

Abstract
Introduction
Obesity in childhood impacts on many areas of the child’s current and future health, including their cardiovascular health. To date many attempts have been made to design interventions to tackle excess childhood weight but with limited success. We aimed to establish the components common to interventions in children that improve cardiovascular health parameters.
Methods
We searched the following databases: EMBASE 1974-week 3 November 2014, Ovid Medline 1946 Present, and PsychINFO 1967-Present for studies reporting interventions in healthy young people under the age of 18. Included interventions had to contain an education component and have been carried out in a community, school, or clinical setting. Papers had to report on at least one of the pre-specified CVD risk parameters and at least one non-biological outcome from knowledge, attitudes or behaviours.
Results
We retrieved 2451 papers, from which 12 studies (18 papers) of 3046 participants were included. From the selected papers we identified four component themes; Health Behaviours, Self-Concept, Practical and Cognitive Tools, and Intervention Characteristics. The subcomponents that made up these themes were fairly consistent across the studies analysed although the studies varied in their duration, settings and children with which they were carried out. Nine of the studies were able to bring about positive change in at least one biological and one non-biological aspect of child cardiovascular health.
Conclusion
The component themes identified here were common to intervention studies that had success in improving parameters of cardiovascular health. We suggest that the focus of childhood health interventions be moved from weight onto cardiovascular health parameters and that future interventions use the lessons learned by their predecessors to incorporate those components that are associated with successful interventions.
Introduction
Worldwide trends show that the numbers of children who are overweight or obese has increased dramatically over recent years: over a third of the child population in many countries are classed as such [1, 2]. While in the past excess weight was a condition primarily associated with more prosperous nations, obesity is now a global health problem and the second largest contributor to global disease burden [3, 4].
Obesity in the young could have wide reaching implications for health and for society. Obesity is associated with numerous physical and mental health comorbidities [1], as well as functional change to the cardiovascular system [5–8], and detrimental effects on society through lost productivity and financial burdens on health services [9, 10]. In addition, children with obesity face discrimination and stigma due to their weight status that also has negative consequences for both their physical and mental health. A review of the literature described the impact that weight bias can have on overweight children and adolescents, and detailed damaging effects on self-esteem, social interactions and even physical health through disordered eating and physical activity habits [11]. Additionally reports of increased blood pressure in those who experience discrimination because of their physical appearance were detailed, further highlighting the need to tackle this problem, but only through interventions that do not reinforce any existing weight stigma [11].
In response to this growing problem, the research community has designed and tested a multitude of behaviour change interventions to reduce weight and improve the health outcomes of children who are overweight and obese. The approaches used have been varied and have attempted to improve outcomes by targeting particular age groups [12, 13], specific health-related behaviours [14–16], and individual cultures [17]. Despite these attempts, shortcomings pervade this area of research. Systematic reviews of interventions have reported substantial limitations including: non comparable groups at baseline, lack of high quality trials, high amounts of heterogeneity leading to small and non-significant effects, effects which are not sustained at follow-up, and studies that are poorly reported [13–18].
The components of the studies summarised by the reviews above, such as dietary education, increasing moderate to vigorous physical activity, and parent education, are some of the most widely used and reported but form only a small part of the total variation of intervention components. These reviews were also all carried out with studies looking either exclusively or at least primarily at the effect of the intervention on weight-related outcomes such as weight loss, BMI reduction, or a reduction in the prevalence of being overweight. Our component analysis was performed as part of the wider WE ♥ Health study in which the aim was to move focus away from weight loss and on to cardiovascular health and in doing so highlight the importance of a healthy body over a slim body. By learning from the successes and failures of previous interventions, it was intended that future interventions could incorporate these lessons learned and build on the existing literature. As such, our aim was to identify the aspects of interventions that most frequently led to improvements in child cardiovascular health outcomes.
Methods
Ethics Statement
Ethical approval was not required as this is a synthesis of previously published research. The authors received no specific funding for this study and declare no conflicts of interest.
Component analysis
This component analysis was methodologically similar to a previous paper that analysed the components of self-monitoring interventions for CVD [19] and was carried out in six stages:
A literature search for relevant interventions.
Description of the included interventions.
Extraction of the intervention components into a pre-defined template.
Extraction of further information about the included interventions such as theoretical basis and the results achieved.
