

Abstract
Both systemic lupus erythematosus and Sjogren’s syndrome are autoimmune diseases. Almost all organs can be involved but the gall bladder is an unusual site. We report a 39-year-old woman with systemic lupus erythematosus and Sjogren’s syndrome presenting with acute acalculous cholecystitis. It is a very rare complication and, in the literature review, surgical interventions are mostly applied for treatment. In our case, high dose corticosteroid was tried and clinical manifestations and radiologic findings were improved.
Keywords: acute acalculous cholecystitis, systemic lupus erythematosus, Sjogren’s syndrome, corticosteroid
INTRODUCTION
The systemic lupus erythematosus (SLE) is a disease of obscure etiology in which almost all organs can be involved, so its manifestations are various1,2). Sjogren’s syndrome (SS), also another autoimmune disease characterized by lymphocytic infiltration of the glandular organ and extraglandular manifestations, is seen alone or in association with other autoimmune rheumatic diseases, such as SLE3). In both diseases, involvement of gastrointestinal and hepatobiliary systems with sparing gall bladder is well documented. However, as in our case, acute acalculous cholecystitis (AAC) occurring in SLE patient with SS is very unusual, with only a few cases reported in the literature review so far (7 cases in SLE patients and 1 case as a necrotizing angiitis of gall bladder in SLE patient with SS)4–9). Although surgical intervention remains as mainstay treatment, non-surgical treatment with high dose corticosteroid successfully improved symptoms of acute acalculous cholecystitis-associated SLE patient with SS.
CASE
A 39-year-old woman was admitted due to abrupt abdominal pain in the right upper quadrant. Five years before the admission, she was diagnosed as SLE with SS manifested by oral ulcer, photosensitivity, malar rash with positive serologic finding of ANA (speckled, level 4, >1:2560), anti-dsDNA antibody and anti-Ro antibody (SS-A), dry eye, dry mouth, positive Schirmer’s test and biopsy findings of the minor salivary gland from the lower lip. Ever since, she has been visiting the clinic on a regular basis and has been on 5 mg of prednisone under the diagnosis of SLE with SS.
On admission, the temperature was 36.5°C, the pulse was 84/min, the respirations were 20/min and the blood pressure was 110/70 mmHg. She also complained of anorexia, nausea and multiple episodes of diarrhea. She had no history of fever, recent travel, recent exposure to ill persons or ingestion of contaminated food. She was dehydrated and looked pale. There was tenderness on the right upper quadrant of her abdomen, with positive Murphy’s sign. Laboratory tests, including blood cultures, were taken. They revealed hemoglobin 11 g/dL, WBC 7,000/mm3, neutrophils 84.2%, lymphocytes 6.4%, eosinophils 0.3%, monocytes 8.1%, ESR 57 mm/hr and CRP 7.43 mg/dL. Total protein 7.5 mg/dL, albumin 3.5 mg/dL, serum creatinine 3.9 mg/dL, BUN 34 mg/dL, ALT 13 U/L, AST 15 U/L, total bilirubin 0.4 mg/dL, alkaline phosphatase 63 U/L, amylase 66 U/L and lipase 0.4 U/L. Serologic profiles were speckled type ANA (level 4, >1:2560) and negative for anti-dsDNA antibody and anticardiolipin antibody. The C3 level was 90.6 mg/L and C4 levels 20.2 mg/L. Stool examination revealed neither parasites nor ova.
