by an active inflammatory process 72. A further example suggesting a role for QUIN in suicidality was the finding of a positive association between high CSF QUIN levels and high suicidal intent (Spearman ρ = 0.3, P = 0.03). In a follow‐up study, we measured CSF levels of the metabolites repeatedly over the first years following a suicide attempt 73. We found that the QUIN levels were continuously elevated in the patients who had performed a suicide attempt, while the levels were highest in close proximity to the attempt. The magnitude of their depressive and suicidal symptoms fluctuated with increasing cytokine levels and decreasing KYNA levels. In line with this, decreased plasma KYNA levels in depressed patients have previously been observed 74, although recent studies indicate that patients with depression without suicidality may not have any significant changes in the peripheral kynurenine pathway 75.
Interestingly, this accumulating evidence suggests that subsets of patients, prone to suicidal behaviour, could be sensitive to inflammatory changes and may develop symptoms upon such challenges, possibly as a result of an enzymatic imbalance of the kynurenine pathway in the CNS. The increased levels of QUIN could also contribute to the cell loss and structural changes in cortical and subcortical regions that have been reported in patients with suicidal behaviour, due to the neurotoxic effects of the metabolite 76. Recent postmortem data from suicide completers support the data gathered in attempters, by showing increased counts of QUIN‐reactive microglia cells in the subgenual anterior cingulate cortex (sACC) and anterior midcingulate cortex (aMCC) of those with depression who completed suicide 77. The findings that an NMDA receptor agonist (QUIN) is increased and an NMDA receptor antagonist (KYNA) is found to be decreased in patients support a role for a glutamatergic mechanism in the generation of suicidality. Noteworthy, the findings of exceptionally high levels of the NMDA receptor agonist QUIN in the CNS of suicidal patients could provide a neurobiological rationale for the rapid remedial effects of ketamine, an NMDA receptor antagonist, on suicidal ideation 78, 79. It remains to be described how enzymes in the kynurenine pathway are regulated. It is currently not known whether specific cytokines activate some of the enzymes in the kynurenine pathway in preference over others, or why some metabolites would accumulate in favor of another. In this respect, it has been suggested that genetic variants could pay a role 80.
Suicidal ideation and behaviour in somatic conditions with increased inflammation
The studies described above shows that inflammation is present in some cohorts of suicidal patients and that inflammation also is specifically associated with clinically important symptoms of suicidal behaviour. In addition, studies in both animals and human subjects confirm the causal relation between cytokines and symptoms of hopelessness, aggression and hostility, intermediate phenotypes for suicidal behaviour 14, 15, 16. Therefore, it is possible that inflammation observed in patients with so‐called ‘primary psychiatric conditions’ is actually part of a pathogenic mechanism that contributes to suicidal symptoms. Many somatic conditions are associated with increased peripheral and central inflammation. If our hypothesis is true, then, suicidal ideation and behaviour should also be increased in some of these somatic conditions.
Suicide, asthma and allergies
Asthma and allergies consist of an array of innate and adaptive immune responses, locally as well as systemically in the peripheral blood 81. To our knowledge, it is currently not known if there are any CNS inflammatory changes in these conditions. This topic is of interest, as several epidemiological studies have shown a link between suicide, allergies and asthma. There is an increased risk for both suicidal ideation, completed suicides and suicide attempts in patients with asthma 82. A large epidemiological study from Taiwan investigated suicide rates in more than 160 000 high school students, with and without asthma, over 12 years 83. The suicide rate in students with asthma was more than double that of the control group, with no difference in the number of natural deaths. In another epidemiological study from the Unites States (US), both suicidal ideation and suicide attempts were found to be associated with a current diagnosis of asthma 84. The risk increase for suicidal ideation and attempts seems to be approximately two‐ to three‐fold, with numbers varying between different studies.
A spring peak of suicides is observed each year around the world, but there is no current explanation for this phenomenon 85. Hypothetically, the increased amount of seasonal aeroallergens known to peak in spring, such as airborne pollen, could lead to increased upper airway inflammation and an increased risk of suicidal behaviour, in particular in sensitized individuals. A study from the United States over 4 years did indeed report an increased rate of suicides during the peaks in tree pollen in females 86. While a subsequent study in the United States failed to replicate the original finding 87, this was later replicated by a large population study in Denmark 88. It is important to note that the seasonal variation may be related to several factors, such as the exposure to visible and UV light, and seasonal variations of vitamin D levels, as discussed below. In addition, intranasal corticosteroids, first‐line treatment for allergic rhinitis, are known to reduce cytokine production in the nasal airways and have been pharmaco‐ecologically shown to be negatively associated with suicide rates. 89.