Authors contacted to provide missing information if any of the previous stages are not able to be completed from the papers.
Finally the extracted information was examined for components that were most frequently associated with success in interventions.
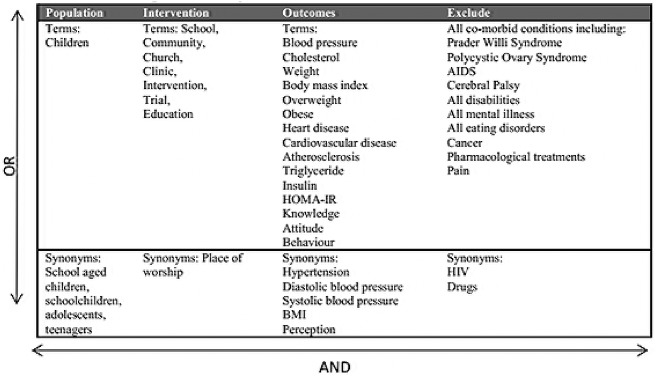
We searched the following databases: EMBASE 1974-week 3 November 2014, Ovid Medline 1946 Present, and PsychINFO 1967-Present. The search terms detailed in Fig 1 were truncated with wild card characters where necessary and searched in each of the databases. The PRISMA Checklist for this study can be seen in S1 PRISMA Checklist.
Fig 1. Search terms.
Studies included in the component analysis had to report on an intervention carried out in healthy young people under the age of 18 and use a control group so that the likelihood of any results occurring due to the effect of the intervention could be judged. We defined an improvement or healthy change in the variables of interest as a change in the intervention group compared to the control group, that could either be an increase or decrease depending on the variable, which reached a significance level of p≤0.05 as reported by the study. Included interventions had to contain an education component and had to have been carried out in a community, school, or clinical setting. Papers had to report on at least one of the CVD risk parameters searched as an outcome as well as the change in at least one non-biological outcome from knowledge, attitudes or behaviours. The inclusion criteria are summarised below:
Intervention studies.
Must have a control group.
Must be group interventions.
Interventions must be carried out in a school, community or clinical setting.
The intervention must have an education component.
Must measure at least one CVD risk parameters searched.
Must measure change in at least one of knowledge, attitudes or behaviours.
Studies were excluded if they contained a pharmacological element or if the paper did not report on changes in both the CVD risk parameters and the change in the knowledge, attitudes, or behaviours of the children. Papers were not excluded based on country of origin or date or language of publication. The exclusion criteria are summarised below:
Use of a pharmacological treatment.
Participants have a known co-morbid condition.
Failure to report sufficient outcome data.
Results
The database search retrieved 2451 papers, which were de-duplicated to leave 2044 papers. The titles of these papers were read and any that did not meet the inclusion criteria were excluded. The full text of the remaining 330 papers were read and excluded if any exclusion criteria were met. The most common reasons for exclusion from the component analysis were a lack of control group and a failure to report changes to CVD risk parameters as well as knowledge, attitudes or behaviours. Finally 12 studies (18 papers) which met all of the inclusion criteria and reported their data in sufficient detail were selected (Fig 2).
Fig 2. Selection process of papers included in the component analysis.

Table 1 shows the main characteristics of the included studies. The studies described interventions that lasted between six weeks and two years and where maintenance of the results was measured, these had follow-up periods of between six weeks and one year post intervention. A number of the studies were based on theoretical models such as the Theory of Planned Behaviour [20], Cognitive Behavioural Therapy [21–26], Social Cognitive Theory [22–27], and Cognitive Theory [28–30].
Table 1. Characteristics of included studies.
