

Abstract
Background:
Vitamin B12 deficiency is thought to be uncommon in the eastern parts of India including Bengal and the eastern states as compared to the northern and southern parts of India. The importance of cutaneous features in relation to vitamin B12 deficiency is not well described in literature.
Aim:
To know the clinical profile of vitamin B12 deficiency in this region and to find out if there is any relationship between dermatologic manifestations with vitamin B12 deficiency.
Materials and Methods:
All symptomatic patients of anemia requiring blood transfusions who had either raised mean corpuscular volume (MCV) or bicytopenia/pancytopenia on complete blood count or were symptomatic in the form of skin hyperpigmentation were screened for vitamin B12 deficiency.
Results:
Twenty-five patients were tested for vitamin B12 deficiency. Of them 19 patients were found to be having vitamin B12 deficiency.
Conclusions:
Vitamin B12 deficiency is not uncommon in the eastern parts of India, contrasting the previous thoughts that it was uncommon in this area, though larger studies are required to know it better. This study included only those requiring blood transfusions, thus a much higher prevalence is expected in this area. Patients with vitamin B12 deficiency do present with severe anemia requiring blood transfusions and often have skin hyperpigmentation.
Keywords: Hyperpigmentation, sub-Himalayan Bengal, Vitamin B12 deficiency
What was known?
Vitamin B12 deficiency is not very common in eastern part of India including Bengal. The relationship of dermatologic manifestations with overt vitamin B12 deficiency has not been adequately evaluated in literature.
Introduction
Vitamin B12 (cobalamin) deficiency has been a known clinical entity for long. Megaloblastic anemia results from abnormal maturation of hematopoietic cells due to faulty DNA synthesis. Two vitamins, cobalamin (vitamin B12) and folic acid are essential for DNA biosynthesis. Deficiency of either of these vitamins results in asynchrony in the maturation of the nucleus and cytoplasm of rapidly regenerating cells. In the hematopoietic system, this asynchrony results in abnormal nuclear maturation with normal cytoplasmic maturation, apoptosis, ineffective erythropoiesis, intramedullary haemolysis, pancytopenia and typical morphological abnormalities in the blood and marrow cells.[1,2] There is evidence that the disease is more common than was previously believed[3] but there are very little Indian data on this[4] especially from the eastern parts including Bengal and the eastern states. A recent Pubmed search with keywords of “vitamin B12 deficiency” or “pernicious anemia” and “India” did not reveal any study from this part of the country. However, there are vitamin B12 deficiency-related studies from other parts of India.[4,5,6]
Among the common causes of anemia in this area, the predominant forms are those having iron deficiency and congenital hemolytic anemia. Three consecutive cases of severe anemia requiring blood transfusions, who had florid cutaneous manifestations in the form of skin hyperpigmentation, were subsequently found to be vitamin B12 deficient and had put to our thoughts that vitamin B12 deficiency could be more common in this region than expected. This prompted us to carry out a study despite our limited set up. We did a prospective study between March 2013 and August 2013 to document the incidence of vitamin B12 deficiency with anemia in our hospital, document the clinical presentation and dietary practices in affected patients.
Cutaneous features of vitamin B12 deficiency are not well described in literature. The first description of hyperpigmentation in vitamin B12 deficiency was given by Dr. Bramwell Cook and this has been documented in subsequent case reports. Some of the described cutaneous manifestations are skin hyperpigmentation, vitiligo, angular stomatitis, and hair changes.[7] Hyperpigmentation of the extremities—especially over the dorsum of the hands and feet, with accentuation over the interphalangeal joints and terminal phalanges—associated with pigmentation of oral mucosa is a characteristic of vitamin B12 deficiency [Figures 1 and 2].[8,9,10] Interestingly, this hyperpigmentation is more common in dark-skinned patients.[7] The relationship of cutaneous features with degree of vitamin B12 deficiency is, however, not well studied.
Figure 1.

Photograph of hands showing hyperpigmentation
Figure 2.

Photograph of patient showing pigmentation of tongue and icterus
Materials and Methods
Study Design
Prospective, Observational
Study Period
March 2013 to August 2013
Patients
Total 25, Male 4 and Female 21.
The inclusion criteria for the study were symptomatic anemia patients requiring hospital admission with any one of the following
Raised MCV (>100 fl) on CBC
-
Bicytopenia or pancytopenia defined by the presence of two or more of the following
- Hemoglobin < 12 gm/dl for female subjects, <13 gm/dl for male subjects
- WBC count < 4000/mm3
- Platelet count < 150,000/mm3
Cutaneous manifestation defined by skin hyperpigmentation at the knuckles.