Vitamin D, inflammation and suicidality
Vitamin D is the common term for a group of related substances, particularly cholecalciferol (vitamin D3) and ergocalciferol (vitamin D2). The effects of vitamin D on the immune system include a shift in the T helper (Th)‐balance toward a Th2 phenotype, which in simplified terms can be said to lead to a less pro‐inflammatory state. As there is an over‐representation of vitamin D deficiency in patients with psychiatric illness 90, the lack of vitamin D has been proposed to contribute to the underlying disease mechanisms 91. Two studies to date have addressed the association between vitamin D and suicidality 92, 93. Umhau et al. investigated the vitamin D levels in blood samples from around 1000 active duty US military service members, of which half completed suicide over the year following the blood sample. They found that low vitamin D status was common in active military members, and the lowest levels were associated with an increased risk for suicide 92. In the study by Grudet et al., it was found that as many as 90% of patients with a recent suicide attempt had suboptimal levels of vitamin D, and 60% had a clear clinical deficiency. As expected, vitamin D in the blood correlated inversely with the levels of pro‐inflammatory cytokines 93.
Autoimmunity and suicidality
Increased rates of suicidality are also observed in autoimmune disorders such as systemic lupus erythematosus (SLE), MS and celiac disease. Approximately 40% of patients with SLE and MS develop depression at some point during their illness 94, 95. The neurobiological changes in SLE frequently include antibodies against the NMDA receptor, as well as microglial activation and BBB dysfunction 96. The prevalence of suicidal ideation was as high as 34% in a sample of around 300 Chinese patients with SLE 97. In a cohort of over 12 000 hospitalized patients with MS, Fredrikson et al. 98 found an increased suicide risk (odds risk ratio = 2.3) when compared to the general population. A smaller scale study of around 100 patients with MS in Denmark confirmed the two‐fold increased risk of dying by suicide 99. A large epidemiological study on a total of over 29 000 individuals with celiac disease in Sweden established that the patients with inflammatory disease also have a two‐fold increased risk for suicide 100.
Traumatic brain injury and suicidality
Traumatic brain injury (TBI) is a well‐known cause of neuroinflammation and glial activation 101. The effects on the brain parenchyma can be long lasting and has been proposed to underlie the increased suicidal behaviour observed in veterans as well as to constitute a risk factor in sports associated with frequent head trauma 102. Interestingly, in a recent large epidemiological study, the death records were compared between around 200 000 individuals who had been hospitalized due to TBI in Sweden over a 40‐year period and over 2 million controls, never hospitalized for TBI, as well as 150 000 unaffected siblings of the TBI victims 103. It was found that the TBI victims were more than 3 times as likely than the general population and unaffected siblings to die from suicide. Juengst et al. 104 measured serum and CSF levels of TNF‐α in patients with moderate and severe TBI as well as in controls. They found that the TBI patients had significantly higher TNF‐α levels than healthy controls and that the levels were associated both with disinhibition and suicidal ideation up to 12 months after the injury. Among 559 patients with mild‐to‐severe TBI, 25% reported suicidal ideation at one or more time points over the first year after the injury 105.
Infections and suicidality
Infectious agents in the CNS are likely to greatly increase the CSF levels of cytokines and kynurenine metabolites 106. Therefore, such infections can give important insights into the role of neuroinflammation in the development of suicidal symptoms. It is known that neuroborreliosis and neurosyphilis, as well as late‐stage HIV and AIDS, all frequently lead to neuropsychiatric symptoms. However, the prevalence and incidence rates of suicidality in these conditions still remain to be established. Suicide rates in patients that suffered from bacterial and viral meningitis are also unknown, but would be of relevance as such patients may be at heightened risk and could benefit from increased surveillance. There are also neurotrophic pathogens of low virulence, known to reside relatively quietly within the CNS of immuno‐competent hosts after infection. Such pathogens include the parasite Toxoplasma gondii (T. gondii). Interestingly, accumulating research now shows that such chronic, low‐grade infections may exert effects on the host brain to a much larger extent than previously thought. Repeated studies now confirm that there is a significantly increased risk for suicidal behaviour in individuals that are positive for T. gondii infection 107, 108, 109, 110. About 30% of the world's population is infected with the parasite in developing, as well as industrial, parts of the world. The initial peripheral infection is associated with none or very limited flulike symptoms in immunocompetent hosts, where after the parasite enters the brain, to form intracellular cysts in neurons and glial cells. A chronic infection with T. gondii can lead to increased neuroinflammation and increased production of kynurenine metabolites within the brain, potentially at the localized sites of the parasitic cysts 111. Moreover, it is possible that the parasite and the surrounding inflammatory changes could show varying degrees of activity, depending on the immunocompetence of the host. Finally, it has been shown that the T. gondii parasite contains two genes encoding tyrosine hydroxylase, the enzyme responsible for producing l‐dopa 112. Changes in impulsivity and the regulation of fear might increase the risk for suicidal behaviour, perhaps particularly in combination with inflammatory changes in the CNS. We analyzed the antibody titers to T. gondii in a small study of recent suicide attempters and controls and found that seropositivity was associated with a greatly increased odds risk ratio for suicide attempt (adjusted odds risk ratio = 7.1; P = 0.01) 109 . In a large epidemiological study of 45 000 Danish mothers, seropositive subjects had an increased relative risk of 1.8 for violent suicide attempts and 2.1 for suicides compared to non‐infected mothers 110. These results are consistent with previously reported small samples of patients with mood disorders and younger patients with schizophrenia, both studies eliminating the potential confound of mental illness by including both healthy controls and also psychiatric controls as comparison 107, 108. Recently, T. gondii infection has been linked, independent of mental illness, with intermediate phenotypes of suicidal behaviour such as trait aggression (in women) and impulsivity (in younger men) 113.