| Author | Study name | Country of origin | Number of participants | Age | Setting | Design | Duration | Outcomes measured | Achieved improvements in biological and non-biological outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Taylor et al. (2007) [33,34] | APPLE | New Zealand | 730 | 6–9 years | School | Non-randomised, controlled physical activity, nutrition and educational intervention | 2 years | Height, weight, waist circumference, pulse rate, blood pressure, BMI. Dietary intake questionnaire, physical activity through accelerometry, physical activity questionnaire, time spent television | Yes |
| Angelopoulos et al. (2009) [20] | CHILDREN | Greece | 646 | 9–10 years | School | Cluster randomised, controlled nutrition and physical activity intervention | 1 year | Yes | |
| Melnyk et al. (2009) [21] | COPE TEEN | USA | 19 | 14–15 years | School | Cluster randomised, controlled educational intervention | 9 weeks | Yes | |
| Schofield et al. (2005) [38] | GSOP | Australia | 85 girls | 15 years | School | Non-randomised, controlled physical activity self-monitoring and education intervention | 6 weeks, 6 week follow-up | No | |
| Stock et al. (2007) [35] | Healthy Buddies | Canada | 383 | 4–11 years | School | Non-randomised, controlled health promotion intervention | 21 weeks | Yes | |
| Johnson et al. (1991) [37] | Heart Smart Program | USA | 19 children 23 parents | 9–13 years | School | Non-randomised, controlled education, physical activity and nutrition intervention involving parents | 12 weeks | No | |
| Nguyen et al. (2012) [22,23,24,25,26] | LOOZIT | Australia | 151 | 13–16 years | Local community health centre and children’s hospital | Randomised, controlled lifestyle modification intervention | 7 weeks, 24 month follow-up | Yes | |
| Sacher et al. (2010) [27] | MEND | UK | 116 | 9–11 | Community (e.g. schools and sports centres) | Randomised, controlled healthy lifestyle intervention | 9 weeks, 12 week follow-up | Yes | |
| Bayne-Smith et al. (2004) [36] | PATH | USA | 442 girls | 14–17 years | School | Randomised, controlled heart health education and physical activity intervention | 12 weeks | Yes | |
| Nemet et al. (2005) [32] | - | Israel | 46 | 8–14 years | Child health and sports centre, Meir General Hospital, Tel Aviv University | Randomised, controlled diet, behaviour and physical activity intervention | 3 months, 1 year follow-up | Yes | |
| Park et al. (2007) [31] | - | Korea | 44 | 13–15 years | School | Randomised, controlled lifestyle and education and exercise intervention | 12 weeks | No | |
| Tershakovec et al. (1998) [28–30] | - | USA | 342 | 6 years | Home | Randomised, controlled nutrition education intervention | 10 weeks, 12 months follow-up | Yes |
The studies reported some improvements in the outcomes of interest following the interventions. The weight of the intervention group was improved in four studies [31–35] while reductions in BMI and BMIz score were seen in seven studies [20, 22–27, 31–35]. The biochemical and functional parameters of CVD were improved by some of the interventions. Specifically, systolic blood pressure was improved in five studies [20, 27, 31, 35, 36], and diastolic blood pressure in two studies [20, 36]. Improvements were also seen in the children’s high density lipoprotein (HDL) cholesterol in one study [21], low density lipoprotein (LDL) cholesterol in two studies [28–31], total cholesterol in two studies [22–26, 31], triglycerides in two studies [22–26, 31], and insulin resistance measured by the homeostasis model assessment of insulin resistance (HOMA-IR) in one study [31] (see S1 Table).
The non-biological outcomes also saw some improvements after the interventions. Health behaviours were improved in eleven studies [20–30, 32–38], health knowledge was increased in four studies [21, 28–30, 35, 36], and the children’s attitudes to health were improved in one study [35]. Table 2 shows the outcomes that were improved in each of the studies.
Table 2. Component themes.
| Main theme | Sub-components |
|---|---|
| Health Behaviours | Diet, physical activity, lifestyle compatible activities, focus on fitness, familiarity with fruit and vegetables |
| Self-Concept | Self-esteem, body image, self-efficacy |
| Practical and Cognitive Tools | Goal setting, problem solving, stress management, practical skills (e.g. interpreting nutrition labels and food preparation) |
| Intervention Characteristics | Take home materials, deliverer resources, focus away from weight, involvement of others (e.g. parents, peers, community), interactive, homework, focus on behaviour, attitude and knowledge change, professional involvement (e.g. dietician). |
The included studies were not without shortcomings in their methods and data. The most common of these being improvements that were not sustained at follow-up, short follow-up periods, and when confounding factors were controlled for, changes seen in only one age or gender group. The inclusion of a follow-up period was an area in which much variation was seen between studies. Of the 12 included studies, five had follow-up periods ranging from six weeks to one year (Table 1). It may be expected that studies that followed-up their participants would have been less likely to achieve improvements in the biological and non-biological factors of interest, as the effect of the study lessens over time. This was not the case, however, as of the five studies only one, which also had the shortest follow-up, did not report improvements in both the biological and non-biological factors.