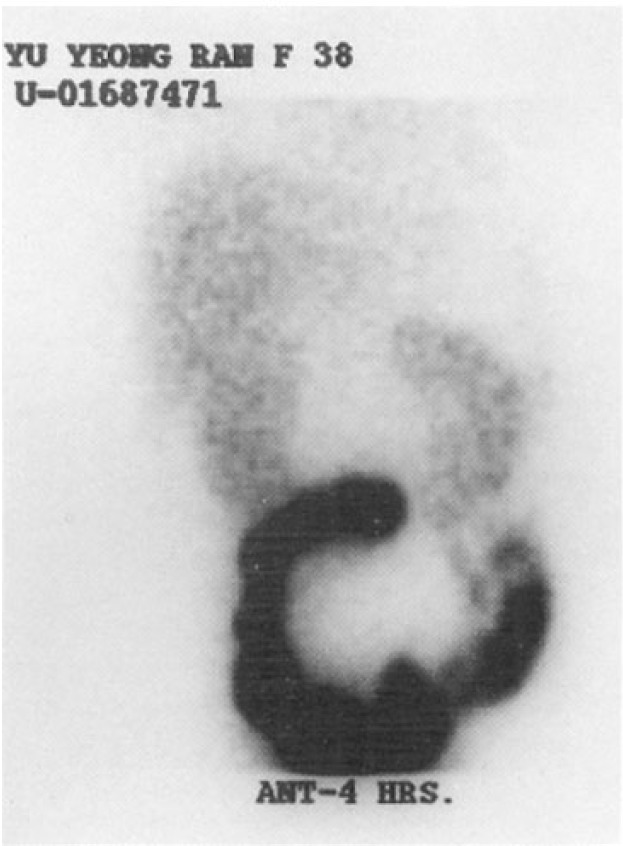
Abdominal CT (Figure 1-A) showed pericholecystic edema, increased thickness of the gall bladder wall without any evidence of stones and small amount of ascites without edematous bowel walls. Similar results were obtained by abdominal ultrasonography. Four hours after injection of the Tc-99m DISIDA, the gall bladder had not been visualized in scintigraphy (Figure 1-B). Gastric endoscopic findings were normal. All these findings strongly supported the diagnosis of lupus-associated acute acalculous cholecystitis, despite normal laboratory findings such as C3, C4 and anti dsDNA.
Figure 1-A.
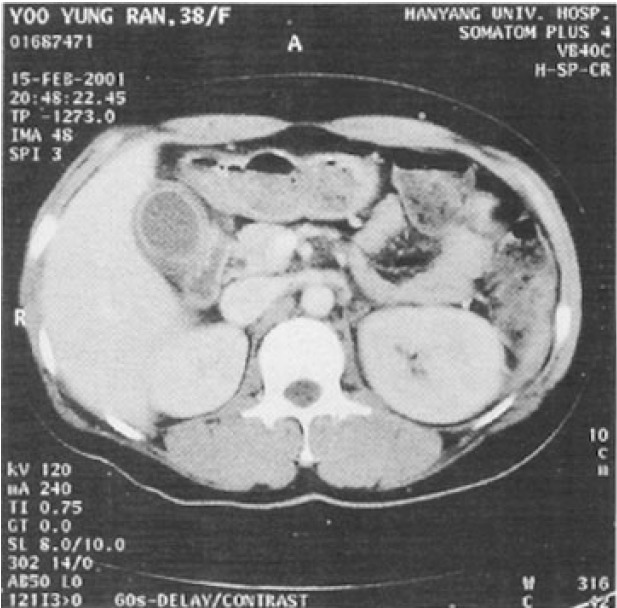
Figure 1-B.
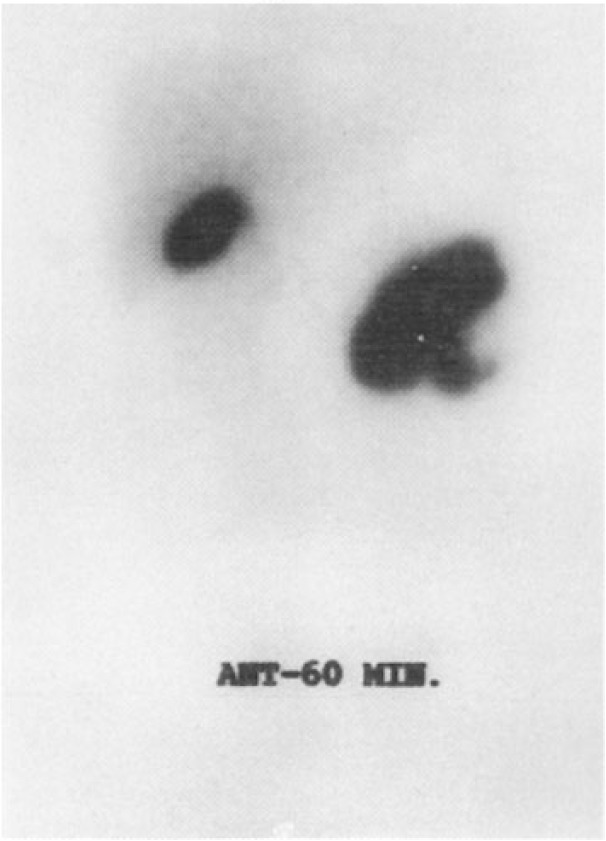
Initially, the patient was treated with third-generation cephalosporin, parenteral nutritional support and replacement of fluid and electrolyte. After the treatment course, serum BUN and creatinine levels returned to within normal range without improvement in her symptoms. As there was no evidence of infection with negative blood culture results, we applied a separate three cycles of high dose methyprednisolone. The symptoms markedly improved several days after the treatment and follow-up image studies were carried out. The CT scan (Figure 2-A) was normal. The hepatobiliary scan (Figure 2-B), compared to the previous study, revealed that gall bladder function improved. She was discharged with oral prednisone with steroid tapering planned at the out-patient clinic.