Discussion
In summary, there is a growing body of evidence that inflammation, as manifested by increased levels of pro‐inflammatory cytokines and inflammatory metabolites, is present in patients with suicidal behaviour and ideation. The inflammatory changes can be detected in the periphery, CSF and brain parenchyma of affected patients. Inflammation activates the kynurenine pathway, with a down‐stream production of metabolites with effects on glutamate neurotransmission, which could be an important biological mechanism responsible for symptom generation. The rapid antisuicidal effect of the NMDA receptor antagonist, ketamine, may be due to its effect on the same biological pathway. In addition, cytokines induce site‐specific effects on behaviour and emotion in different brain areas. Our knowledge in this field is just beginning to evolve. In order to find the optimal treatment regimen for suicidal symptoms, it is of critical importance to identify both the upstream triggers of inflammation, the downstream neurobiological effectors, as well as moderators that convey vulnerability or resilience. Importantly, there are several anti‐inflammatory treatments that are clinically approved for other indications. The effects of these common anti‐inflammatory agents could be tested in patients with suicidal behaviour and ideation in randomized controlled trials (RCTs), after it has been concluded which one of them have the optimal effects in reducing CNS inflammation. Future clinical trials should also, for example, evaluate the effects of antiparasitic treatment on T. gondii infection in patients with suicidal behaviour. Other novel therapeutic strategies could include inhibition of the first enzyme of the kynurenine pathway, IDO‐1, or target microglial activation by means of drugs such as minocycline. As knowledge increases about the role of specific cytokines for symptom generation, specific cytokine blockers, potentially with access to the CNS, could also be developed and tested. Finally, it makes sense to screen patients prior to clinical trials to identify subgroups of patients with increased inflammation, or vulnerability to inflammation, in order to minimize heterogeneity of treatment response 114. Identification of such subgroups of patients with an inflammatory profile is expected to increase the precision of anti‐inflammatory treatments in reducing suicide risk, at the same time preventing unnecessary exposure to anti‐inflammatory treatments in those unlikely to benefit.
Declaration of interests
Eric D. Achtyes has received research funding to support work related to depression from AssurEx, Janssen, Novartis, Pine Rest Foundation, Priority Health, and the University of Chicago. He has also served as a consultant to Roche for work on schizophrenia.
Acknowledgements
Lena Brundin and Eric D. Achtyes were supported by the National Institute of Mental Health, Bethesda, MD, R01MH104622‐01, Michigan State University and Van Andel Research Institute. Elena Y. Bryleva was supported by Van Andel Research Institute. Sophie Erhardt was supported by Swedish Research Council Grants 2009‐7052, 2013‐2838 and an independent research grant from Astra Zeneca. Teodor T. Postolache was supported by an American Foundation for Suicide Prevention Distinguished Investigator Award and by Veterans Integrated Service Network 19, Rocky Mountain Mental Illness Research Education and Clinical Center (MIRECC), Denver, CO, USA, and the Veterans Integrated Service Network 5, MIRECC, Baltimore, MD, USA. Partial funding for Teodor T. Postolache was also provided by the Mid‐Atlantic Nutrition and Obesity Research Center (NORC) (P30DK072488) from the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, MD. The views, opinions and findings contained in this article belong to the authors and should not be construed as an official position of the NIH, American Foundation for Suicide Prevention, Department of Veterans Affairs or any other funding organization.
Brundin L, Erhardt S, Bryleva EY, Achtyes ED, Postolache TT. The role of inflammation in suicidal behaviour.
