

Abstract
The lateral limit of endoscopic endonasal surgery has yet to be defined. The aim of this study was to investigate the lateral limit of endoscopic endonasal surgery at the level of the sphenoid sinus. Access from the sphenoid sinus to the middle cranial fossa through the cavernous sinus triangles was evaluated by cadaver dissection. Anatomical analysis demonstrated that the medial temporal dura mater was exposed through the anterior area of the clinoidal triangle, anteromedial triangle, and superior area of the anterolateral triangle, indicating potential corridors to the middle cranial fossa. This study suggests that the cavernous sinus triangles are applicable in selected cases to manage middle cranial fossa lesions by endoscopic endonasal surgery.
Keywords: cavernous sinus, endoscopy, internal carotid artery, skull base
Introduction
Recent advances in endoscopic endonasal surgery have facilitated minimally invasive ventral skull base surgery.1–5) Although the endoscopic endo-nasal approach allows access to a longitudinally spacious area from the frontal sinus to the axis, lateral extension is limited because the corridor is surrounded by vital structures.6) The cavernous sinus is situated at the border between the sphenoid sinus and the floor of the middle cranial fossa, and is thought to represent a substantial lateral limit for the endoscopic endonasal approach at the level of the sphenoid sinus. However, from an anatomical perspective, the cranial nerves in the lateral and superior walls of the cavernous sinus have small areas known as the cavernous sinus triangles (Fig. 1a).7) These triangles are known to be the entrances from the middle cranial fossa to the cavernous sinus during transcranial skull base surgery. In contrast, these triangles might represent potential corridors to the middle cranial fossa in endoscopic endonasal surgery. The present anatomical analysis was performed to clarify the lateral limits of endoscopic endonasal surgery.
Fig. 1.
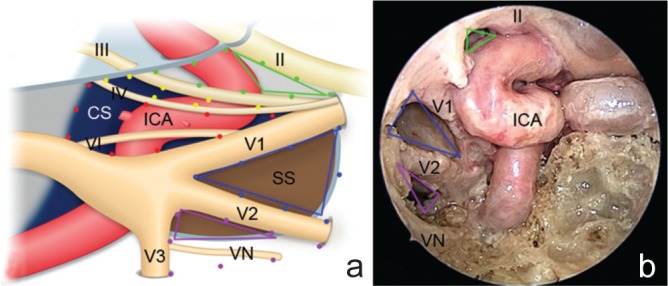
Schematic portrayal (a) and endoscopic view (b) of the cavernous sinus triangles. a: The clinoid triangle is delineated by the optic nerve, oculomotor nerve, and dura mater between the optic nerve and oculomotor nerve (green dotted lines). The anterior clinoid process is situated in the clinoid triangle in normal structures. The supra- and infratrochlear triangles are defined by the oculomotor nerve, trochlear nerve, and dura mater between the oculomotor and trochlear nerves (yellow dotted lines), and by the trochlear nerve, first division of the trigeminal nerve and dura mater between the trochlear nerve and first division of the trigeminal nerve (red dotted lines), respectively. The anteromedial and anterolateral triangles are defined by the first and second divisions of the trigeminal nerves and a line between the superior orbital fissure and foramen rotundum (blue dotted lines), and by the second and third divisions of the trigeminal nerve and a line between the foramen rotundum and foramen ovale (purple dotted lines), respectively. The ICA runs medial to the cranial nerves and across the clinoidal, supratrochlear, and infratrochlear triangles. b: The anterior area of the clinoidal triangle (green lines), anteromedial triangle (blue lines), and superior area of the anterolateral triangle (purple lines) are shown from the endoscopic endonasal approach. These triangles exposed by the endoscopic endonasal approach are situated anterior to the ICA, and correspond to the areas indicated (a).16) CS: cavernous sinus, ICA: internal carotid artery, SS: sphenoid sinus, VN: Vidian nerve, II: optic nerve, III: occulomotor nerve, IV: trochlear nerve, V1: first division of the trigeminal nerve, V2: second division of the trigeminal nerve, V3: third division of the trigeminal nerve, VI: abducens nerve.