Figure 2-A.
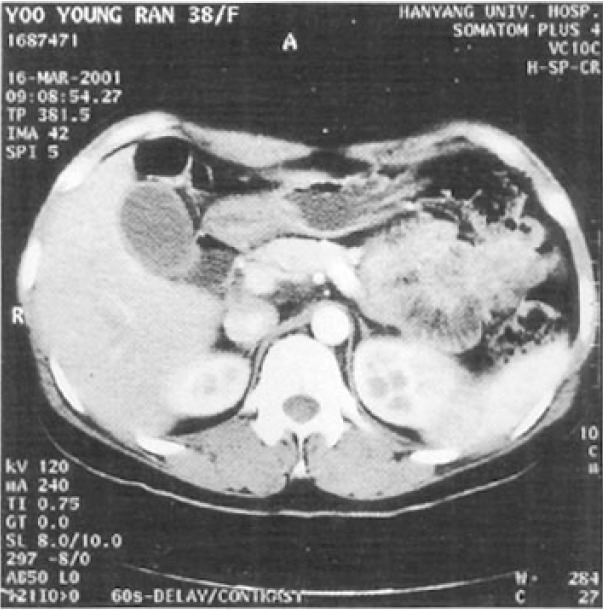
Figure 2-B.
She looked well and did not show any symptom related to AAC three months after discharge from the out-patient clinic.
DISCUSSION
The majority of SLE patients complain of gastrointestinal symptoms in the course of the disease10,11). Their etiologies are various; esophageal reflux and spasm, peptic ulceration with perforation, small and large intestinal abnormalities, such as edema, dysmotility, vasculitis and malabsorption, peritonitis from polyserositis, ascites, pancreatitis and hepatobiliary abnormality. In SS, the following gastrointestinal manifestations can be observed; difficulty in swallowing with xerostomia, reflux of gastric acid, atrophic gastritis, pancreatic insufficiency, coexistent of primary biliary sclerosis or sclerosing cholangitis3). According to previously reported cases, the gall bladder is rarely involved in SLE patients4–8) and only a single case was presented as necrotizing angiitis in a SLE patient with SS9). When the gall bladder is suspected as a source of abdominal pain in SLE, infection, gall stones or other causative factors must be evaluated and ruled out to confirm the final diagnosis of lupus involvement. The scintigraphy, ultrasonography and abdominal CT have all been proposed as the best way to evaluate the AAC12,13). Two most reliable diagnostic clues to cholecystitis are 1) increased gall bladder wall thickness and 2) the accumulated fluid around the gall bladder. Hepatobiliary scan showing invisible gall bladder particularly boasts in diagnosing acute cholecystitis. As the patient’s image studies are compatible with the above criteria of the AAC and as there were neither any evidence of infection nor related risk factors as causes of cholecystitis, we were able to conclude that the cholecystitis would be the results of vasculitis or serositis due to autoimmune diseases4–9).
In AAC, surgical approaches, such as cholecystectomy or percutaneous cholecystostomy, are regarded as the mainstay of treatment14,15). There has been only one case reported of medical treatment with high-dose corticosteroid therapy in a patient having AAC combined with high SLE disease activity8). The treatment had been successful in our case, possibly because of the following reasons: 1) the patient’s general good condition, 2) absence of significant laboratory data change during out-patient follow-up and admission period, 3) absence of definite risk factors related to AAC, 4) absence of serious complications, 5) exclusion of possibility of infection.