Components common to changes in outcomes
In order to ascertain which components were present in studies that brought about a positive change in the outcomes of interest, any papers which failed to improve at least one biological and one non-biological outcome were excluded. This left nine out of the twelve included studies remaining [20–30, 32–36]. Of the three excluded studies, Schofield, Mummery and Schofield (2005) [38] and Johnson et al. (1991) [37] were able to bring about some significant improvements in physical activity and dietary measures, however these were not accompanied by significant improvements in the biological factors of interest as defined above. Park et al. (2007) [31] reported significant improvements in many of the biological factors of interest, but did not report any changes in non-biological factors. These studies reported interventions that were among the shortest of those included in this analysis which could have meant that they were not long enough for significant improvements to be seen. There were those, however, that did achieve improvements in both the biological and non-biological factors that were of similar length, and so we must assume that the different outcomes seen were due to the differences in how the interventions were constructed, delivered, and assessed. For the details of which factors were improved in all 12 studies see S1 Table.
Table 2 shows the components common to the nine studies that had achieved an improvement in both biological and non-biological outcomes. The components were grouped into component themes and each theme is discussed below.
Health behaviours
The subcomponents of this theme focussed on instructing the children in healthy eating [20–30, 32–34, 36] and physical activity [20–26, 32–36]. The healthy eating component included learning about the food pyramid [32], setting targets like reducing the consumption of sugar sweetened drinks, increasing the consumption of fruit and vegetables [27, 33, 34], and increasing the children’s familiarity with different fruit and vegetables [20]. Physical activity included encouraging the children to increase the amount of time they spent being active [32], physical education (PE) lessons that placed greater importance on fitness [20, 32, 35], and activities that could easily be incorporated into the children’s lifestyles [21, 33, 34]. Of the studies that included instruction in healthy eating, all nine studies brought about significant (p-values ≤ 0.05) improvements in the children’s diets. Such improvements included reductions in carbonated and fruit juice drinks, reduction in fats and oils consumed, increases in the number of children eating breakfast and increases in fruit and vegetable servings consumed. Seven of the eight studies targeting physical activity brought about significant (p-values ≤ 0.05) improvements which included reductions in screen time and increases in extra-curricular physical activity.
Self-concept
This theme included three sub-components; self-esteem, healthy body image [20–26, 35], and self-efficacy [20]. Self-esteem and healthy body image was addressed through discussions to change self-concept, role-modelling, education in growth and development, and introducing techniques such as positive thinking and self-talk. Self-esteem and body image were assessed using a pictorial current-self and ideal-self rating scale, the Beck Youth Inventory [39], which includes a sub-scale on self-concept, or the Harter Self-Perception Profile [40]. Significant improvements in self-esteem or body satisfaction were reported in the LOOZIT study (global self-worth; 0.21, 95% CI 0.01 to 0.32, p<0.001 and body shape dissatisfaction; -0.56, 95% CI -0.74 to -0.38, p<0.001) and the MEND study (global self-esteem score increase; 0.3, 95% C.I. 0.0 to 0.5, p = 0.03) [23, 27]. However, even in the studies where such improvements were not found, there were improvements to the children’s attitudes towards their health, which could have been facilitated by attempts to increase self-esteem.
Increasing self-efficacy to lead healthy lives was targeted specifically by the CHILDREN programme [20]. Self-efficacy was targeted through techniques such as modelling, enactment and guided practice in weekly sessions that lasted one to two hours [20]. This study did not, however, measure the change in self-efficacy, instead, change in diet, physical activity and sedentary behaviour were measured.
Practical and cognitive tools
The practical and cognitive tools theme included components such as goal setting, where the children had to make goals for themselves and report back at a later time whether these were achieved or not [20, 22–26]. Where they were not achieved, discussions were held about the reasons why this may be and ways in which problems arising could be dealt with. Children were given practical skills such as how to read nutrition labels on food packaging, how to modify recipes to make them healthier, and how to make healthy choices, for example when eating at a restaurant [27, 32]. Cognitive skills, such as ways in which stress could be managed more effectively through improving the children’s communication skills, were also used by some studies [22–26].
