

Abstract
Introduction:
It is unknown whether Saudis receive health examinations periodically. To inform health authorities on the health-seeking behavior of the Saudi population, we investigated patterns of periodic health examination (PHE) use by Saudis.
Materials and Methods:
We conducted a nationally representative multistage survey of individuals aged 15 years or older on sociodemographic characteristics, healthcare utilization, and self-reported chronic conditions. We used a backward elimination multivariate logistic regression model to measure associations between PHE and sociodemographic, behavioral, and health characteristics.
Results:
Between April and June 2013, a total of 12,000 households were contacted, and 10,735 participants completed the survey (response rate of 89.4%). Among participants, 2542 (22.9%), representing more than 2.7 million Saudis aged 15 years or older, received a PHE during the past 2 years. Moreover, 7463 (73.5%) participants, representing 9.1 million Saudis, visited a healthcare setting in the past 2 years due to illness or injury. The likelihood of receiving a PHE in the past 2 years increased with age, education, being married, consumption of five servings of fruits and vegetables per day, diagnoses of prediabetes, diabetes, or hypercholesterolemia, and a visit to a healthcare setting within the last 2 years due to an illness or an injury.
Discussion:
This is the first national study to investigate the use of PHE in Kingdom of Saudi Arabia (KSA) where healthcare is freely available. Few Saudis seek preventive healthcare and most healthcare visits are for injuries or sickness. KSA may reduce its health expenditures by routinizing PHE and detecting chronic conditions at early stages.
Keywords: Periodic health examination, prevention, primary care, Saudi Arabia, screening
Introduction
Periodic health examinations (PHE) are a group of tasks designed either to determine the risk of subsequent disease or identify disease in its early, symptomless state.[1,2] In the Kingdom of Saudi Arabia (KSA) free healthcare is offered to Saudi citizens.[3,4] However, Saudi still face major preventable health challenges.[5,6,7] Health-seeking behavior among Saudis has not been documented. Such information is crucial to plan outreach and health-promotion activities by concerned stakeholders. To inform health authorities on the health-seeking behavior of the Saudi population, we investigated PHE and reasons for using healthcare services through a national household survey.
Materials and Methods
Ethics statement
The Saudi Ministry of Health and its Institutional Review Board (IRB) have approved the study protocol. The University of Washington IRB has deemed the study as IRB exempt since The Institute for Health Metrics and Evaluation received de-identified data for these analyses. All respondents consented and agreed to participate in this study. We used verbal consent that was captured by our computer program since it is commonly used and accepted in KSA. Two verbal consents were obtained: One for the household roster (obtained from the head of the household or the most knowledgeable person in the house) and another obtained from the randomly selected respondent. If the randomly selected respondent was between the ages of 15–17 years old, then the parent(s) or legal guardian of that individual consented on their behalf to participate in the study. The KSA Ministry of Health and the University of Washington IRB approved the verbal consents that were obtained in this study, as this is an accepted norm in KSA.
The Saudi Health Interview Survey is a national multistage survey of individuals aged 15 years or older. Households of Saudi citizens were randomly selected from a national sampling frame maintained and updated by the Census Bureau. The Ministry of Health divides KSA into 13 health regions, each with its own health department. We divided each region into sub-regions and blocks used by the KSA Department of Statistics. All regions were included, and a probability proportional to size was used to select randomly sub-regions and blocks. Households were randomly selected from each block. A roster of household members was collected, and an adult aged 15 or older was randomly selected to be surveyed. If the randomly selected adult was not present, our surveyors made an appointment to return, and a total of three visits were made before the household was considered as a nonresponse. Weight, height, and blood pressure of the randomly selected adult were measured at the household by a trained professional.
The survey included questions on sociodemographic characteristics, tobacco consumption, diet, physical activity, healthcare utilization, different health-related behaviors, and self-reported chronic conditions. These conditions included prediabetes, diabetes, hypercholesterolemia and hypertension.
To assess self-rated health, respondents were asked, “In general, would you say your health is excellent, very good, good, fair, or poor?”
