

Abstract
Rhabdomyolysis is a rare complication that emerges in a variety of infectious diseases, such as tsutsugamushi infection. In this study, we report a 71-year-old female patient with tsutsugamushi infection who exhibiting rhabdomyolysis and acute renal failure. On admission, an eschar, which is characteristic of tsutsugamushi infection, was found on her right flank area. Moreover, her tsutsugamushi antibody titer was 1:40960. The elevated values of serum creatinine phosphokinase (CPK), aldolase, creatinine and dark brown urine secondary to myoglobinuria are consistent with indications of rhabdomyolysis and acute renal failure due to tsutsugamushi infection. Her health improved without any residual effects after treatment with doxycyclin and hydration with normal saline.
Keywords: Tsutsugamushi infection, Rhabdomyolysis, Acute renal failure
INTRODUCTION
Rhabdomyolysis is a syndrome characterized by extended myolysis, elevation of serum creatinine phosphokinase, myoglobinuria, and the frequent occurrence of renal dysfunction1). The spectrum of causes is quite broad and includes disorders of traumatic, metabolic, infectious, toxic, and enzymatic origin2). In Korea, while tsutsugamushi infection is a common disease, the association of rhabdomyolysis and acute renal failure with this disease is very rare3,4). Here, we describe a case of rhabdomyolysis and acute renal failure associated with tsutsugamushi infection.
CASE REPORT
A 71-year-old female farmer, with a past history of diabetes mellitus, showed symptoms of diffuse myalgia, severe muscle weakness and fever for 4 days. She was dehydrated, and general myalgias and weakness were so severe that she was unable to walk. Physical examination revealed the following values: 38.5°C body temperature, 80/50 mmHg blood pressure, 100/min pulse rate, 20/min respiratory rate. In particular, an eschar, which is characteristic of tsutsugamushi disease, was found on her right flank area. Her Tsutsugamushi antibody titer, which was measured by serologic indirect fluoroimmunoassay, was 1:40960. Significant laboratory findings included serum creatine phophokinase (CPK) 3250 U/L (normal less than 200 U/L), serum aldolase 22.4 IU/mL (normal less than 8 IU/mL), blood urea nitrogen 95 mg/dL (normal less than 22 mg/dL), creatinine 4.6 mg/dL (normal less than 1.4 mg/dL), potassium 5.1 mg/dL, sodium 129 mg/dL, uric acid 12.4 mg/dL (normal less than 7 mg/dL), albumin 2.1 g/dL, aspartate transaminase 173 U/L, and alanine transaminase 89.5 U/L. The patient’s urine was red, and analysis revealed a large amount of blood (4+, 0–1 red blood cells/high power field, 5–9 white blood cells/high power field). Urine myoglobin was 23.5 ng/mL (normal less than 7 ng/mL). White blood cell count was 6.4×109/L, hemoglobin 14.9 g/dL, and platelet count 92×109/L. Chest X-ray, electrocardiogram, and abdominal film were normal. She was diagnosed with rhabdomyolysis and acute renal failure associated with tsutsugamushi infection and was treated with doxycycline and fluid resuscitation with normal saline. Five days into treatment, creatinine and other laboratory findings normalized (Figure 1) and other clinical symptoms and signs improved greatly, including fever, myalgia, weakness and hypotension. She was subsequently discharged after 12 days.
Figure 1.
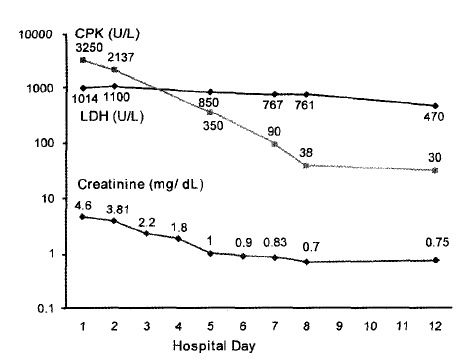
Clinical course of the patient.
DISCUSSION
Tsutsugamushi disease is an acute, rashed febrile disease with widely varying prognoses that ranges from unsymptomatic infection to death3,5). Early diagnosis and treatment can lead to speedy recovery. Otherwise, many complications may develop, including meningitis, myocarditis, acute renal failure, interstitial pneumonia and disseminated intravascular coagulopathy4–6). Rhabdomyolysis has been reported in association with a variety of infections, including coxsackie virus, leptospirosis, rocky mountain spotted fever, influenza and salmonella2,7–10). However, rhabdomyolysis with acute renal failure due to tsutsugamushi infection is a rarely reported complication4). The classic symptoms of rhabdomyolysis consists of myalgias, muscle tenderness, weakness, elevated serum creatinine phosphokinase (CPK), and dark brown urine secondary to myoglobinuria1). Complications of rhabdomyolysis include hyperkalemia, hyperuricemia, hypocalcemia, and hyperphosphatemia as a result of myonecrosis and myolysis. Acute renal failure is another potentially life threatening complication.
