

Description
An 86-year-old man, a healthcare worker (HCW), was screened at the Occupational Health and Safety Centre, Mumbai, which has helped diagnose and compensate hundreds of cases of asbestosis among former employees and spouses of the Indian subsidiaries of T&N Limited, UK.1 The patient had dyspnoea grade III, clubbing of nails and auscultation revealed bilateral crepitations on deep inspiration. There were no other relevant signs. Lung function tests showed that forced vital capacity and forced expiratory volume in 1 s were less than 60% of the predicted values. A chest X-ray posterioranterior view showed evidence of parenchymal (International Labour Organisation (ILO) grading t/t; 2/1) and pleural (bilateral lower zone pleural calcifications in profile) asbestosis: (figure 1). He was compensated for his disease by the T&N trust.
Figure 1.
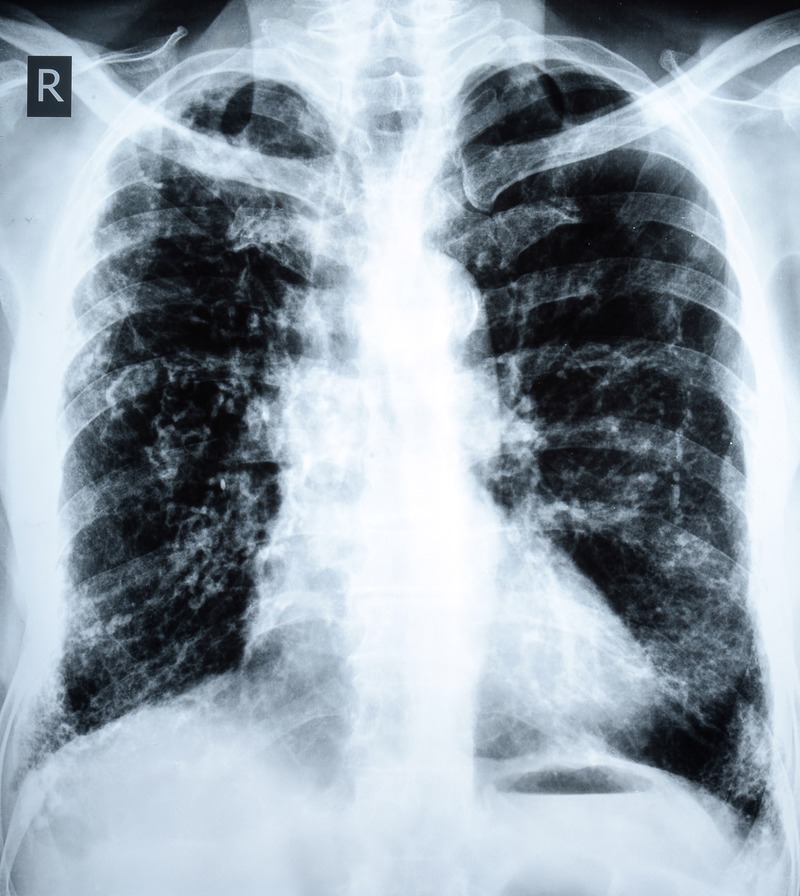
A posterioranterior view chest X-ray shows evidence of both parenchymal (ILO grading t/t; 2/1) and pleural (bilateral lower zone pleural calcifications in profile) asbestosis.
He had worked at a clinic that was situated outside the compound of the factory, initially as a sweeper, and then as a dresser, for 36 years. As the workers came to the clinic in their factory clothes and unshowered, the patient was exposed to asbestos dust from the workers’ clothes and hair. Contaminated workers’ clothes are a risk factor for the development of asbestosis.2 It is, rarely, reported that HCWs can develop industrial diseases if they work in the vicinity of an industry. These diseases are not listed among the traditional occupational diseases of HCWs.3 Occupationally acquired asbestosis among HCWs has not been reported. Detailed exposure history of HCWs who work in an industrial setting is necessary to be able to diagnose occupational diseases peculiar to that industry.
Learning points.
Asbestosis can develop due to secondary exposure among healthcare workers who work in an occupational health clinic of an asbestos manufacturing factory.
Detailed exposure history of healthcare workers who are exposed to industrial hazards is necessary to be able to diagnose occupational diseases that are peculiar to that industry.
Footnotes
Contributors: VM examined the case, diagnosed the patient based on clinical signs and investigations and wrote the manuscript.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Murlidhar V, Kanhere V. Asbestosis in an asbestos composite mill at Mumbai: a prevalence study. Environ Health 2005;4:24 doi:10.1186/1476-069X-4-24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rosell-Murphy MI, Abos-Herrandiz R, Olivella JT et al. Risk factors associated with asbestos-related diseases: a community-based case-control study. BMC Public Health 2013;13:723 doi:10.1186/1471-2458-13-723 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Centers for disease control and prevention, CDC, Atlanta, USA. Health care workers. http://www.cdc.gov/niosh/topics/healthcare/ (accessed 15 Jun 2015).