Following patients were excluded
Those who received blood transfusions within 1 month prior to presentation
Those already on vitamin B12 supplementations.
Study protocol
Detailed history regarding demography, clinical presentation with special reference to pallor, organomegaly, nervous system examination (tingling, numbness, parasthesia, Deep Tendan Reflexes, Sensory system etc), dietary habits, jaundice, history suggestive of malabsorptions, drug history, previous blood transfusions and family history were documented. Subjects were classified as non-vegetarians if they habitually consume at least one non-vegetarian meal per day for most of the days of the week. After informed consent, blood samples were drawn for hemoglobin, MCV, hypersegmented neutrophils, WBC count, platelet count, serum cobalamin, serum folic acid and bilirubin. Serum vitamin B12 and folate were measured in COBAS 6000 by electrochemiluminescence method and bilirubin was measured by photometry.
Statistical analysis
Values are expressed as mean ± SD for continuous variables. Clinical features like hyperpigmentation etc., were expressed as percentage. Comparison of vitamin B12 between groups was done using the Student t-test. Significance level was taken as 95%, P < 0.05.
Results
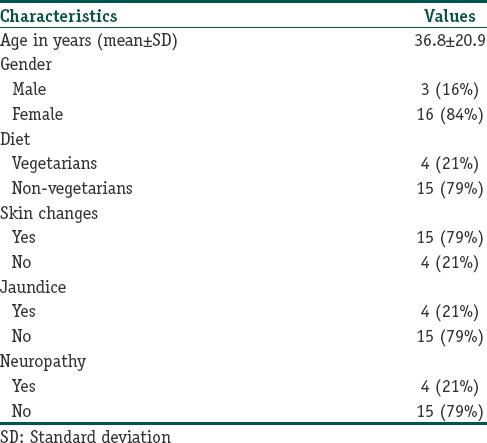
The majority of the patients were in their 30s. The youngest patient was 13 years old and the oldest patient was 72 years old. There was female predominance, with 84% of patients being female. As much as 79% of the patients were non-vegetarian. Hyperpigmentation of the knuckles was found in 79% of patients. Jaundice was present in 21% of the patients. Clinical evidence of neuropathy was present in 21% of patients. Demographic and clinical characteristics of the patients are shown in Table 1.
Table 1.
Demographic and clinical profile of B12 deficient patients’
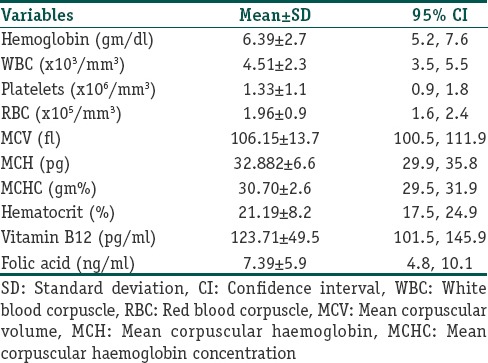
The mean hemoglobin was 6.39 ± 2.7 gm/dl. Mean WBC count was 4.51 ± 2.3 × 103 /mm3. Mean platelet count was 1.33 ± 1.1 × 106 /mm3. The mean MCV was 106.15 ± 13.7 fl. The mean serum vitamin B12 was 123.71 ± 49.5 pg/ml. Hematological profiles are shown in Table 2.
Table 2.
Hematological profile of patients with vitamin B12 deficiency
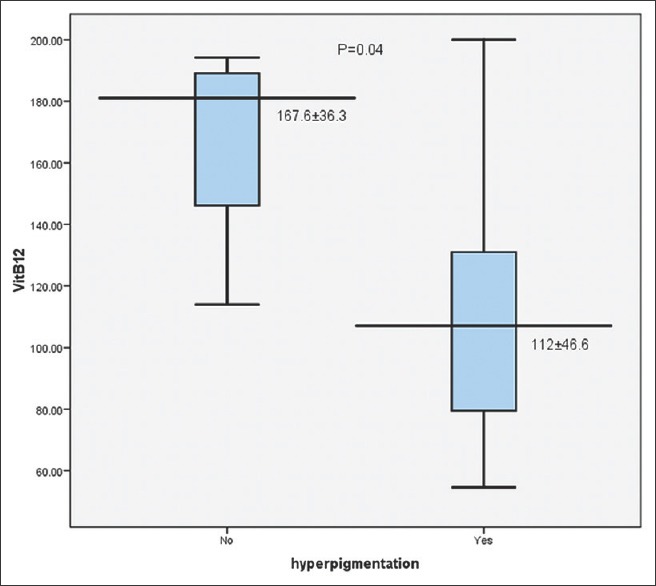
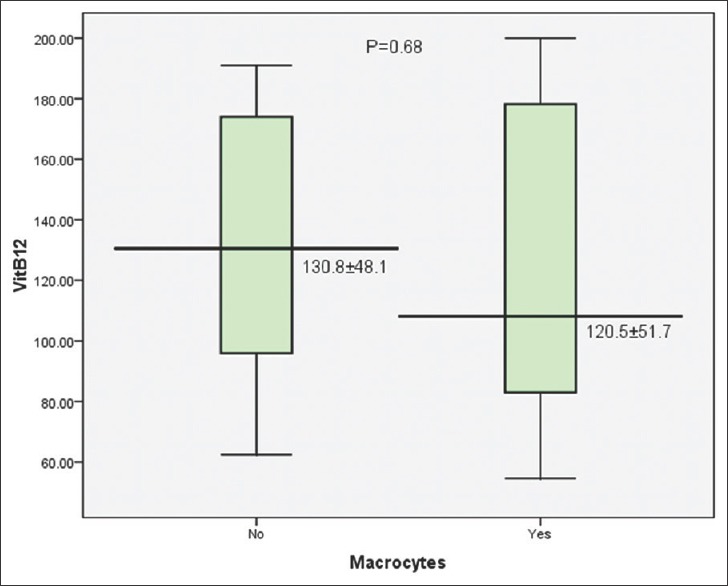
We analyzed if the presence of hyperpigmentation or the laboratory evidence of macrocytic anemia (MCV > 100 fl) is predictive of low serum vitamin B12 level. The mean vitamin B12 levels were 130.8 ± 48.1 and 120.5 ± 51.7 in patients with normal MCV and raised MCV, respectively [Figure 3]. This was not found to be statistically significant (P = 0.68). In contrast, the vitamin B12 levels in patients with hyperpigmentation were significantly lower than that in patients without hyperpigmentation (112 ± 46.6 versus 167.6 ± 36.3; P = 0.04) [Figure 4].
Figure 3.
Comparison of serum vitamin B12 levels between patients with and without macrocytes (MCV≥100 fl) on peripheral blood smear
Figure 4.
Comparison of serum vitamin B12 levels between patients with and without hyperpigmentation
Discussions