To measure diagnosed blood pressure, diabetes, and hypercholesterolemia status, respondents were asked three separate questions: “Have you ever been told by a doctor, nurse, or other health professional that you had: (1) Prediabetes Mellitus, otherwise known as prediabetes, borderline diabetes, impaired fasting glucose, impaired glucose tolerance, or impaired sugar tolerance; (2) diabetes mellitus, otherwise known as diabetes, sugar diabetes, high blood glucose, or high blood sugar; (3) hypercholesterolemia, otherwise known as high or abnormal blood cholesterol; (4) hypertension, otherwise known as high blood pressure?” Women diagnosed with diabetes or hypertension during pregnancy were not counted as having these conditions. Similarly, the same types of questions were used to determine previous diagnosis of stroke, myocardial infarction, atrial fibrillation, cardiac arrest, congestive heart failure, chronic obstructive pulmonary disease, asthma, renal failure, and cancer. We considered a person to be diagnosed with a chronic condition if they reported being diagnosed with any of these conditions.
To assess use of healthcare services, participants were asked, “In what year did you last visit: (1) A hospital, (2) a clinic, (3) a doctor for medical attention for any reason?” Those who provided an answer were then asked, “What was the reason for your last visit to: (1) A hospital, (2) a clinic, (3) a doctor?” Respondents could choose between “illness,” “injury,” “vaccination,” and “other preventive services.”
To calculate the time since last PHE, participants were asked, “In what year did you last visit a doctor or other health professional for a routine checkup? A routine checkup is a general physical exam, not an exam for a specific injury, illness, or condition.”
Statistical analysis
We used a backward elimination multivariate logistic regression model to measure association between having received a PHE within the last 2 years and sex, age, marital status, education, self-rated health, use of healthcare services, and history of diagnosis with prediabetes, diabetes, hypercholesterolemia, hypertension, and other chronic conditions. Data were weighted to account for the probability of selection, and age and sex poststratification based on census data for age and sex distribution of the Saudi population. We used SAS 9.3 [SAS Institute. Inc., Cary, North Carolina, USA] for the analyses. The SAS procedures SURVEYFREQ and SURVEYLOGISTIC were used to provide the un-weighted frequencies, the weighted percentages and estimates at the population level, and the adjusted odds ratios (AOR) and their 95% confidence intervals (95% CI). These procedures account for the survey weights and complex design.
Results
Between April and June 2013, a total of 12,000 households were contacted, and 10,735 participants completed the survey (response rate of 89.4%). The characteristics of respondents who completed the questionnaire are presented in Table 1.
Table 1.
Sociodemographic characteristics, Saudi Health Interview Survey, 2013
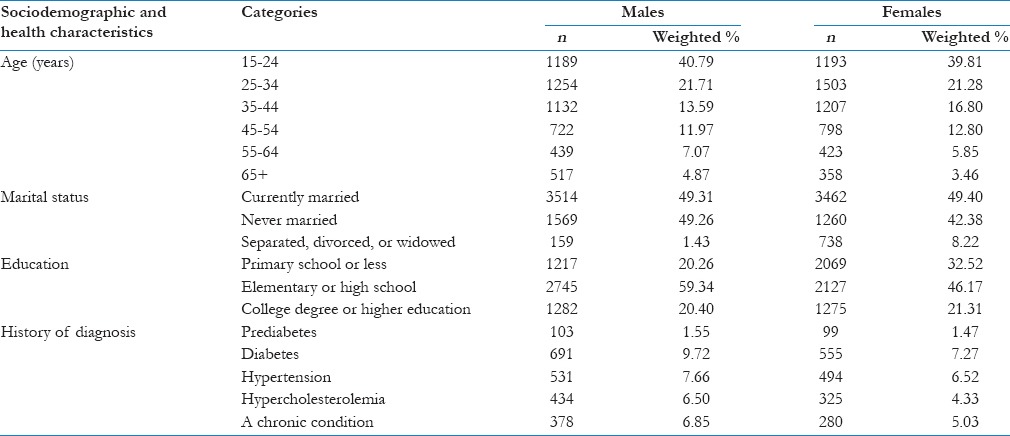
Among participants, 2542 (weighted percent: 22.9), representing more than 2.7 million Saudis aged 15 years or older, received a PHE during the past 2 years. Moreover, 7,463 (weighted percent: 73.5%), representing 9.1 million Saudis aged 15 years or older, visited a healthcare setting in the past 2 years due to illness or injury. Of these, 25.8% also reported receiving a PHE.
