

Abstract
Agenesis of the right lobe of the liver is a rare congenital anomaly and only 29 cases have been reported in the literature. We encountered a patient with this anomaly diagnosed by ultrasonography, Computed tomography (CT), hepatobiliary scintigraphy, endoscopic retrograde cholangiopancreatography (ERCP) and celiac angiography.
The radiological findings, differential diagnosis, and clinical significance of this anomaly are reviewed.
Keywords: Agenesis, Right Lobe of the liver
INTRODUCTION
Congenital agenesis of the right lobe of the liver, although the configruation of hepatic lobes and segments varies considerably among individuals1), is very rare and only 29 cases have reported in the literature2). It has been known that this anomaly is caused by the developmental failure of the right portal vein or an error of mutual induction between the primitive diaphragm and the endodermal diverticulum representing the primitive liver3). Most of the patients with this anomaly are acompanied by the presence of retro-or suprahepatic gallbladder and other biliary diseases, including cholelithiases and gallbladder cancer4).
Herein, we present a new case and discuss the radiologic findings and clinical significance of this anomaly.
CASE REPORT
A 36-year-old male was admitted to Kosin University Hospital and because of severe colicky pain in the right upper quadrant of the abdomen radiating to the right shoulder. From 21 days prior to this admission, he had suffered from a dull aching pain in the right hypochondrium and treated with antacids and analgesics. On one day, before admission, the above symptom was more aggravated and severe colicky pain in the right hypochondrium eventually developed. On admission, he showed an acutely ill appearance and liver was palpable 2 cm below the right subcostal margin. Jaundice, anemia and malnutrition were not noted on inspection.
The laboratory findings showed a normal blood count and normal liver function values, except for a mild elevation of serum aminotransferase levels. Urinalysis and stool examination were also normal. Abdominal ultrasonography (Fig. 1A, 1B) and CT (Fig. 2A, 2B) visualized an enlarged caudate lobe as well as left lobe of the liver. The intrahepatic bile duct in the left lobe of the liver was slightly dilated and contained stones in it. The right lobe of the liver was absent and the gallbladder was displaced anterolaterally to the chest wall. ERCP (Fig. 3) revealed an absence of the right hepatic duct, supralateral displacement of gallbladder forming a blunt angle between the long axis of gallbladder and common bile duct. Liver scan using 99mTc-DISIDA (Fig. 4) showed an upward displacement of gallbladder with normal excretory function.
Fig. 1.
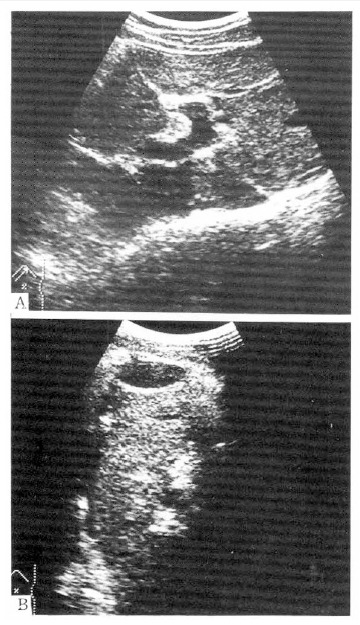
Ultrasonographic findings. (A) Right subcostal scanning shows that the left portal vein and it’s branches are well visualized but the right portal vein is absent. (B) Right intercostal scan reveals that the gallbladder is shifted anterolaterally to chest wall. Left medial segment contains stones.
Fig. 2.
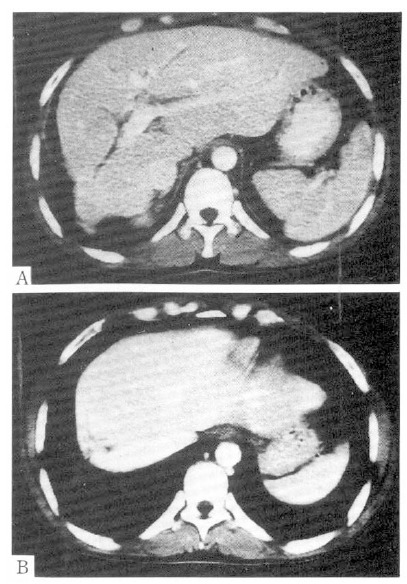
(A) Abdominal CT scan through liver shows no right lobe. Caudate lobe and lateral segment of the left lobe are markedly enlarged. Medial segment of the left lobe is normal in size. (B) Stones in focally dilatated intrahepatic bile duct are seen in medial segment of the left lobe.