All of the studies that aimed to provide children with practical or cognitive skills achieved improvements in either one or both of their physical activity levels and diet.
Intervention characteristics
Unlike the preceding three themes, the intervention characteristics theme summarised the ways in which the successful interventions were delivered rather than what they delivered. Common characteristics included interventions that were interactive, the children were encouraged to discuss, play games and use role play to facilitate their learning [20], and that both children and those delivering the intervention were provided with materials such as workbooks [20, 22–26, 28–30, 32–34]. The children’s workbooks contained physiological and health information, activities, and space to enter their own thoughts that could be kept after the intervention had finished. Materials given to the researchers or teachers were often provided with the intention of keeping the delivery of the intervention consistent across lessons and were made up of instructions on delivering the intervention, reproducible materials for the children, and guidance on how the intervention should be assessed.
A common component was the involvement of parents, peers or the community so that general knowledge could be increased and support given to the children participating in the intervention [22–26, 28–30, 32, 37]. Finally, some of the studies used professionals, such as dieticians, in the design and delivery of the intervention [28–30, 32].
Discussion
The purpose of this component analysis was to establish the components common to interventions in children that contribute to improvements in cardiovascular health parameters. The components we identified were classified into four themes: Health Behaviours, Self-Concept, Practical and Cognitive Tools, and Intervention Characteristics. To the best of our knowledge, this is the only study that has set out to determine which components are common to successful interventions to improve cardiovascular health in school aged children. Although the components of successful cardiovascular health promotion interventions have not been summarised previously, the themes that we have identified have been explored individually to a greater or lesser extent. A previous systematic review found inconsistent results when health behaviours were targeted to tackle obesity when only nine out of 20 interventions were able to show a significant improvement in mean BMI in the intervention group [41]. These papers were however seeking to change the BMI of their child participants, a goal that has been recognised to be difficult to achieve especially in the long term [42], and which was not the aim for this component analysis.
The Self Concept theme was created to encompass both self-esteem and self-efficacy. Self-efficacy forms a central part of Social Cognitive Theory, whereby the belief that an individual is able to act in order to bring about a desired change is central to them taking on that action [43]. As CVD is so strongly linked to behavioural factors, an individual’s self-efficacy to make lifestyle choices that are healthful rather than harmful, or modify their harmful behaviours is very important in preventing CVD.
The Practical and Cognitive Tools theme has been discussed previously in a 2011 paper by Lueke [44]. This paper advocates teaching children how to make healthy decisions and face the challenge of living healthily, rather than shielding them from unhealthy influences. The paper recommends that children are provided with such tools, even though some may argue that they have little control over their own diets, as they will be able to practice their newly gained skills while they are young and so will be prepared for when they have to make all their own decisions [44].
Finally the Intervention Characteristics theme suggests ways in which successful interventions should be carried out including the provision of student and teacher materials to ensure the faithful delivery of the intervention and the avoidance of type III errors. Type III errors have been defined as the attempt to assess the effectiveness of an intervention that has not been carried out in the way it has been designed, so that there is no testable relationship between the intervention and the factors it was designed to influence [45]. Therefore, by including instructions for teachers and materials for both teachers and students the risk of type III errors may be reduced.
Strengths and weaknesses
The strength of this component analysis lies in the structured and systematic way in which relevant studies were identified for inclusion and the efforts made to ensure that their design was as comparable as possible. In this way 12 studies were selected and four component themes were identified that have been used to promote heart health to children and were successful at least in the short term. This component analysis is however not without its weaknesses. It is possible that our database search failed to identify some relevant studies that should have been included in the analysis. It is our belief however that as our searches were designed carefully and carried out in multiple databases this is unlikely. A second weakness is that although great care was taken to ensure that the included studies were as comparable and matched our requirements as closely as possible, there was still a level of heterogeneity among them in the ways in which they were delivered, their duration and the characteristics of the children to whom they were delivered. We believe however that as this analysis was descriptive rather than quantitative, this limitation is not serious enough to negate the findings.