Among Saudis aged 15 years or older, 1.5%, 8.5%, 5.4%, 7.1%, and 6.0% reported being diagnosed with prediabetes, diabetes, hypercholesterolemia, hypertension, and other chronic conditions, respectively.
The likelihood of receiving a PHE in the past 2 years increased with age (AOR = 1.2; 95% CI: 1.1–1.3); among those with elementary or high school education (AOR = 1.4; 95% CI: 1.1–1.7), or college degree or higher (AOR = 1.7; 95% CI: 1.3–2.0); currently (AOR = 1.7; 95% CI: 1.3–2.1) and previously married (AOR = 1.5; 95% CI: 1.1–2.1); those who consumed five servings of fruits and vegetables per day (AOR = 2.1; 95% CI: 1.3–3.4); those diagnosed with prediabetes (AOR = 1.8; 95% CI: 1.0–3.0), diabetes (AOR = 1.4; 95% CI: 1.1–1.8), or hypercholesterolemia (AOR = 2.3; 95% CI: 1.8–3.0); and those who visited a health care setting within 2 years from the survey time due to an illness or an injury (AOR = 1.8; 95% CI: 1.5–2.2), compared to the younger; less educated; single; those who consumed no fruits and vegetables on a daily basis, those who have no diagnoses of prediabetes, diabetes, or hypercholesterolemia; and those who have never been to a healthcare setting, or have been but prior to 2 years from the survey time, or have been within 2 years from the survey time but for vaccinations or other preventive services [Table 2].
Table 2.
Sociodemographic, behavioral, and health characteristics associated with receipt of a periodic health examination within the last 2 years, Kingdom of Saudi Arabia, 2013
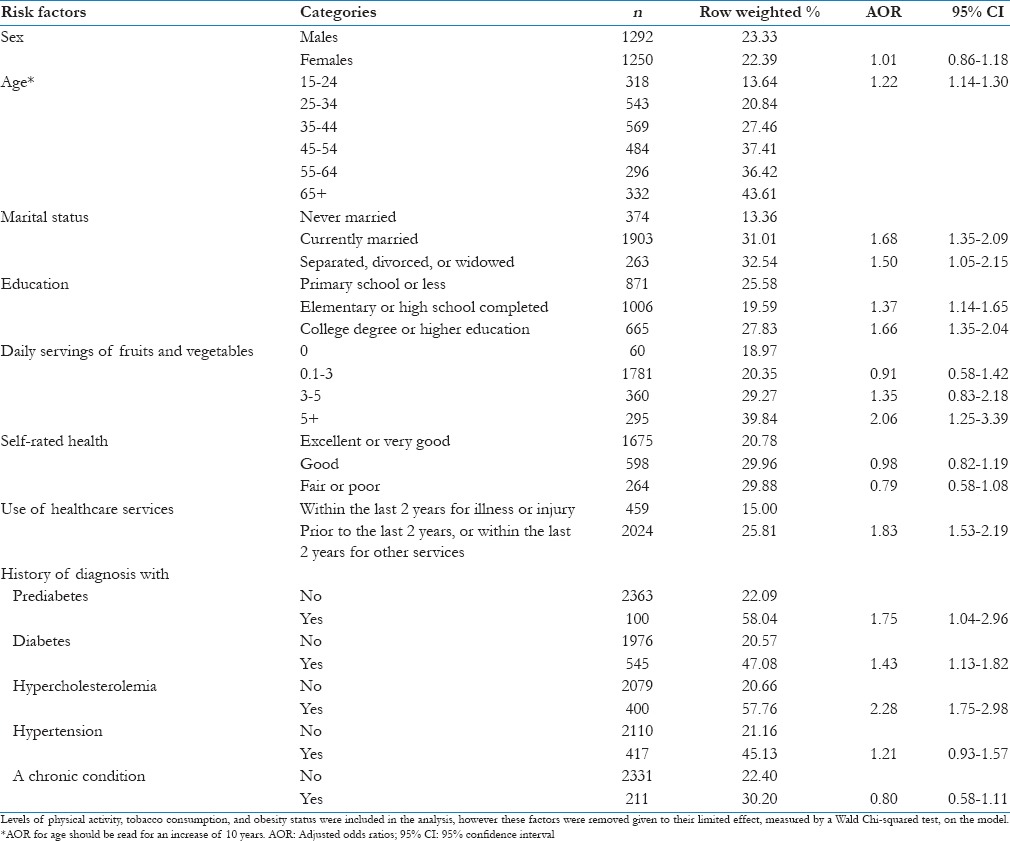
We repeated the same analysis after combining all diagnoses of chronic conditions. The results had the same patterns as for the likelihood of receiving a PHE within 2 years from the survey time. Specifically, those diagnosed with any condition (prediabetes, diabetes, hypercholesterolemia, hypertension, or other chronic conditions) were almost twice as likely (AOR = 1.7; 95% CI: 1.5–2.1) to have received a PHE within 2 years of the survey time, compared to those who have no such diagnosis.
Discussion