Vitamin B12 deficiency causes a range of disorders and affects all age groups. The main systems affected in vitamin B12 deficiency are the hematologic, gastrointestinal, and nervous systems.[11] Other manifestations involve the cardiovascular system, skeletal system and skin and hair changes.[12] This study noted in particular the cutaneous changes, above other profiles, as it was a very consistent finding.
The average Indian vegetarian diet is deficient in cobalamin[13,14] and this must be noted when considering the results of the earlier studies from north and south India because of the large vegetarian diet population. On the contrary, this hospital is catering a population from North Bengal, Assam and other north eastern states where there is a predominant non-vegetarian diet. The cause of vitamin B12 deficiency in this part of the country may thus not be diet related.
Interestingly, vitamin B12 deficiency was found to be more common than was expected. Raised MCV (>100 fl) was found in 79% of patients. A previous study has shown that the sensitivity of high MCV was 30% for low serum vitamin B12 concentration, 58% for deficiency, and 75% for deficiency in patients with anemia.[15] Pancytopenia was found in 42% and bicytopenia in 26% thus highlighting vitamin B12 deficiency as an important cause of multiple cell line deficiency.
An important clinical presentation found in this study was hyperpigmentation of the extremities, particularly of the knuckles, found in 79%. This is a relatively consistent finding so that the index of suspicion rises significantly in those patients with knuckle hyperpigmentation. Jaundice and neurological involvement were rather uncommon, both found in only 21% even at very low serum vitamin B12 levels.
Determining the cause of vitamin B12 deficiency was not possible due to logistic constraints. Vitamin B12 deficiency commonly occur in vegetarians as the important source of vitamin B12 are animal products.[16] It was surprising that 79% of affected patients had non-vegetarian diet, thus making us more keen to know what might be the cause of vitamin B12 deficiency in this part of the country. The authors do however admit that the dietary assessment was a limited one considering the difficulty in measuring the nutritional value of Indian diet and the heterogeneity of population. Further well-designed, larger epidemiologic studies are required to confirm the increased prevalence of vitamin B12 deficiency in this region. Thus, it may be considered only as a pilot study as this part of the country has lack of literature regarding vitamin B12 deficiency, and the importance of skin manifestations as a clinical pointer to symptomatic vitamin B12 deficiency. In a recent study from southern India, hyperpigmentation has been observed to be an early and consistent feature of vitamin B12 deficiency.[17]
Thus, this study has demonstrated the occurrence of symptomatic vitamin B12 deficiency in this part of the country and has highlighted the importance of mucocutaneous manifestations as a clinical marker in such patients. However, large-scale population-based studies are required to validate our findings.