References
- 1. Mortality GBD, Causes OF, Death C. Global, regional, and national age‐sex specific all‐cause and cause‐specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;385:117–171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. World Health Organization . Preventing suicide: a global imperative. Geneva, 2014. [updated 2014; cited April 30, 2015]; Available from: http://apps.who.int/iris/bitstream/10665/131056/1/9789241564779_eng.pdf. [Google Scholar]
- 3. Varnik P. Suicide in the world. Int J Environ Res Public Health 2012;9:760–771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bertolote JM, Fleischmann A. Suicide and psychiatric diagnosis: a worldwide perspective. World Psychiatry 2002;1:181–185. [PMC free article] [PubMed] [Google Scholar]
- 5. da Cruz D, Pearson A, Saini P et al. Emergency department contact prior to suicide in mental health patients. Emerg Med J 2011;28:467–471. [DOI] [PubMed] [Google Scholar]
- 6. Wasserman D, Rihmer Z, Rujescu D et al. The European Psychiatric Association (EPA) guidance on suicide treatment and prevention. Eur Psychiatry 2012;27:129–141. [DOI] [PubMed] [Google Scholar]
- 7. Hammad TA, Laughren T, Racoosin J. Suicidality in pediatric patients treated with antidepressant drugs. Arch Gen Psychiatry 2006;63:332–339. [DOI] [PubMed] [Google Scholar]
- 8. Zarate C, Duman RS, Liu G, Sartori S, Quiroz J, Murck H. New paradigms for treatment‐resistant depression. Ann N Y Acad Sci 2013;1292:21–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Fond G, Loundou A, Rabu C et al. Ketamine administration in depressive disorders: a systematic review and meta‐analysis. Psychopharmacology 2014;231:3663–3676. [DOI] [PubMed] [Google Scholar]
- 10. Roy A, Sarchiopone M, Carli V. Gene–environment interaction and suicidal behavior. J Psychiatr Pract 2009;15:282–288. [DOI] [PubMed] [Google Scholar]
- 11. Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta‐analysis. Br J Psychiatry 1997;170:205–228. [DOI] [PubMed] [Google Scholar]
- 12. Osby U, Brandt L, Correia N, Ekbom A, Sparen P. Excess mortality in bipolar and unipolar disorder in Sweden. Arch Gen Psychiatry 2001;58:844–850. [DOI] [PubMed] [Google Scholar]
- 13. Hawton K, van Heeringen K. Suicide. Lancet 2009;373:1372–1381. [DOI] [PubMed] [Google Scholar]
- 14. Dumais A, Lesage AD, Alda M et al. Risk factors for suicide completion in major depression: a case–control study of impulsive and aggressive behaviors in men. Am J Psychiatry 2005;162:2116–2124. [DOI] [PubMed] [Google Scholar]
- 15. Perroud N, Baud P, Mouthon D, Courtet P, Malafosse A. Impulsivity, aggression and suicidal behavior in unipolar and bipolar disorders. J Affect Disord 2011;134:112–118. [DOI] [PubMed] [Google Scholar]
- 16. David Klonsky E, Kotov R, Bakst S, Rabinowitz J, Bromet EJ. Hopelessness as a predictor of attempted suicide among first admission patients with psychosis: a 10‐year cohort study. Suicide Life Threat Behav 2012;42:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. McGuffin P, Perroud N, Uher R et al. The genetics of affective disorder and suicide. Eur Psychiatry 2010;25:275–277. [DOI] [PubMed] [Google Scholar]
- 18. Bach H, Arango V. Neuroanatomy of serotonergic abnormalities in suicide, Chapter 2 In: Dwivedi Y, ed. The neurobiological basis of suicide. Boca Raton, FL: CRC Press, 2012. [PubMed] [Google Scholar]
- 19. Mann JJ. Neurobiology of suicidal behaviour. Nat Rev Neurosci 2003;4:819–828. [DOI] [PubMed] [Google Scholar]
- 20. Raison CL, Borisov AS, Broadwell SD et al. Depression during pegylated interferon‐alpha plus ribavirin therapy: prevalence and prediction. J Clin Psychiatry 2005;66:41–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Raison CL, Borisov AS, Majer M et al. Activation of central nervous system inflammatory pathways by interferon‐alpha: relationship to monoamines and depression. Biol Psychiatry 2009;65:296–303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Raison CL, Dantzer R, Kelley KW et al. CSF concentrations of brain tryptophan and kynurenines during immune stimulation with IFN‐alpha: relationship to CNS immune responses and depression. Mol Psychiatry 2010;15:393–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Dieperink E, Ho SB, Tetrick L, Thuras P, Dua K, Willenbring ML. Suicidal ideation during interferon‐alpha2b and ribavirin treatment of patients with chronic hepatitis C. Gen Hosp Psychiatry 2004;26:237–240. [DOI] [PubMed] [Google Scholar]
- 24. Janssen HL, Brouwer JT, van der Mast RC, Schalm SW. Suicide associated with alfa‐interferon therapy for chronic viral hepatitis. J Hepatol 1994;21:241–243. [DOI] [PubMed] [Google Scholar]
- 25. Fragoso YD, Frota ER, Lopes JS et al. Severe depression, suicide attempts, and ideation during the use of interferon beta by patients with multiple sclerosis. Clin Neuropharmacol 2010;33:312–316. [DOI] [PubMed] [Google Scholar]
