

Abstract
Neck clipping of a large middle cerebral artery aneurysm was performed using a newly developed surgical microscope integrated with modules for both indocyanine green (ICG) and fluorescein videoangiography. During surgery, ICG and fluorescein videoangiography by intra-arterial or intravenous injection were safely carried out without interrupting the surgical procedure. Based on the findings obtained from the case, we evaluated the differences between the dyes and the injection routes. With intra-arterial injection, fluorescein offered sharper contrast images and was better at depicting fine arteries than ICG. Patchy staining of vessel walls was observed in intravenous fluorescein videoangiography, while it was not evident in ICG. Intra-arterial injection method had a great advantage in the rapid clearance of the dyes, which allowed us to perform repeated videoangiography within a short period, and was useful in detecting incomplete clipping in this case; however, catheter insertion requires additional work and carries a potential risk. Use of a microscope integrated for both ICG and fluorescein videoangiography would be another method for repeated evaluation. Namely, alternate use of the dyes enables us to perform videoangiography in a short time even via intravenous injection.
Keywords: clipping, videoangiography, fluorescein, indocyanine green, intracranial aneurysm
Introduction
Intraoperative fluorescence videoangiography has recently been introduced to monitor blood flow during neurosurgical procedures. This technique has been playing important roles in cerebrovascular surgery, especially in intracranial aneurysmal surgery, demonstrating postprocedural blood flow in the aneurysm lumen, parent arteries, and perforating arteries.1–3) Indocyanine green (ICG) and fluorescein have been commonly used for florescence videoangiography. In ophthalmological examinations, both ICG and fluorescein have distinct roles based on their characteristics;4) however, characteristic differences between the two dyes in the same neurosurgical field have been obscured.
Both ICG and fluorescein videoangiography are performed commonly by intravenous injection at present, this procedure, however, cannot be repeated within a short time since both dyes remain in the vessels for longer than 15 minutes.5) Hence, we have applied the intra-arterial injection method which has been established as a safe one,6–8) though catheter insertion into the artery requires some additional work and carries a potential risk.
In the current case, we performed ICG and fluorescein videography during surgery of an unruptured large middle cerebral artery (MCA) aneurysm using a newly developed operating microscope integrated with a module for both ICG and fluorescein videoangiography. Intra-arterial ICG and fluorescein videoangiography were performed repeatedly before and after neck clipping, and intravenous videoangiography was also performed after clipping. We compared the differences between the dyes and the injection routes in the same surgical field for the first time. In addition, we confirmed a great advantage of using a microscope integrated both ICG and fluorescein videoangiography on aneurysmal surgery.
Case Report
A 63-year-old woman was referred to our institute with an unruptured right large MCA aneurysm. A newly developed surgical microscope (OPMI PENTERO 900; Carl Zeiss Meditec AG, Jena, Germany) integrated with modules for both ICG (INFRARED 800TM; Carl Zeiss Meditec AG) and fluorescein videoangiography (YELLOW 560TM; Carl Zeiss Meditec AG) was used for the surgery, and the patient signed written informed consent forms giving us permission to perform intraoperative ICG and fluorescein videoangiography. An angiographic catheter was introduced into the right internal carotid artery to perform intraoperative digital subtraction angiography (DSA). ICG dye (Diagnogreen; Daiichi Sankyo Co., Ltd., Tokyo) or fluorescein sodium (FLUORESCITE®; Alcon Laboratories, Inc., Fort Worth, Texas USA) was administered via the catheter for intraoperative DSA or via a cutaneous vein of the forearm. For intra-arterial injection, 10 ml of 10 μg/ml (0.2%) ICG or 200 μg/ml (0.2%) fluorescein sodium diluted by normal saline was used based on our previous experience. For intravenous use, 5 ml of ICG (5 mg/ml) or fluorescein sodium (100 mg/ml) was injected into a cutaneous vein according to the previous reports.2,3)
The MCA bifurcation aneurysm was exposed by transsylvian approach. Prior to neck clipping, ICG and fluorescein videoangiography were performed (Fig. 1). With intra-arterial injection, both ICG and fluorescein videoangiography clearly depicted the aneurysm and the surrounding arteries immediately after the injection. Both dyes disappeared rapidly (within 10 seconds), which allowed us to repeat videoangiography in a short period. In intra-arterial injection method, fluorescence videoangiography could depict small arteries more clearly than ICG videoangiography. Hence, contrast of images and ability to depict fine arteries were superior in intra-arterial fluorescein videoangiography to in intra-arterial ICG videoangiography. A slightly curved clip was applied to the aneurysmal neck, and videoangiography was performed again. Although the aneurysm appeared to be obstructed completely, videoangiography revealed that both dyes slowly filled into the aneurysmal dome, indicating incomplete clipping. The additional clip was applied to the aneurysmal neck (Fig. 2A), and no increase of the dyes in the aneurysmal dome was confirmed though the residual filling of the dyes in the aneurysm was still observed before the injection (Fig. 2B). Finally, videoangiography via intravenous injection was performed (Fig. 2C). When the artery was illuminated approximately 10–15 minutes after the previous injection, the area of fluorescein emission in the aneurysm was increased, while that with ICG was not (Fig. 2C, at 0 seconds). Intravenous injection could depict the surrounding arteries clearly; however, contrast of the image of intravenous injection was inferior to that of intra-arterial injection, and the dyes remained in the vessels for more than 5 minutes. Prolonged patchy staining of vessel walls was observed in fluorescein videoangiography, which was not evident in ICG.