Materials and Methods
All anatomical dissections were performed in the Laboratory of Microsurgical and Endoscopic Anatomy at the Medical University of Vienna. The study protocols were approved by the local institutional research committee. The cavernous sinus and surrounding structures were studied via an endoscopic endonasal approach. Specimens were injected with red silicone through the arterial system. The venous system was not injected, to facilitate recognition of cavernous sinus nerves and arteries. A 4-mm-diameter endo-scope, 18 cm in length, was used with 0° and 30° rod-lenses (Karl Storz, Tuttlingen, Germany). The endoscope was connected to a light source through a fiberoptic cable and to a camera fitted with three-chip, high-definition sensors. The video camera was connected to a monitor for optimal display of the high-definition images.
Results
Following posterior nasal septectomy and anterior sphenoidectomy, the middle turbinate, uncinate process, bulla ethmoidalis, and posterior ethmoidal cells were removed. Maxillary a ntrostomy was performed and the posterior wall of the maxillary sinus was partially removed, exposing the superomedial part of the pterygopalatine fossa. The contents of the pterygopalatine fossa were displaced laterally, and the medial pterygoid process, foramen rotundum, and Vidian canal were identified. The medial pterygoid process was then drilled out. This corridor provided a direct trajectory to the lateral wall of the sphenoid sinus. Sellar and parasellar bones, optic canal, and the bony lateral wall of the sphenoid sinus were opened, widely exposing the dura mater of the parasellar area and cavernous sinus. The dura mater of the cavernous sinus was removed, revealing the contents of the cavernous sinus (Fig. 2a). The anterior clinoid process was located below the optic nerve sheath and lateral to the internal carotid artery (ICA). The ICA was displaced medially, and then the oculomotor nerve running to the superior orbital fissure became visible. The carotid-oculomotor membrane bridging between the oculomotor nerve and ICA was seen to attach to the inferior surface of the anterior clinoid process (Fig. 2b). The area surrounded by the optic nerve, oculomotor nerve, and ICA was the clinoidal triangle visualized from the endonasal route. This triangle corresponded only to the anterior area of the clinoidal triangle (Fig. 1a, b). In another specimen, in which the anterior clinoid process and carotid-oculomotor membrane had been removed and the medial temporal dura mater had been elevated from the middle cranial fossa floor through the transcranial route, the frontal and medial temporal dura mater were able to be reached through the clinoidal triangle via the endonasal route (Fig. 2c). The anterior area of the clinoidal triangle was exposed without medial displacement of the ICA (Fig. 1b).
Fig. 2.
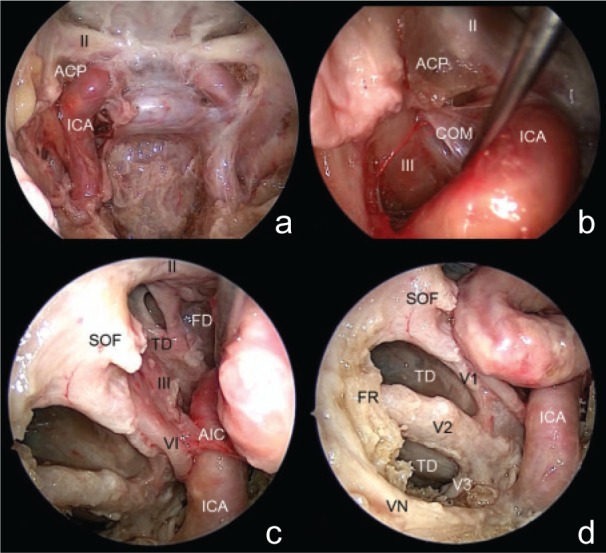
Endoscopic anatomy of cavernous sinus triangles. a: The dura mater over the right cavernous sinus is removed and contents of the cavernous sinus are shown. b: The area surrounded by the optic nerve, oculomotor nerve, and ICA is the clinoidal triangle as visualized from the endonasal route. This triangle corresponds with only the anterior area of the clinoidal triangle. An endoscopic view of the clinoid triangle with the anterior clinoid process show the anterior clinoid process located below the optic nerve and lateral to the ICA. Medial displacement of the ICA reveals that the carotid-oculomotor membrane bridging between the oculomotor nerve and ICA attaches to the inferior surface of the anterior clinoid process. c: The clinoid triangle without the anterior clinoid process shows the medial temporal and frontal dura mater through the clinoid triangle. Exposure of the supra- and infra-trochlear triangles is restricted by the abducens nerve, artery of the inferior cavernous sinus, and ICA. d: The anteromedial triangle is defined by the first and second divisions of the trigeminal nerve and a line between the superior orbital fissure and the foramen rotundum. The anterolateral triangle, delimited by the second and third divisions of the trigeminal nerve, is partially