This is the first national study to investigate healthcare-seeking behavior in KSA, a country where healthcare is available for free. Our findings show that few Saudis seek preventive healthcare, and most visits are for injuries or sickness. Our findings are alarming, as Saudis have high rates of diagnosed and undiagnosed chronic diseases. Indeed, preventive services are urgently needed to curb the burden of chronic diseases in the Kingdom. Our findings of the elderly seeking more healthcare services are due to increased comorbidities with age.[8] Interestingly, men, who are generally known to seek healthcare less than women,[9] did not differ in their receipt of a PHE. However, men are also known to be influenced by women in their healthcare-seeking behavior,[10] which could explain why married men are more likely to seek healthcare than unmarried ones.
Our findings on increased PHE with education are not surprising. Indeed, educated individuals are more likely to understand the importance of preventive services and take action to protect their health before they face sickness. In his health-promotion model, Nutbeam places education at the basis of the chain leading to health outcomes.[11] It is a major factor to influence individual health literacy, which “represents the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways that promote and maintain good health.”[12] Unfortunately, health education has been reported to be poor in KSA,[12] and the MOH needs to focus its efforts in this domain to empower Saudis in improving their health.
We have previously reported on the high prevalence of preventable chronic diseases such as hypertension, diabetes, and hypercholesterolemia in KSA.[5,6,7] We mostly pointed out the high number of affected individuals who are undiagnosed, or unaware of their conditions. It is mostly this group that might progress toward sudden adverse health events that require intensive treatment, at a higher cost than the usual disease progression. PHEs allow individuals to be aware of their health status, take the right measures, and get the appropriate care. For instance, we have previously shown how Saudis who had been diagnosed with prediabetes managed to control their hemoglobin A1c) blood levels better than those who were not. However, and despite the higher uptake of PHE with age, the risk of being undiagnosed with hypertension, diabetes, or hypercholesterolemia increased with age, while those who are diagnosed tend to seek a routine medical visit more often than the others. This finding indicates that Saudis start seeking healthcare only when they have developed a disease, instead of routinely checking their health to detect early signs of health problems and prevent their progression.