Fig. 1.
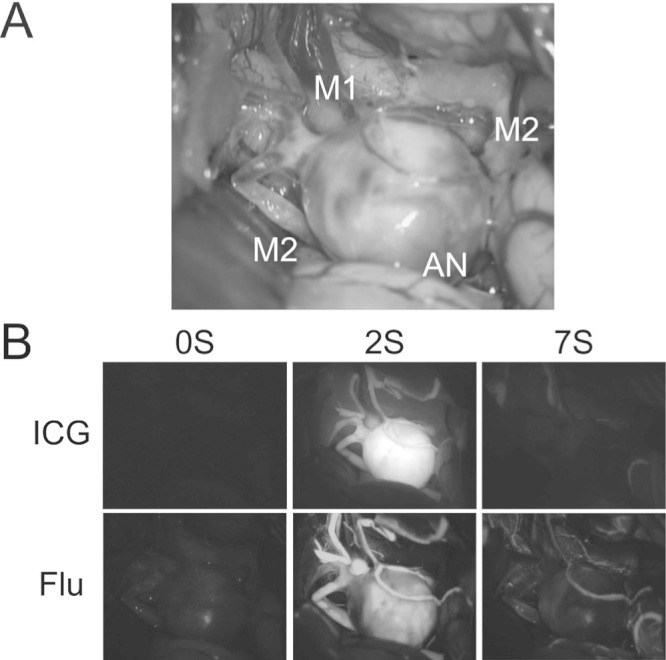
Intraoperative photographs before placement of clips on the aneurysm. A: A right transsylvian approach exposed the large aneurysm (AN), M1 segment, and two M2 segments of the middle cerebral artery. B: Intra-arterial ICG and fluorescein videoangiography clearly depicted the aneurysm and the surrounding arteries immediately after the injection. Contrast of image and ability to depict fine arteries were superior in fluorescein to in ICG. Time after the injection is presented in seconds. Flu: fluorescein, ICG: indocyanine green.
Fig. 2.

Intraoperative photographs after placement of an additional clip. A: Multiple clips were applied to the aneurysmal neck. B: Intra-arterial ICG and fluorescein videoangiography demonstrated no increase of the dyes in the aneurysmal dome, although the residual filling of the dyes in the aneurysm was observed before the injection. C: Intravenous ICG and fluorescein videoangiography could depict the surrounding arteries clearly; however, the dyes remained in the vessels for more than 5 minutes. Prolonged patchy staining of vessel walls was observed in fluorescein videoangiography (arrow). Also note that the area of fluorescein emission in the aneurysm before intravenous injection (at 0 seconds) was larger than that at 10 seconds after intra-arterial injection (B). Flu: fluorescein, ICG: indocyanine green.
Intraoperative DSA also confirmed complete neck clipping. Postoperative computed tomography (CT) scans showed no abnormality and the patient's postoperative course was uneventful.
Discussion
This is the initial case report in which aneurysmal clipping was monitored by both ICG and fluorescein videoangiography. Using a newly developed surgical microscope for both ICG and fluorescein, we could carry out videoangiography of both dyes easily without interrupting the surgical procedure. We closely observed the images of videoangiography and evaluated the differences between the dyes in a same surgical field.
I. Differences between ICG and fluorescein
In our settings, videoangiography of both dyes were very useful in aneurysmal surgery, and any adverse effects of the dyes were not observed. Distinct roles of ICG and fluorescein videoangiography have not been established in neurosurgery, but the current case revealed that there were subtle differences between the two dyes. First, in the intra-arterial injection method, contrast of images and ability to depict fine arteries were superior in fluorescein videoangiography than in ICG. Although information about fine arteries was not necessary in this MCA aneurysm case, intra-arterial injection fluorescein videoangiography will be useful during the surgery of aneurysms near fine perforating arteries. Second, patchy staining of vessel walls was observed in intravenous fluorescein videoangiography, while such phenomenon was not evident in ICG. Fluorescein sodium has a small molecular weight (376 kD) compared to ICG (775 kD), and easily leaks into the blood vessel walls. Consequently, the vascular wall itself comes to emit fluorescence.9) We also observed an interesting phenomenon in which a similar mechanism might participate. The area of fluorescein emission in the aneurysm was increased by the time of intravenous injection (Fig. 2C, at 0 seconds). Since the area of ICG emission was not increased, this might be related to the differences between ICG and fluorescein, i.e., the leak of fluorescein into the aneurysmal wall might cause the increase of the area. Third, in addition to the findings obtained from this case, we previously reported that ICG has an advantage in detecting aneurysms buried in subarachnoid clots, since ICG excitation and fluorescence are near-infrared radiation and can penetrate thin tissue.1) Fluorescein is visible light, and detection of aneurysm in subarachnoid clots using fluorescein videoangiography has not been reported.