- 26. Reichenberg A, Yirmiya R, Schuld A et al. Cytokine‐associated emotional and cognitive disturbances in humans. Arch Gen Psychiatry 2001;58:445–452. [DOI] [PubMed] [Google Scholar]
- 27. Nassberger L, Traskman‐Bendz L. Increased soluble interleukin‐2 receptor concentrations in suicide attempters. Acta Psychiatr Scand 1993;88:48–52. [DOI] [PubMed] [Google Scholar]
- 28. Steiner J, Bielau H, Brisch R et al. Immunological aspects in the neurobiology of suicide: elevated microglial density in schizophrenia and depression is associated with suicide. J Psychiatr Res 2008;42:151–157. [DOI] [PubMed] [Google Scholar]
- 29. Tonelli LH, Stiller J, Rujescu D et al. Elevated cytokine expression in the orbitofrontal cortex of victims of suicide. Acta Psychiatr Scand 2008;117:198–206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Lindqvist D, Janelidze S, Hagell P et al. Interleukin‐6 is elevated in the cerebrospinal fluid of suicide attempters and related to symptom severity. Biol Psychiatry 2009;66:287–292. [DOI] [PubMed] [Google Scholar]
- 31. Pandey GN, Rizavi HS, Ren X et al. Proinflammatory cytokines in the prefrontal cortex of teenage suicide victims. J Psychiatr Res 2012;46:57–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Janelidze S, Mattei D, Westrin A, Traskman‐Bendz L, Brundin L. Cytokine levels in the blood may distinguish suicide attempters from depressed patients. Brain Behav Immun 2011;25:335–339. [DOI] [PubMed] [Google Scholar]
- 33. Kim YK, Lee SW, Kim SH et al. Differences in cytokines between non‐suicidal patients and suicidal patients in major depression. Prog Neuropsychopharmacol Biol Psychiatry 2008;32:356–361. [DOI] [PubMed] [Google Scholar]
- 34. Falcone T, Fazio V, Lee C et al. Serum S100B: a potential biomarker for suicidality in adolescents? PLoS One 2010;5:e11089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. O'Donovan A, Rush G, Hoatam G et al. Suicidal ideation is associated with elevated inflammation in patients with major depressive disorder. Depress Anxiety 2013;30:307–314. [DOI] [PubMed] [Google Scholar]
- 36. Black C, Miller BJ. Meta‐analysis of cytokines and chemokines in suicidality: distinguishing suicidal versus nonsuicidal patients. Biol Psychiatry 2015;78:28–37. [DOI] [PubMed] [Google Scholar]
- 37. Serafini G, Pompili M, Elena Seretti M et al. The role of inflammatory cytokines in suicidal behavior: a systematic review. Eur Neuropsychopharmacol 2013;23:1672–1686. [DOI] [PubMed] [Google Scholar]
- 38. Le‐Niculescu H, Levey DF, Ayalew M et al. Discovery and validation of blood biomarkers for suicidality. Mol Psychiatry 2013;18:1249–1264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Dantzer R, O'Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci 2008;9:46–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry 2009;65:732–741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Borsini A, Zunszain PA, Thuret S, Pariante CM. The role of inflammatory cytokines as key modulators of neurogenesis. Trends Neurosci 2015;38:145–157. [DOI] [PubMed] [Google Scholar]
- 42. Schobitz B, de Kloet ER, Sutanto W, Holsboer F. Cellular localization of interleukin 6 mRNA and interleukin 6 receptor mRNA in rat brain. Eur J Neuorsci 1993;5:1426–1435. [DOI] [PubMed] [Google Scholar]
- 43. Schele E, Fekete C, Egri P et al. Interleukin‐6 receptor alpha is co‐localised with melanin‐concentrating hormone in human and mouse hypothalamus. J Neuroendocrinol 2012;24:930–943. [DOI] [PubMed] [Google Scholar]
- 44. Ericsson A, Liu C, Hart RP, Sawchenko PE. Type 1 interleukin‐1 receptor in the rat brain: distribution, regulation, and relationship to sites of IL‐1‐induced cellular activation. J Comp Neurol 1995;361:681–698. [DOI] [PubMed] [Google Scholar]
- 45. Kawasaki Y, Zhang L, Cheng JK, Ji RR. Cytokine mechanisms of central sensitization: distinct and overlapping role of interleukin‐1beta, interleukin‐6, and tumor necrosis factor‐alpha in regulating synaptic and neuronal activity in the superficial spinal cord. J Neurosci 2008;28:5189–5194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Garcia‐Oscos F, Salgado H, Hall S et al. The stress‐induced cytokine interleukin‐6 decreases the inhibition/excitation ratio in the rat temporal cortex via trans‐signaling. Biol Psychiatry 2012;71:574–582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Dunn AJ. Effects of cytokines and infections on brain neurochemistry. Clin Neurosci Res 2006;6:52–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Malkesman O, Pine DS, Tragon T et al. Animal models of suicide‐trait‐related behaviors. Trends Pharmacol Sci 2009;30:165–173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Hassanain M, Zalcman S, Bhatt S, Siegel A. Interleukin‐1 beta in the hypothalamus potentiates feline defensive rage: role of serotonin‐2 receptors. Neuroscience 2003;120:227–233. [DOI] [PubMed] [Google Scholar]