Fig. 3.
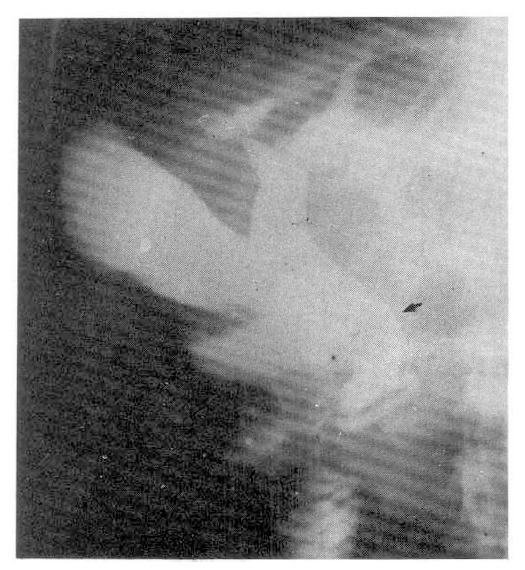
ERCP shows absence of hepatic duct leading to right lobe. Gallbladder moved upward to form blunt angle between gallbladder long axis and common bile duct. Intrahepatic duct stones are seen also.
Fig. 4.
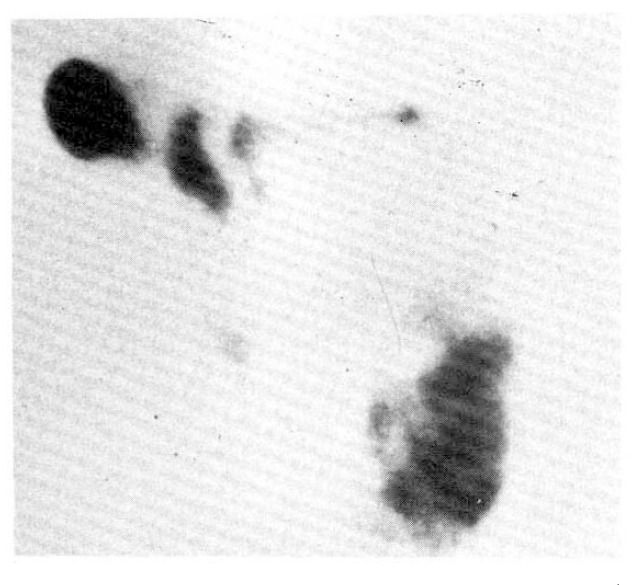
99mTc-DISIDA hepatobiliary scintigraphy at 1 hour visualizes superiorly displaced gallbladder, and no excretory abnormality.
Hepatic artery was divided into the middle and left hepatic artery from which the cystic artery is originating, but the right hepatic artery was not found on celiac angiography (Fig. 5A). Portovenography showed an absence of the right portal vein (Fig. 5B).
Fig. 5.
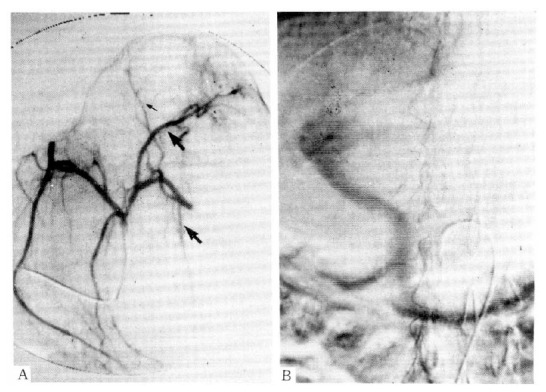
(A) Celiac angiography shows that hepatic artery divided into middle and left hepatic artery, cystic artery arises from left hepatic artery, but artery going to the right lobe is absent. (B) Portovenography shows absence of right portal vein.
DISCUSSION
Agenesis of the right hepatic lobe should be differentiated from a lobar atrophy of the right hepatic lobe, caused by cirrhosis, cholangiocarcinoma5), idiopathic portal hypertension and other biliary tract diseases6). Among these diseases, that produce a lobar atrophy of the right hepatic lobe, severe right lobe atrophy, secondary to liver cirrhosis and cholangiocarcinoma, often become an issue in the differential diagnosis of the right lobe agenesis7).