What is new?
Symptomatic vitamin B12 deficiency is not uncommon in eastern India including Bengal and constitutes an important cause of severe anemia here. Dermatologic manifestations especially hyperpigmentation of the knuckles can serve as important clinical clue to diagnose overt vitamin B12-deficient patients.
Footnotes
Source of support: Nil
Conflict of Interest: Nil.
References
- 1.Antony AC. Hematology. Basic principles and practice. In: Hoffman R, Benz EJ, Shattil SJ, Furie B, Cohen HJ, Silberstein LE, editors. 4th ed. Edinburgh: Churchill Livingstone; 2005. pp. 519–56. [Google Scholar]
- 2.Carmel R. Megaloblastic anemias: Disorders of impaired DNA synthesis. In: Greer JP, Foerster J, Lukens JN, Rodgers GM, Paraskevas F, Glader B, editors. Wintrobe's clinical hematology. 11th ed. Philadelphia: Lippincott Williams and Wilkins; 2004. pp. 1367–95. [Google Scholar]
- 3.Carmel R. Efficacy and safety of fortification and supplementation with vitamin B12: Biochemical and physiological effects. Food Nutr Bull. 2008;29(2 Suppl):S177–87. doi: 10.1177/15648265080292S121. [DOI] [PubMed] [Google Scholar]
- 4.Bhatia P, Kulkarni JD, Pai SA. Vitamin B12 deficiency in India: Mean corpuscular volume is an unreliable screening parameter. Natl Med J India. 2012;25:336–8. [PubMed] [Google Scholar]
- 5.Premkumar M, Gupta N, Singh T, Velpandian T. Cobalamin and folic acid status in relation to the etiopathogenesis of pancytopenia in adults in a tertiary care centre in North India. Anemia. 2012;2012:707402. doi: 10.1155/2012/707402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Khanduri U, Sharma A. Megaloblastic anemia: Prevalence and causative factors. Natl Med J India. 2007;20:172–5. [PubMed] [Google Scholar]
- 7.Kannan R, Ng MJ. Cutaneous lesions and vitamin B12 deficiency: An often-forgotten link. Can Fam Physician. 2008;54:529–32. [PMC free article] [PubMed] [Google Scholar]
- 8.Aaron S, Kumar S, Vijayan J, Jacob J, Alexander M, Gnanamuthu C. Clinical and laboratory features and response to treatment in patients presenting with vitamin B12 deficiency–related neurological syndromes. Neurol India. 2005;53:55–8. doi: 10.4103/0028-3886.15057. [DOI] [PubMed] [Google Scholar]
- 9.Baker SJ, Ignatius M, Johnson S, Vaish SK. Pigmentation and vitamin B12 deficiency. Br Med J. 1963;2:1205. doi: 10.1136/bmj.2.5366.1205-b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Baker SJ, Ignatius M, Johnson S, Vaish SK. Hyperpigmentation of skin. A sign of vitamin-B12 deficiency. Br Med J. 1963;1:1713–5. doi: 10.1136/bmj.1.5347.1713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Oh RC, Brown DL. Vitamin B12 deficiency. Am Fam Physician. 2003;67:979–86. [PubMed] [Google Scholar]
- 12.Dr Siew Chee Weng. A systematic review of vitamin B12 deficiency. Singapore Family Physician. 2008;34:51–7. [Google Scholar]
- 13.Antony AC. Vegetarianism and vitamin B-12 (cobalamin) deficiency. Am J Clin Nutr. 2003;78:3–6. doi: 10.1093/ajcn/78.1.3. [DOI] [PubMed] [Google Scholar]
- 14.Antony AC. Prevalence of cobalamin (vitamin B12) and folate deficiency in India- audi altera partem. Am J Clin Nutr. 2001;74:157–9. doi: 10.1093/ajcn/74.2.157. [DOI] [PubMed] [Google Scholar]
- 15.Oosterhuis WP, Niessen RW, Bossuyt PM, Sanders GT, Sturk A. Diagnostic value of the mean corpuscular volume in the detection of vitamin B12 deficiency. Scand J Clin Lab Invest. 2000;60:9–18. doi: 10.1080/00365510050184994. [DOI] [PubMed] [Google Scholar]
- 16.Herrmann W, Obeid R. Causes and early diagnosis of vitamin B12 deficiency. Dtsch Arztebl Int. 2008;105:680–5. doi: 10.3238/arztebl.2008.0680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Jithendriya M, Kumaran S. P IB. Addisonian pigmentation and Vitamin B12 deficiency: A case series and review of the literature. Cutis. 2013;92:94–9. [PubMed] [Google Scholar]