Conclusively, this current case suggests that noninvasive treatment of AAC may be used, regardless of the activity of SLE with wide tolerance, if above criteria are satisfied.
REFERENCES
- 1.McAlindon T. Update on the epidemiology of systemic lupus erythematosus: new spins on old ideas. Curr Opin Rheumatol. 2000;12:104–112. doi: 10.1097/00002281-200003000-00004. [DOI] [PubMed] [Google Scholar]
- 2.Ruiz-lrastorza G, Khamashta MA, Castellino G, Hughes GR. Systemic lupus erythematosus. Lancet. 2001;357:1027–1032. doi: 10.1016/S0140-6736(00)04239-2. [DOI] [PubMed] [Google Scholar]
- 3.Tzioufas AG, Youinou P, Moutsopoulos HM. Oxford textbook of rheumatology. New york: Oxford University Press; 1998. Sjogren’s syndrome; pp. 1301–1317. [Google Scholar]
- 4.Martinez D, Lowe R. Case report: systemic lupus erythematosus (SLE) serositis mimicking acute cholecystitis. Clin Radiol. 1991;44:434–435. doi: 10.1016/s0009-9260(05)80670-1. [DOI] [PubMed] [Google Scholar]
- 5.Raijman I, Schrager M. Hemorrhagic acalculous cholecystitis in systemic lupus erythematosus. Am J Gastroenterol. 1989;84:445–457. [PubMed] [Google Scholar]
- 6.Newbold KM, Allum WH, Downing R, Symmons DP, Oates GD. Vasculitis of the gall bladder in rheumatoid arthritis and systemic lupus erythematosus. Clin Rheumatol. 1987;6:287–289. doi: 10.1007/BF02201039. [DOI] [PubMed] [Google Scholar]
- 7.Swanepoel CR, Floyd A, Allison H, Learmonth GM, Cassidy MJ, Pascoe MD. Acute acalculous cholecystitis complicating systemic lupus erythematosus: case report and review. Br Med J(Clin Res Ed) 1983;286:251–252. doi: 10.1136/bmj.286.6361.251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kamimura T, Mimori A, Takeda A, Masuyama J, Yoshio T, Okazaki H, Kano S, Minota S. Acute acalculous cholecystitis in systemic lupus erythematosus: a case report and review of the literature. Lupus. 1998;7:361–363. doi: 10.1191/096120398678920154. [DOI] [PubMed] [Google Scholar]
- 9.Suwa A, Hama N, Kawai S, Ishiyama K, Tanabe M, Yamada T, Goto M, Nakajima A, Kashiwazaki S, Inada S. A case of Sjogren’s syndrome and systemic lupus erythematosus complicated with necrotizing angiitis on the gallbladder. Ryumachi. 1995;35:904–909. [PubMed] [Google Scholar]
- 10.Hallegua DS, Wallace DJ. Gastrointestinal manifestation of systemic lupus erythematosus. Curr Opin Rheumatol. 2000;12:379–385. doi: 10.1097/00002281-200009000-00005. [DOI] [PubMed] [Google Scholar]
- 11.Al-Hakeem MS, McMillen MA. Evaluation of abdominal pain in systemic lupus erythematosus. Am J Surg. 1998;176:291–294. doi: 10.1016/s0002-9610(98)00155-x. [DOI] [PubMed] [Google Scholar]
- 12.Robert KZ. Cholelithiasis and cholecystitis Textbook of gastrointestinal radiology. Philadelphia: W.B. Saunders company; 2000. pp. 1330–1345. [Google Scholar]
- 13.Barie PS, Fischer E, Eachempati SR. Acute acalculous cholecystitis. Curr Opin Crit Care. 1999;5:144. [Google Scholar]
- 14.Frassinelli P, Werner M, Reed JF, III, Scagliotti C. Laparoscopic cholecystectomy alleviates pain in patients with acalculous biliary disease. Surg Laparosc Endosc. 1998;8:30–34. [PubMed] [Google Scholar]
- 15.Yang HK, Hodgson WJ. Laparoscopic cholecystostomy for acute acalculous cholecystitis. Surg Endosc. 1996;10:673–675. doi: 10.1007/BF00188528. [DOI] [PubMed] [Google Scholar]