Implication for research and practice
The purpose of this study was to identify the components associated with education interventions that were successful in improving the health and health behaviours of children so that they might be incorporated into new interventions to target childhood cardiovascular health. It was found that an emphasis should be placed on how behaviours impact on internal mechanisms so that why healthy living is important might be highlighted to children. Second, the self-esteem of the child should always be central to any intervention and interventions should be designed so that weight bias is not perpetuated, but instead children are encouraged to see themselves as able to influence their own health outcomes and are equipped with the confidence and self-efficacy to do so. Third, children should be given practical and cognitive tools by health lessons that will assist them in their health decision making. Such skills could include stress management, reading nutrition labels, understanding how diet and physical activity interact to either promote or impede health, adapting recipes, and communication skills. Finally, health lessons should be interactive and hands on with materials for both the student and the teachers delivering the lessons so that they may be delivered with fidelity to the intervention design, allowing the effectiveness of the intervention to be assessed appropriately.
Conclusion
The component themes identified were Health Behaviours, Self-Concept, Practical and Cognitive Skills and Intervention Characteristics. We conclude that as these themes have arisen from intervention studies that have had success in improving the health and health behaviours of children, they should be incorporated into future studies with similar aims so that these studies might build on the knowledge gained by their predecessors.
Supporting Information
(DOC)
(DOCX)
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
The authors disclosed receipt of the following financial support for the research, authorship, or publication of this article: a Medical Research Council doctoral training support grant for Claire Friedemann Smith paid to the University of Oxford but did not contribute funding to this work.
References
- 1. Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity: public-health crisis, common sense cure. The Lancet 2002;360(9331):473–82. [DOI] [PubMed] [Google Scholar]
- 2. National Obesity Observatory. International comparisons of obesity prevalance Observatories Association of Public Health Observatories, editor: NHS, 2009. [Google Scholar]
- 3. World Health Organisation. Obesity: preventing and managing the global epidemic: report of a WHO consultation Geneva: World Health Organisation, 2000. [PubMed] [Google Scholar]
- 4. Lim S. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet 2012(380):2224–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Freedman DS, Dietz WH, Srinivasan SR, Berenson GS. The Relation of Overweight to Cardiovascular Risk Factors Among Children and Adolescents: The Bogalusa Heart Study. Pediatrics 1999;103(6):1175–82. [DOI] [PubMed] [Google Scholar]
- 6. Aggoun Y, Farpour-Lambert NJ, Marchand LM, Golay E, Maggio ABR, Beghetti M. Impaired endothelial and smooth muscle functions and arterial stiffness appear before puberty in obese children and are associated with elevated ambulatory blood pressure. Eur. Heart J. 2008;29(6):792–99. [DOI] [PubMed] [Google Scholar]
- 7. Stabouli S, Kotsis V, Papamichael C, Constantopoulos A, Zakopoulos N. Adolescent Obesity is Associated with High Ambulatory Blood Pressure and Increased Carotid Intimal-Medial Thickness. The Journal of Pediatrics 2005;147(5):651–56. [DOI] [PubMed] [Google Scholar]
- 8. Morrison KM, Shin S, Tarnopolsky M, Taylor VH. Association of depression & health related quality of life with body composition in children and youth with obesity. Journal of Affective Disorders 2014; 172: 18–23. [DOI] [PubMed] [Google Scholar]
- 9.The Pensions Commission. A New Pensions Settlement for the Twenty-First Century, The Second report of the Pensions Commission. London, 2005.
- 10.Department of Health. Department of Health- Spending review, 2010.