II. Differences between injection routes and an advantage of using a microscope for both ICG and fluorescein videoangiography
Although intravenous injection is a common method for fluorescence videoangiography, there are some substantial advantages to intra-arterial injection. First, washout of the dyes with intra-arterial injection is exceedingly superior to that with intravenous injection, which allow us to perform repeated videoangiography before and after clipping. Since real-time monitoring is extremely important in aneurysmal surgery, the superiority in washout time of the dyes is a great advantage of intra-arterial injection. Second, intra-arterial injection method could provide brighter and higher contrast images compared to conventional intravenous injection method. Third, intra-arterial injection method can reduce dose of the dyes. Although toxicities of the ICG and fluorescein were reported to be very low, rare complications such as cardiac reaction and respiratory compromise were reported after administration of ICG or fluorescein.10,11) The lower administration dose of the dyes would bring lower complication rates. On the other hand, there is a disadvantage to intra-arterial injection. Catheter insertion into the artery requires some additional work, and carries a potential risk. The newly developed microscope used in this case, which can perform both ICG and fluorescein videoangiography, could offer a solution. Namely, alternate use of the dyes (ICG to fluorescein or fluorescein to ICG) enables us to perform videoangiography twice in a short time even via intravenous injection, since fluorescence of both dyes does not interfere with each other.
References
- 1). Kuroda K, Kinouchi H, Kanemaru K, Wakai T, Senbokuya N, Horikoshi T: Indocyanine green videoangiography to detect aneurysm and related vascular structures buried in subarachnoid clots. J Neurosurg 114: 1054– 1056, 2011. [DOI] [PubMed] [Google Scholar]
- 2). Raabe A, Nakaji P, Beck J, Kim LJ, Hsu FP, Kamerman JD, Seifert V, Spetzler RF: Prospective evaluation of surgical microscope-integrated intraoperative near-infrared indocyanine green videoangiography during aneurysm surgery. J Neurosurg 103: 982– 989, 2005. [DOI] [PubMed] [Google Scholar]
- 3). Suzuki K, Kodama N, Sasaki T, Matsumoto M, Ichikawa T, Munakata R, Muramatsu H, Kasuya H: Confirmation of blood flow in perforating arteries using fluorescein cerebral angiography during aneurysm surgery. J Neurosurg 107: 68– 73, 2007. [DOI] [PubMed] [Google Scholar]
- 4). Stanga PE, Lim JI, Hamilton P: Indocyanine green angiography in chorioretinal diseases: indications and interpretation: an evidence-based update. Ophthalmology 110: 15– 21; quiz 22–23, 2003. [DOI] [PubMed] [Google Scholar]
- 5). Woitzik J, Horn P, Vajkoczy P, Schmiedek P: Intraoperative control of extracranial-intracranial bypass patency by near-infrared indocyanine green videoangiography. J Neurosurg 102: 692– 698, 2005. [DOI] [PubMed] [Google Scholar]
- 6). Feindel W, Yamamoto YL: Cerebral microcirculation: studies by fluorescein angiography and local cerebral blood flow measurements by radioisotopes. Neurol Med Chir (Tokyo) 13: 21– 37, 1973. [DOI] [PubMed] [Google Scholar]
- 7). Feindel W, Yamamoto YL, Hodge CP: Intracarotid fluorescein angiography: a new method for examination of the epicerebral circulation in man. Can Med Assoc J 96: 1– 7, 1967. [PMC free article] [PubMed] [Google Scholar]
- 8). Hongo K, Kobayashi S, Okudera H, Hokama M, Nakagawa F: Noninvasive cerebral optical spectroscopy: depth-resolved measurements of cerebral haemodynamics using indocyanine green. Neurol Res 17: 89– 93, 1995. [DOI] [PubMed] [Google Scholar]
- 9). Suzuki K, Watanabe Y, Ichikawa T: [Usefulness of intraoperative fluorescence cerebral angiography using fluorescein sodium]. Surg Cereb Stroke 37: 240– 245, 2009. (Japanese) [Google Scholar]
- 10). Hope-Ross M, Yannuzzi LA, Gragoudas ES, Guyer DR, Slakter JS, Sorenson JA, Krupsky S, Orlock DA, Puliafito CA: Adverse reactions due to indocyanine green. Ophthalmology 101: 529– 533, 1994. [DOI] [PubMed] [Google Scholar]
- 11). Yannuzzi LA, Rohrer KT, Tindel LJ, Sobel RS, Costanza MA, Shields W, Zang E: Fluorescein angiography complication survey. Ophthalmology 93: 611– 617, 1986. [DOI] [PubMed] [Google Scholar]