recognizable. Because the inferior area of the anterolateral triangle is covered by the sphenoidal bone behind the Vidian nerve, only the superior area of the anterolateral triangle, as delineated by the second division of the trigeminal nerve, proximal segment of the third division of the trigeminal nerve, and the Vidian nerve, is exposed. Inferomedial temporal dura mater is apparent through the entire anteromedial triangle and superior area of the anterolateral triangle.16) ACP: anterior clinoid process, AIC: artery of the inferior cavernous sinus, COM: carotid-oculomotor membrane, FD: frontal dura mater, FR: foramen rotundum, ICA: internal carotid artery, SOF: superior orbital fissure, TD: temporal dura mater, VN: Vidian nerve, V1: first division of the trigeminal nerve, V2: second division of the trigeminal nerve, V3: third division of the trigeminal nerve, II: optic nerve, III: occulomotor nerve, VI: abducens nerve.
The supra- and infratrochlear triangles were slightly exposed after medial displacement of the ICA, which was restricted by the artery of the inferior cavernous sinus bridging between the ICA and the lateral wall of the cavernous sinus (Fig. 2c). The supra- and infratrochlear triangles showed narrow spaces compared to other triangles. The oculomotor nerve, trochlear nerve, first division of the trigeminal nerve, and abducens nerve ran together into the superior orbital fissure, comprising a nerve bundle. The supra- and infratrochlear triangles are thus narrower anteriorly and wider posteriorly. Moreover, the abducens nerve, artery of the inferior cavernous sinus, and ICA prevented exposure of a wider posterior area of the supra- and infratroch-lear triangles (Fig. 2c). Reaching the middle cranial fossa through the supra- and infra triangles is thus impossible, even in anatomical analysis.
The second and third divisions of the trigeminal nerves pass through the foramen rotundum and foramen ovale, respectively. The entire anteromedial triangle, composed by the first and second divisions of the trigeminal nerve, was apparent (Fig. 2d). The anterolateral triangle, delimited by the second and third divisions of the trigeminal nerve, was partially recognizable (Fig. 2d). The superior area of the anterolateral triangle delineated by the second division of the trigeminal nerve, proximal segment of the third division of the trigeminal nerve, and the Vidian nerve, was revealed, while the inferior area of the anterolateral triangle was covered by the sphenoidal bone behind the Vidian nerve (Fig. 1b, 2d). The inferomedial temporal dura mater was visualized through the entire anteromedial triangle and superior area of the anterolateral triangle (Fig. 2d).
Discussion
The cavernous sinus is an intricate structure located in the central skull base. Microsurgical anatomical studies have investigated detailed neurovascular relationships in the cavernous sinus and various surgical approaches to the cavernous sinus have been developed over recent decades.7–12) In addition, the anatomy of the medial cavernous sinus has also been analyzed using an endoscopic endonasal approach in recent years.13–16) Cavallo et al. compared the cavernous sinus triangles via transcranial and endoscopic endonasal routes, and described the anatomical features of the cavernous sinus under endoscopic views.14) Anatomical views of the cavernous sinus triangles via endoscopic endonasal approaches differ from transcranial views in terms of not only trajectory, but also exposed area. Because the cavernous portion of the ICA is located medially in the cavernous sinus, views from the endoscopic endonasal approach are greatly influenced by the ICA. The posterior elements of the cavernous sinus triangles behind the ICA are not visualized, so exposure of the entire area of cavernous sinus triangles, particularly most of the areas of the supra- and infratrochlear triangles, is impractical even in cadaveric investigation. Only the entire anteromedial triangle, anterior area of the clinoidal triangle, and superior area of the anterolateral triangle are exposed, and these three areas are thought to represent potential pathways to the middle cranial fossa in endoscopic endonasal surgery.