- 50. Bhatt S, Bhatt R, Zalcman SS, Siegel A. Role of IL‐1 beta and 5‐HT2 receptors in midbrain periaqueductal gray (PAG) in potentiating defensive rage behavior in cat. Brain Behav Immun 2008;22:224–233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Bhatt S, Siegel A. Potentiating role of interleukin 2 (IL‐2) receptors in the midbrain periaqueductal gray (PAG) upon defensive rage behavior in the cat: role of neurokinin NK(1) receptors. Behav Brain Res 2006;167:251–260. [DOI] [PubMed] [Google Scholar]
- 52. Patel A, Siegel A, Zalcman SS. Lack of aggression and anxiolytic‐like behavior in TNF receptor (TNF‐R1 and TNF‐R2) deficient mice. Brain Behav Immun 2010;24:1276–1280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Carroll JE, Low CA, Prather AA et al. Negative affective responses to a speech task predict changes in interleukin (IL)‐6. Brain Behav Immun 2011;25:232–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Westling S, Ahren B, Traskman‐Bendz L, Brundin L. Increased IL‐1beta reactivity upon a glucose challenge in patients with deliberate self‐harm. Acta Psychiatr Scand 2011;124:301–306. [DOI] [PubMed] [Google Scholar]
- 55. Bezemer G, van Gool AR, Fekkes D et al. Psychiatric side effects and fluctuations in serotonergic parameters in the treatment of chronic hepatitis C infection. Neuropsychobiology 2012;65:126–132. [DOI] [PubMed] [Google Scholar]
- 56. Lotrich FE, Ferrell RE, Rabinovitz M, Pollock BG. Labile anger during interferon alfa treatment is associated with a polymorphism in tumor necrosis factor alpha. Clin Neuropharmacol 2010;33:191–197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Miller AH. Conceptual confluence: the kynurenine pathway as a common target for ketamine and the convergence of the inflammation and glutamate hypotheses of depression. Neuropsychopharmacology 2013;38:1607–1608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Schwarcz R, Bruno JP, Muchowski PJ, Wu HQ. Kynurenines in the mammalian brain: when physiology meets pathology. Nat Rev Neurosci 2012;13:465–477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Schwieler L, Larsson MK, Skogh E et al. Increased levels of IL‐6 in the cerebrospinal fluid of patients with chronic schizophrenia–significance for activation of the kynurenine pathway. J Psychiatry Neurosci 2015;40:126–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Urata Y, Koga K, Hirota Y et al. IL‐1beta increases expression of tryptophan 2,3‐dioxygenase and stimulates tryptophan catabolism in endometrioma stromal cells. Am J Reprod Immunol 2014;72:496–503. [DOI] [PubMed] [Google Scholar]
- 61. Maes M, Leonard BE, Myint AM, Kubera M, Verkerk R. The new ‘5‐HT’ hypothesis of depression: cell‐mediated immune activation induces indoleamine 2,3‐dioxygenase, which leads to lower plasma tryptophan and an increased synthesis of detrimental tryptophan catabolites (TRYCATs), both of which contribute to the onset of depression. Prog Neuropsychopharmacol Biol Psychiatry 2011;35:702–721. [DOI] [PubMed] [Google Scholar]
- 62. Asberg M, Traskman L, Thoren P. 5‐HIAA in the cerebrospinal fluid. A biochemical suicide predictor? Arch Gen Psychiatry 1976;33:1193–1197. [DOI] [PubMed] [Google Scholar]
- 63. Leklem JE. Quantitative aspects of tryptophan metabolism in humans and other species: a review. Am J Clin Nutr 1971;24:659–672. [DOI] [PubMed] [Google Scholar]
- 64. Guillemin GJ, Kerr SJ, Smythe GA et al. Kynurenine pathway metabolism in human astrocytes: a paradox for neuronal protection. J Neurochem 2001;78:842–853. [DOI] [PubMed] [Google Scholar]
- 65. Stone TW. Neuropharmacology of quinolinic and kynurenic acids. Pharmacol Rev 1993;45:309–379. [PubMed] [Google Scholar]
- 66. de Carvalho LP, Bochet P, Rossier J. The endogenous agonist quinolinic acid and the non endogenous homoquinolinic acid discriminate between NMDAR2 receptor subunits. Neurochem Int 1996;28:445–452. [DOI] [PubMed] [Google Scholar]
- 67. Hilmas C, Pereira EF, Alkondon M, Rassoulpour A, Schwarcz R, Albuquerque EX. The brain metabolite kynurenic acid inhibits alpha7 nicotinic receptor activity and increases non‐alpha7 nicotinic receptor expression: physiopathological implications. J Neurosci 2001;21:7463–7473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Guillemin GJ. Quinolinic acid, the inescapable neurotoxin. FEBS J 2012;279:1356–1365. [DOI] [PubMed] [Google Scholar]
- 69. Erhardt S, Olsson SK, Engberg G. Pharmacological manipulation of kynurenic acid: potential in the treatment of psychiatric disorders. CNS Drugs 2009;23:91–101. [DOI] [PubMed] [Google Scholar]