Terres et al analyzed the morpholopic changes on CT scan in cirrhotic liver and concluded that the morpholopy of cirrhotic liver was characterized by a decrease in the volume of the right hepatic lobe and medial segment of left hepatic lobe and an increase in volume of the caudate lobe and the lateral segment of the left hepatic lobe8).
The CT and ultrasonographic findings in our case revealed an enlarged caudate lobe and the lateral segment of the left hepatic lobe. These findings, in conjunction with normal size of medial segment of the left hepatic lobe, were quite similar to the morphologic changes in a cirrhotic liver, out there were no clinical features related to liver cirrhosis, cholangiocarcinoma and past history of hepatic surgery or trauma. Moreover, the absence of the right portal vein branch and artery, leading to the right hepatic lobe observed on angiography in our case, confirms the diagnosis. Radin et al4), based on the analysis of 24 cases of the right lobe agenesis, reported that this anomaly might be often associated with biliary tract disease, portal hypertension of the presinusoidal type, cholelithiasis and other congenital anomalies. In our case, intrahepatic duct stones were found in ERCP, but neither stone in gallbladder or cholangiocarcinoma in hilum were observed.
The absence of portal hypertension in our case might be explained by a full compensatory hypertrophy of the left lateral segment of the left lobe and the caudate lobe which keeps the capacity of the intrahepatic vascular bed3,9).
In the study by Radin et al4), 3 of the five patients with right lobe agenesis had agenesis of caudate lobe and 2 patients had mildly to moderately enlarged caudate lobe. However in our case, the caudate lobe was so markedly enlarged that it seemed to displace the gallbladder from retrohepatic position commonly seen in right lobe agenesis to anterolaterally.
Most of the patients with this anomaly remain clinically latent, but they often are complicated by a right upper abdominal pain probably derived from abnormal gallbladder position and contractility, cholelithiasis and choledocholithiasis.
It is, therefore, important to consider agenesis of the right hepatic lobe in the differential diagnosis when imaging studies revealing an abnormal hepatic morphologic characteristics associated with right upper abdominal pain.
REFERENCES
- 1.John RH, Ralph JA. Computed tomography of the whole body. 2en ed. 1988. p. 797. [Google Scholar]
- 2.Suneja SK, Teal JS. Scintigraphy in evaluation of the hypoplastic right hepatic lobe: a reare variant. J Natl Med Assoc. 1989;81:205. [PMC free article] [PubMed] [Google Scholar]
- 3.Betrand L, Janbon M. Une couse inedite d’hypertension portale: Lagenesie du lobe droit du foie. Rev Int Hepatol. 1962;12:897. [Google Scholar]
- 4.Radin DR, Colleti PM, Ralls PW, Boswell WD. Agenesis of the right lobe of the liver. Radiology. 1987;164:639. doi: 10.1148/radiology.164.3.3303118. [DOI] [PubMed] [Google Scholar]
- 5.Nakanuma Y, Nakamura Y, Hoso M, Ohta G. Atrophy and ductopenia of the right hepatic lobe in a patient with choledocholithiasis. Acta Pathol JPN. 1986;36:1719. doi: 10.1111/j.1440-1827.1986.tb02235.x. [DOI] [PubMed] [Google Scholar]
- 6.Fukai Y, Kikukawa M, Yoshida S. A case of Carvli’s disease with complete atrophy affecting hepatic Segment. J Jpn Soc Clin Surg. 1984;45:468. [Google Scholar]
- 7.Masayuki K, Takeyoshi I, Yoshihara Y, Hidetaka D. Agenesis of the right lobe of the liver: Case report. Gastriintesti Radiol. 1991;16:320. [Google Scholar]
- 8.Torres WE, Whimire LF, Gedgaudas-McClees K, Bernardino ME. Computed tomography of hepatic morphologic changes in cirrhosis of the liver. J Comput Assist Tomogr. 1986;10:173. doi: 10.1097/00004728-198601000-00009. [DOI] [PubMed] [Google Scholar]
- 9.Negre E, Pujol H, Thevenet A. L’hypertension portale des agenesis du lobe droit du fole. Presse Med. 1962;70:2501. [PubMed] [Google Scholar]