While opening the normal cavernous sinus carries a risk of hazardous venous bleeding, such bleeding is controllable in cavernous sinus tumors because of regression of the venous system by tumors. Furthermore, the cavernous sinus triangles usually represent small spaces, whereas cavernous sinus tumors enlarge the triangular area. Erosion of the anterior clinoid process by tumor would allow better access to the clinoidal triangle without anterior clinoidectomy. Pathological conditions such as adenomas invading the cavernous sinus protruding the lateral wall of the cavernous sinus would be favored candidates for management by endoscopic endonasal surgery, because such tumors are often soft and suckable.
Identification of the ICA is essential when exposing the cavernous sinus triangles during endoscopic cavernous sinus tumor surgery. We identify the ICA based on dural structures around the superior cavernous sinus, rather than by bony features which are often destroyed by tumors.17) Pursuing the optic nerve sheath medially after drilling the optic canal can lead to the proximal orifice of the optic nerve sheath at the transition between the optic nerve sheath and dura mater of the tuberculum sellae. Just below the proximal orifice of the optic nerve sheath, the distal dural ring encasing the clinoid segment of the ICA becomes readily identifiable. Exposure of the optic nerve and clinoid segment of the ICA allows the clinoid triangle to be opened, accessing superior cavernous sinus pathology with extension to the middle cranial fossa. Concerning the inferior cavernous sinus, previous anatomical and clinical reports have mentioned exposure of the Vidian nerve as a reliable landmark for the lacerum segment of the ICA.18,19) Anatomical landmarks including the ICA, superior orbital fissure, foramen rotundum, foramen ovale, and Vidian nerve would offer access to the anteromedial and anterolateral triangles.
The cavernous sinus is defined as the lateral limit of the endoscopic endonasal approach in normal anatomy. However, when a pathology occupies the cavernous sinus and protrudes into the middle cranial fossa, the limits of endoscopic endonasal approach may vary. Detailed knowledge of endoscopic endonasal anatomy and careful selection of pathological indications would expand the limits of endoscopic endonasal surgery.
References
- 1). Cappabianca P, Cavallo LM, Esposito F, De Divitiis O, Messina A, De Divitiis E: Extended endoscopic endonasal approach to the midline skull base: the evolving role of transsphenoidal surgery. Adv Tech Stand Neurosurg 33: 151– 199, 2008. [DOI] [PubMed] [Google Scholar]
- 2). Kassam A, Snyderman CH, Mintz A, Gardner P, Carrau RL: Expanded endonasal approach: the rostrocaudal axis. Part I. Crista galli to the sella turcica. Neurosurg Focus 19: E3, 2005. [PubMed] [Google Scholar]
- 3). Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R: Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus 19: E6, 2005. [PubMed] [Google Scholar]
- 4). Kassam A, Snyderman CH, Mintz A, Gardner P, Carrau RL: Expanded endonasal approach: the rostrocaudal axis. Part II. Posterior clinoids to the foramen magnum. Neurosurg Focus 19: E4, 2005. [PubMed] [Google Scholar]
- 5). Shin M, Kondo K, Saito N: Neuroendoscopic transnasal surgery for skull base tumors: basic approaches, avoidance of pitfalls, and recent innovations. Neurol Med Chir (Tokyo) 52: 697– 703, 2012. [DOI] [PubMed] [Google Scholar]