- 70. Linderholm KR, Skogh E, Olsson SK et al. Increased levels of kynurenine and kynurenic acid in the CSF of patients with schizophrenia. Schizophr Bull 2012;38:426–432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Sublette ME, Galfalvy HC, Fuchs D et al. Plasma kynurenine levels are elevated in suicide attempters with major depressive disorder. Brain Behav Immun 2011;25:1272–1278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Erhardt S, Lim CK, Linderholm KR et al. Connecting inflammation with glutamate agonism in suicidality. Neuropsychopharmacology 2013;38:743–752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Bay‐Richter C, Linderholm KR, Lim CK et al. A role for inflammatory metabolites as modulators of the glutamate N‐methyl‐D‐aspartate receptor in depression and suicidality. Brain Behav Immun 2015;43:110–117. [DOI] [PubMed] [Google Scholar]
- 74. Myint AM, Kim YK, Verkerk R, Scharpe S, Steinbusch H, Leonard B. Kynurenine pathway in major depression: evidence of impaired neuroprotection. J Affect Disord 2007;98:143–151. [DOI] [PubMed] [Google Scholar]
- 75. Dahl J, Andreassen OA, Verkerk R et al. Ongoing episode of major depressive disorder is not associated with elevated plasma levels of kynurenine pathway markers. Psychoneuroendocrinology 2015;56:12–22. [DOI] [PubMed] [Google Scholar]
- 76. van Heeringen K, Bijttebier S, Desmyter S, Vervaet M, Baeken C. Is there a neuroanatomical basis of the vulnerability to suicidal behavior? A coordinate‐based meta‐analysis of structural and functional MRI studies. Front Hum Neurosci 2014;8:824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Steiner J, Walter M, Gos T et al. Severe depression is associated with increased microglial quinolinic acid in subregions of the anterior cingulate gyrus: evidence for an immune‐modulated glutamatergic neurotransmission? J Neuroinflammation 2011;8:94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Price RB, Nock MK, Charney DS, Mathew SJ. Effects of intravenous ketamine on explicit and implicit measures of suicidality in treatment‐resistant depression. Biol Psychiatry 2009;66:522–526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Diazgranados N, Ibrahim LA, Brutsche NE et al. Rapid resolution of suicidal ideation after a single infusion of an N‐methyl‐D‐aspartate antagonist in patients with treatment‐resistant major depressive disorder. J Clin Psychiatry 2010;71:1605–1611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Claes S, Myint AM, Domschke K et al. The kynurenine pathway in major depression: haplotype analysis of three related functional candidate genes. Psychiatry Res 2011;188:355–360. [DOI] [PubMed] [Google Scholar]
- 81. Holt PG, Sly PD. Viral infections and atopy in asthma pathogenesis: new rationales for asthma prevention and treatment. Nat Med 2012;18:726–735. [DOI] [PubMed] [Google Scholar]
- 82. Goodwin RD. Asthma and suicide: current knowledge and future directions. Curr Psychiatry Rep 2012;14:30–35. [DOI] [PubMed] [Google Scholar]
- 83. Kuo CJ, Chen VC, Lee WC et al. Asthma and suicide mortality in young people: a 12‐year follow‐up study. Am J Psychiatry 2010;167:1092–1099. [DOI] [PubMed] [Google Scholar]
- 84. Goodwin RD, Demmer RT, Galea S, Lemeshow AR, Ortega AN, Beautrais A. Asthma and suicide behaviors: results from the Third National Health and Nutrition Examination Survey (NHANES III). J Psychiatr Res 2012;46:1002–1007. [DOI] [PubMed] [Google Scholar]
- 85. Christodoulou C, Douzenis A, Papadopoulos FC et al. Suicide and seasonality. Acta Psychiatr Scand 2012;125:127–146. [DOI] [PubMed] [Google Scholar]
- 86. Postolache TT, Stiller JW, Herrell R et al. Tree pollen peaks are associated with increased nonviolent suicide in women. Mol Psychiatry 2005;10:232–235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Woo JM, Gibbons RD, Rogers CA et al. Pollen counts and suicide rates. Association not replicated. Acta Psychiatr Scand 2012;125:168–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Qin P, Waltoft BL, Mortensen PB, Postolache TT. Suicide risk in relation to air pollen counts: a study based on data from Danish registers. BMJ Open 2013;3:e002462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Woo JM, Gibbons RD, Qin P et al. Suicide and prescription rates of intranasal corticosteroids and nonsedating antihistamines for allergic rhinitis: an ecological study. J Clin Psychiatry 2011;72:1423–1428. [DOI] [PubMed] [Google Scholar]
- 90. McCue RE, Charles RA, Orendain GC, Joseph MD, Abanishe JO. Vitamin D deficiency among psychiatric inpatients. Prim Care Companion CNS Disord 2012;14:pcc.11m01230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Kjaergaard M, Joakimsen R, Jorde R. Low serum 25‐hydroxyvitamin D levels are associated with depression in an adult Norwegian population. Psychiatry Res 2011;190:221–225. [DOI] [PubMed] [Google Scholar]