- 11. Puhl RM, Latner JD. Stigma, Obesity, and the Health of the Nation’s Children. Psychological Bulletin 2007;133 (4): 557–580. [DOI] [PubMed] [Google Scholar]
- 12. Ciampa PJ, Kumar D, Barkin SL, Sanders LM, Yin HS, Perrin EM, et al. Interventions aimed at decreasing obesity in children younger than 2 years: A systematic review. Archives of Pediatrics and Adolescent Medicine 2010;164 (12):1098–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Bond M, Wyatt K, Lloyd J, Taylor R. Systematic review of the effectiveness of weight management schemes for the under fives. Obesity Reviews 2011;12 (4):242–53. [DOI] [PubMed] [Google Scholar]
- 14. Collins CE, Warren J, Neve M, McCoy P, Stokes BJ. Measuring effectiveness of dietetic interventions in child obesity: A systematic review of randomized trials. Archives of Pediatrics and Adolescent Medicine 2006;160 (9):906–22. [DOI] [PubMed] [Google Scholar]
- 15. Silveira JAC, Taddei JAAC, Guerra PH, Nobre MRC. Effectiveness of school-based nutrition education interventions to prevent and reduce excessive weight gain in children and adolescents: A systematic review. Jornal de Pediatria 2011;87 (5):382–92. [DOI] [PubMed] [Google Scholar]
- 16. van Grieken A, Ezendam NPM, Paulis WD, van der Wouden JC, Raat H. Primary prevention of overweight in children and adolescents: A meta-analysis of the effectiveness of interventions aiming to decrease sedentary behaviour. International Journal of Behavioral Nutrition and Physical Activity 2012;9(61). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Li M, Li S, Baur LA, Huxley RR. A systematic review of school-based intervention studies for the prevention or reduction of excess weight among Chinese children and adolescents. Obesity Reviews 2008;9 (6):548–59. [DOI] [PubMed] [Google Scholar]
- 18. Campbell K, Waters E, O'Meara S, Summerbell C. Interventions for preventing obesity in childhood. A systematic review. Obesity Reviews 2001;2(3):149–57. [DOI] [PubMed] [Google Scholar]
- 19. Ward A, Heneghan C, Perera R, Lasserson D, Nunan D, Mant D, et al. What are the basic self-monitoring components for cardiovascular risk management? BMC Medical Research Methodology 2010;10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Angelopoulos PD, Milionis HJ, Grammatikaki E, Moschonis G, Manios Y. Changes in BMI and blood pressure after a school based intervention: The CHILDREN study. European Journal of Public Health 2009;19 (3):319–25. [DOI] [PubMed] [Google Scholar]
- 21. Melnyk BM, Jacobson D, Kelly S, O'Haver J, Small L, Mays MZ. Improving the Mental Health, Healthy Lifestyle Choices, and Physical Health of Hispanic Adolescents: A Randomized Controlled Pilot Study. Journal of School Health 2009;79 (12):575–84. [DOI] [PubMed] [Google Scholar]
- 22. Nguyen B, Shrewsbury VA, O'Connor J, Steinbeck KS, Lee A, Hill AJ, et al. Community-based adolescent weight management with additional therapeutic contact: Twelve month outcomes of the Loozit RCT. Obesity Reviews 2011; 12:278–79. [Google Scholar]
- 23. Nguyen B, Shrewsbury VA, O'Connor J, Steinbeck KS, Lee A, Hill AJ, et al. Twelve-Month Outcomes of the Loozit Randomized Controlled Trial A Community-Based Healthy Lifestyle Program for Overweight and Obese Adolescents. Archives of Pediatrics & Adolescent Medicine 2012;166(2):170–77. [DOI] [PubMed] [Google Scholar]
- 24. O'Connor J, Steinbeck K, Hill A, Booth M, Kohn M, Shah S, et al. Evaluation of a community-based weight management program for overweight and obese adolescents: The Loozit study. Nutr. Diet. 2008;65(2):121–27. [Google Scholar]
- 25. Shrewsbury VA, Nguyen B, O'Connor J, Steinbeck KS, Lee A, Hill AJ, et al. Short-term outcomes of community-based adolescent weight management: The Loozit Study. BMC Pediatrics 2011;11:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Shrewsbury VA, O'Connor J, Steinbeck KS, Stevenson K, Lee A, Hill AJ, et al. A randomised controlled trial of a community-based healthy lifestyle program for overweight and obese adolescents: the Loozit study protocol. BMC Public Health 2009;9:119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Sacher PM, Kolotourou M, Chadwick PM, Cole TJ, Lawson MS, Lucas A, et al. Randomized Controlled Trial of the MEND Program: A Family-based Community Intervention for Childhood Obesity. Obesity 2010, 18, S62–S68. [DOI] [PubMed] [Google Scholar]