- 6). Snyderman CH, Pant H, Carrau RL, Prevedello D, Gardner P, Kassam AB: What are the limits of endoscopic sinus surgery?: the expanded endonasal approach to the skull base. Keio J Med 58: 152– 160, 2009. [DOI] [PubMed] [Google Scholar]
- 7). Rhoton AL: The cavernous sinus, the cavernous venous plexus, and the carotid collar. Neurosurgery 51: S375– S410, 2002. [PubMed] [Google Scholar]
- 8). Parkinson D: A surgical approach to the cavernous portion of the carotid artery. Anatomical studies and case report. J Neurosurg 23: 474– 483, 1965. [DOI] [PubMed] [Google Scholar]
- 9). Dolenc VV: A combined epi- and subdural direct approach to carotid-ophthalmic artery aneurysms. J Neurosurg 62: 667– 672, 1985. [DOI] [PubMed] [Google Scholar]
- 10). Sekhar LN, Burgess J, Akin O: Anatomical study of the cavernous sinus emphasizing operative approaches and related vascular and neural reconstruction. Neurosurgery 21: 806– 816, 1987. [DOI] [PubMed] [Google Scholar]
- 11). Hakuba A, Tanaka K, Suzuki T, Nishimura S: A combined orbitozygomatic infratemporal epidural and subdural approach for lesions involving the entire cavernous sinus. J Neurosurg 71: 699– 704, 1989. [DOI] [PubMed] [Google Scholar]
- 12). Komatsu F, Komatsu M, Inoue T, Tschabitscher M: Endoscopic supraorbital extradural approach to the cavernous sinus: a cadaver study. J Neurosurg 114: 1331– 1337, 2011. [DOI] [PubMed] [Google Scholar]
- 13). Alfieri A, Jho HD: Endoscopic endonasal cavernous sinus surgery: an anatomic study. Neurosurgery 48: 827– 836; discussion 836–837, 2001. [PubMed] [Google Scholar]
- 14). Cavallo LM, Cappabianca P, Galzio R, Iaconetta G, de Divitiis E, Tschabitscher M: Endoscopic transnasal approach to the cavernous sinus versus transcranial route: anatomic study. Neurosurgery 56 (2 Suppl): 379– 389; discussion 379–389, 2005. [DOI] [PubMed] [Google Scholar]
- 15). d'Avella E, Tschabitscher M, Santoro A, Delfini R: Blood supply to the intracavernous cranial nerves: comparison of the endoscopic and microsurgical perspectives. Neurosurgery 62( 5 Suppl 2): ONS305– ONS310; discussion ONS310–ONS311, 2008. [DOI] [PubMed] [Google Scholar]
- 16). Komatsu F, Komatsu M, Di Ieva A, Tschabitscher M: Endoscopic approaches to the trigeminal nerve and clinical consideration for trigeminal schwannomas: a cadaveric study. J Neurosurg 117: 690– 696, 2012. [DOI] [PubMed] [Google Scholar]
- 17). Komatsu F, Shimoda M, Oda S, Imai M, Shigematsu H, Komatsu M, Tschabitscher M, Matsumae M: Identification of the internal carotid artery at the superior part of the cavernous sinus during endoscopic endonasal cavernous sinus tumor surgery. Acta Neurochir (Wien) 156: 475– 479, 2014. [DOI] [PubMed] [Google Scholar]
- 18). Kassam AB, Vescan AD, Carrau RL, Prevedello DM, Gardner P, Mintz AH, Snyderman CH, Rhoton AL: Expanded endonasal approach: vidian canal as a landmark to the petrous internal carotid artery. J Neurosurg 108: 177– 183, 2008. [DOI] [PubMed] [Google Scholar]
- 19). Kassam AB, Prevedello DM, Carrau RL, Snyderman CH, Gardner P, Osawa S, Seker A, Rhoton AL, Jr: The front door to meckel's cave: an anterome-dial corridor via expanded endoscopic endonasal approach—technical considerations and clinical series. Neurosurgery 64 (3 Suppl): 71– 82; discussion 82–83, 2009. [DOI] [PubMed] [Google Scholar]