At the time of her hospitalization, an eschar indicative of tsutsugamushi disease was found on her right flank area. In addition, her tsutsugamushi antibody titer, measured by serologic indirect fluoroimmunoassay, was 1:40960. The elevated values of serum CPK and aldolase and dark brown urine secondary to myoglobinuria are consistent with the diagnosis of rhabdomyolysis. Moroever, there were complications of elevated creatinine, hyperuricemia and hyperkalemia.
The mechanisms during tsutsugamushi infection are poorly understood, but three mechanisms have been proposed for rhabdomyolysis in acute infection1). First, certain organisms (e.g, Clostridium speied) produce toxins that injur the muscle. Second, some pathogens (e.g, influenza virus, group A β-hemolytic streptococci, Staphylococcus aureus, and Gram-negative bacteria) directly invade the skeletal muscle. Finally, endotoxins (e.g, TNF-alpha and Interleukin-1), cause muscle proteolysis.
Careful attention to hydration and avoidance of potentially nephrotoxic agents is vital for patients with tsutsugamushi infection that show symptoms of sepsis and dehydration. With appropriate antibiotic treatment and comprehensive supportive care, the prognosis of rhabdomyolysis and renal failure in this patient population may be fairly good. We treated the patient with doxycycline and fluid resuscitation with normal saline. Subsequently, the patient recovered without any residual effects, and all clinical parameters returned to normal range after 12 days.
In conclusion, despite the rare occurence of rhabdomyolysis in tsutsugamushi infection, careful medical care is necessary for patients with muscle pain and weakness. Early diagnosis and treatement is critical.
Footnotes
This study was supported by research funds from Chosun University, 2002
REFERENCES
- 1.Betrosian A, Thireos E, Kofinas G, Balla M, Papanikolaou M, Georgiadis G. Bacterial sepsis-induced rhabdomyolysis. Intensive Care Med. 1999;25:469–474. doi: 10.1007/s001340050882. [DOI] [PubMed] [Google Scholar]
- 2.Gabow PA, Kaehny WD, Kelleher SP. The spectrum of rhabdomyolysis. Medicine (Baltimore) 1982;61:142–152. doi: 10.1097/00005792-198205000-00002. [DOI] [PubMed] [Google Scholar]
- 3.Chang WH. Current status of tsutsugamushi disease in Korea. J Korean Med Sci. 1995;10:227–238. doi: 10.3346/jkms.1995.10.4.227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Park YH, Kang EH, Kim JH, Park WD. A Case of Rhabdomyolysis and Acute Renal Failure Associated with Tsutsugamushi Disease. Korean J Nephrol. 2000;19:168–174. [Google Scholar]
- 5.Kim YO, Jeon HK, Cho SG, Yoon SA, Son HS, Oh SH, Chae HS, Kim KH, Chae JS, Lee CD, Lee BS. The role of hypoalbuminemia as a marker of the severity of disease in patients with tsutsugamushi disease. Korean J Med. 2000;59:516–521. [Google Scholar]
- 6.Kim IG, Lee SC, Kim JW, Seo KS, Park HB, Lee ST, Kim BC, Kim MK, Cho IH. Two Cases of Tsutsugamushi Meningitis. J Korean Neurol Assoc. 2000;18:642–644. [Google Scholar]
- 7.Byrd RP, Jr, Roy TM. Rhabdomyolysis of infectious and noninfectious causes. South Med J. 2002;95:1356–1357. doi: 10.1097/00007611-200211000-00027. [DOI] [PubMed] [Google Scholar]
- 8.Brncic N, Viskovic I, Sasso A, Kraus I, Zamolo G. Salmonella infection-associated acute rhabdomyolysis Some pathogenic considerations. Arch Med Res. 2002;33:313–315. doi: 10.1016/s0188-4409(01)00369-1. [DOI] [PubMed] [Google Scholar]
- 9.Sirmatel F, Balci I, Sirmatel O, Bayazit N, Hocaoglu S. A case of Salmonella paratyphi B septicaemia complicated by disseminated intravascular coagulation, severe hepatitis rhabdomyolysis and acute renal failure. Infect. 2001;43:19. doi: 10.1053/jinf.2001.0843. [DOI] [PubMed] [Google Scholar]
- 10.Rodriguez FL, Vernet BA, Poo Aguelles P, Fernandez Alvarez E, Garcia Calatayud J. Varicella induced rhabdomyolysis. An Esp Pediatr. 2001;55:374–377. [PubMed] [Google Scholar]