- 28. Shannon B, Greene G, Stallings V, Achterberg C, Berman MK, Gregoire J, et al. A dietary education program for hypercholesterolemic children and their parents. J Am Diet Assoc 1991;91(2):208–12. [PubMed] [Google Scholar]
- 29. Shannon BM, Tershakovec AM, Martel JK, Achterberg CL, Cortner JA, Smiciklas-Wright HS, et al. Reduction of elevated LDL-cholesterol levels of 4- to 10-year-old children through home-based dietary education. Pediatrics 1994;94(6 Pt 1):923–7. [PubMed] [Google Scholar]
- 30. Tershakovec AM, Shannon BM, Achterberg CL, McKenzie JM, Martel JK, Smiciklas-Wright H, et al. One-year follow-up of nutrition education for hypercholesterolemic children. American Journal of Public Health 1998;88(2):258–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Park TG, Hong HR, Lee J, Kang HS. Lifestyle plus exercise intervention improves metabolic syndrome markers without change in adiponectin in obese girls. Annals of Nutrition & Metabolism 2007;51(3):197–203. [DOI] [PubMed] [Google Scholar]
- 32. Nemet D, Barkan S, Epstein Y, Friedland O, Kowen G, Eliakim A. Short- and long-term beneficial effects of a combined dietary-behavioral- physical activity intervention for the treatment of childhood obesity. Pediatrics 2005;115 (4):e443–e49. [DOI] [PubMed] [Google Scholar]
- 33. Taylor RW, McAuley KA, Barbezat W, Strong A, Williams SM, Mann JI. APPLE Project: 2-y findings of a community-based obesity prevention program in primary school-age children. American Journal of Clinical Nutrition 2007;86 (3):735–42. [DOI] [PubMed] [Google Scholar]
- 34. Taylor RW, McAuley KA, Williams SM, Barbezat W, Nielsen G, Mann JI. Reducing weight gain in children through enhancing physical activity and nutrition: the APPLE project. International Journal of Pediatric Obesity 2006;1(3):146–52. [DOI] [PubMed] [Google Scholar]
- 35. Stock S, Miranda C, Evans S, Plessis S, Ridley J, Yeh S, et al. Healthy buddies: A novel, peer-led health promotion program for the prevention of obesity and eating disorders in children in elementary school. Pediatrics 2007;120 (4):e1059–e68. [DOI] [PubMed] [Google Scholar]
- 36. Bayne-Smith M, Fardy PS, Azzollini A, Magel J, Schmitz KH, Agin D. Improvements in heart health behaviors and reduction in coronary artery disease risk factors in urban teenaged girls through a school-based intervention: the PATH program. American Journal of Public Health 2004;94(9):1538–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Johnson CC, Nicklas TA, Arbeit ML, Harsha DW, Mott DS, Hunter SM, et al. Cardiovascular intervention for high-risk families: the Heart Smart Program. Southern Medical Journal 1991;84(11):1305–12. [DOI] [PubMed] [Google Scholar]
- 38. Schofield L, Mummery WK, Schofield G. Effects of a controlled pedometer-intervention trial for low-active adolescent girls. Medicine and Science in Sports and Exercise 2005;37 (8):1414–20. [DOI] [PubMed] [Google Scholar]
- 39. Beck JS, Beck A, Jolly J. Beck Youth Inventories for Children and Adolescents: Manual. 2nd ed. San Antonio, Texas: Harcourt Assessment, 2005. [Google Scholar]
- 40. Harter S. Manual for the Self Perception Profile for Adolescents. Denver: University of Denver, 1988. [Google Scholar]
- 41. Brown T, Summerbell C. Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: an update to the obesity guidance produced by the National Institute for Health and Clinical Excellence. Obesity Reviews 2009, 10: 1, 110–141 [DOI] [PubMed] [Google Scholar]
- 42. Caballero B. Obesity prevention in children: opportunities and challenges. International Journal of Obesity 2004, 28, S90–S95. [DOI] [PubMed] [Google Scholar]
- 43. Bandura A. Health Promotion by Social Cognitive Means. Health Education and Behaviour 2004, 31:143. [DOI] [PubMed] [Google Scholar]
- 44. Lueke L. Devouring Childhood Obesity by Helping Children Help Themselves. Journal of Legal Medicine 2011, 32:2, 205–220. [DOI] [PubMed] [Google Scholar]
- 45. Scanlon JW, Horst P, Nay JN, Schmidt RE, Waller JD. Evaluability assessment: Avoiding type III and IV errors, in Gilbert GR, Conklin PJ (eds): Evaluation Management: A Source Book of Readings. Charlottesville, VA: US Civil Service Commission, 1977. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOC)
(DOCX)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.