- 92. Umhau JC, George DT, Heaney RP et al. Low vitamin D status and suicide: a case–control study of active duty military service members. PLoS One 2013;8:e51543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Grudet C, Malm J, Westrin A, Brundin L. Suicidal patients are deficient in vitamin D, associated with a pro‐inflammatory status in the blood. Psychoneuroendocrinology 2014;50:210–219. [DOI] [PubMed] [Google Scholar]
- 94. Meszaros ZS, Perl A, Faraone SV. Psychiatric symptoms in systemic lupus erythematosus: a systematic review. J Clin Psychiatry 2012;73:993–1001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95. Chwastiak L, Ehde DM, Gibbons LE, Sullivan M, Bowen JD, Kraft GH. Depressive symptoms and severity of illness in multiple sclerosis: epidemiologic study of a large community sample. Am J Psychiatry 2002;159:1862–1868. [DOI] [PubMed] [Google Scholar]
- 96. Lauvsnes MB, Omdal R. Systemic lupus erythematosus, the brain, and anti‐NR2 antibodies. J Neurol 2012;259:622–629. [DOI] [PubMed] [Google Scholar]
- 97. Xie LF, Chen PL, Pan HF et al. Prevalence and correlates of suicidal ideation in SLE inpatients: Chinese experience. Rheumatol Int 2012;32:2707–2714. [DOI] [PubMed] [Google Scholar]
- 98. Fredrikson S, Cheng Q, Jiang GX, Wasserman D. Elevated suicide risk among patients with multiple sclerosis in Sweden. Neuroepidemiology 2003;22:146–152. [DOI] [PubMed] [Google Scholar]
- 99. Bronnum‐Hansen H, Stenager E, Nylev Stenager E, Koch‐Henriksen N. Suicide among Danes with multiple sclerosis. J Neurol Neurosurg Psychiatry 2005;76:1457–1459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Ludvigsson JF, Sellgren C, Runeson B, Langstrom N, Lichtenstein P. Increased suicide risk in coeliac disease–a Swedish nationwide cohort study. Dig Liver Dis 2011;43:616–622. [DOI] [PubMed] [Google Scholar]
- 101. Kumar A, Loane DJ. Neuroinflammation after traumatic brain injury: opportunities for therapeutic intervention. Brain Behav Immun 2012;26:1191–1201. [DOI] [PubMed] [Google Scholar]
- 102. Coughlin JM, Wang Y, Munro CA et al. Neuroinflammation and brain atrophy in former NFL players: an in vivo multimodal imaging pilot study. Neurobiol Dis 2015;74:58–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103. Fazel S, Wolf A, Pillas D, Lichtenstein P, Langstrom N. Suicide, fatal injuries, and other causes of premature mortality in patients with traumatic brain injury: a 41‐year Swedish population study. JAMA Psychiatry 2014;71:326–333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104. Juengst SB, Kumar RG, Arenth PM, Wagner AK. Exploratory associations with Tumor Necrosis Factor‐alpha, disinhibition and suicidal endorsement after traumatic brain injury. Brain Behav Immun 2014;41:134–143. [DOI] [PubMed] [Google Scholar]
- 105. Mackelprang JL, Bombardier CH, Fann JR, Temkin NR, Barber JK, Dikmen SS. Rates and predictors of suicidal ideation during the first year after traumatic brain injury. Am J Public Health 2014;104:e100–e107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106. Heyes MP, Saito K, Crowley JS et al. Quinolinic acid and kynurenine pathway metabolism in inflammatory and non‐inflammatory neurological disease. Brain 1992;115(Pt 5):1249–1273. [DOI] [PubMed] [Google Scholar]
- 107. Arling TA, Yolken RH, Lapidus M et al. Toxoplasma gondii antibody titers and history of suicide attempts in patients with recurrent mood disorders. J Nerv Ment Dis 2009;197:905–908. [DOI] [PubMed] [Google Scholar]
- 108. Okusaga O, Langenberg P, Sleemi A et al. Toxoplasma gondii antibody titers and history of suicide attempts in patients with schizophrenia. Schizophr Res 2011;133:150–155. [DOI] [PubMed] [Google Scholar]
- 109. Zhang Y, Traskman‐Bendz L, Janelidze S et al. Toxoplasma gondii immunoglobulin G antibodies and nonfatal suicidal self‐directed violence. J Clin Psychiatry 2012;73:1069–1076. [DOI] [PubMed] [Google Scholar]
- 110. Pedersen MG, Mortensen PB, Norgaard‐Pedersen B, Postolache TT. Toxoplasma gondii infection and self‐directed violence in mothers. Arch Gen Psychiatry 2012;69:1123–1130. [DOI] [PubMed] [Google Scholar]
- 111. Notarangelo FM, Wilson EH, Horning KJ et al. Evaluation of kynurenine pathway metabolism in Toxoplasma gondii‐infected mice: implications for schizophrenia. Schizophr Res 2014;152:261–267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112. Gaskell EA, Smith JE, Pinney JW, Westhead DR, McConkey GA. A unique dual activity amino acid hydroxylase in Toxoplasma gondii . PLoS One 2009;4:e4801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Cook TB, Brenner LA, Cloninger CR et al. ‘Latent’ infection with Toxoplasma gondii: association with trait aggression and impulsivity in healthy adults. J Psychiatr Res 2015;60:87–94. [DOI] [PubMed] [Google Scholar]
- 114. Miller AH, Raison CL. Are anti‐inflammatory therapies viable treatments for psychiatric disorders?: Where the rubber meets the road. JAMA Psychiatry. 2015;72:527–528. [DOI] [PMC free article] [PubMed] [Google Scholar]