The reasons why people avoid healthcare until it is needed are not a total mystery. Healthcare services, specifically those that are physically invasive, such as venipuncture, are known to generate acute stress among recipients.[13] Often, fear of disease pushes people to seek more screening but fear surrounding screening procedures prohibits them from seeking screening when no symptoms are apparent.[14,15]
Our previous finding that older individuals are more likely to be undiagnosed with the three chronic conditions despite their greater attempts to receive a PHE indicates missed opportunities in the health system.[5,6,7] Since the 1970s, the Canadian task force on the PHE and the US Taskforce for preventive services, as well as the American Academy of Family Physicians[16] have updated their guidelines to tailor PHE toward age- and sex-specific examinations. Perhaps the Saudi healthcare system should develop and implement such guidelines to increase preventive care services in the Kingdom. The Saudi Ministry of Health can provide primary care physicians with a memory aid of evidence-based practices for PHE, such as a list of examinations to conduct based on patients’ age and sex. Health information on the Saudi population, next to guidelines that have been rigorously evaluated, can be used to tailor this memory aid to the needs of primary healthcare in KSA.[17] Such a strategy would be welcomed by primary healthcare providers in KSA, as the vast majority of them believe that evidence-based practices can improve care.[18]
Our study has some limitations. First, our data are cross-sectional, and hence we cannot assess causality. Second, many of our behavioral data, such as diet and physical activity, are self-reported and subject to recall and social desirability biases. On the other hand, our study is based on a large sample size and used a standardized methodology for all its measures.
Despite these limitations, our study remains nationally representative and has the merit of providing accurate data due to our near-real-time data-quality monitoring through the whole survey period.
In 2013, the KSA spent $18.9 billion on health services and social development, the fourth-largest share of sector-wise state budget allocations.[4] Given our results on the high numbers of people with chronic disease, we assume that the majority of these expenditures are for treatment and care. For instance, a diabetic Saudi individual costs 10 times more in healthcare than a nondiabetic.[19] KSA can reduce its health expenditures by increasing its prevention efforts and detecting chronic conditions at early stages when simple lifestyle changes can be enough to stop the progression of the disease. Routinizing PHEs through the Saudi healthcare system and making them age and sex-specific can help reach these goals.
Acknowledgments
This study was financially supported by a grant from the Ministry of Health of the Kingdom of Saudi Arabia. We would like to acknowledge Adrienne Chew at the Institute for Health Metrics and Evaluation for editing this manuscript.
Footnotes
Source of Support: This study was financially supported by a grant from the Ministry of Health of the Kingdom of Saudi Arabia.
Conflict of Interest: The salaries of the authors from the Institute for Health Metrics and Evaluation (IHME) were fully or partially paid through a grant from the Ministry of Health (MOH) of the Kingdom of Saudi Arabia. The MOH managed the data collection for this study.
References
- 1.The periodic health examination. Canadian task force on the periodic health examination. Can Med Assoc J. 1979;121:1193–254. [PMC free article] [PubMed] [Google Scholar]
- 2.Si S, Moss JR, Sullivan TR, Newton SS, Stocks NP. Effectiveness of general practice-based health checks: A systematic review and meta-analysis. Br J Gen Pract. 2014;64:e47–53. doi: 10.3399/bjgp14X676456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Almalki M, Fitzgerald G, Clark M. Health care system in Saudi Arabia: An overview. East Mediterr Health J. 2011;17:784–93. doi: 10.26719/2011.17.10.784. [DOI] [PubMed] [Google Scholar]
- 4.Saudi Arabian Monetary Agency: Fourty Ninth Annual Report: Latest Economic Developments. [Last cited on 2014 Oct 24]. Available from: http://www.sama.gov.sa/sites/samaen/ReportsStatistics/ReportsStatisticsLib/5600_R_Annual_En_49_Apx.pdf .
- 5.El Bcheraoui C, Memish ZA, Tuffaha M, Daoud F, Robinson M, Jaber S, et al. Hypertension and its associated risk factors in the Kingdom of Saudi Arabia, 2013: A national survey. Int J Hypertens 2014. 2014 doi: 10.1155/2014/564679. 564679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.El Bcheraoui C, Basulaiman M, Tuffaha M, Daoud F, Robinson M, Jaber S, et al. Status of the diabetes epidemic in the Kingdom of Saudi Arabia, 2013. Int J Public Health. 2014;59:1011–21. doi: 10.1007/s00038-014-0612-4. [DOI] [PubMed] [Google Scholar]
- 7.Basulaiman M, El Bcheraoui C, Tuffaha M, Robinson M, Daoud F, Jaber S, et al. Hypercholesterolemia and its associated risk factors-Kingdom of Saudi Arabia, 2013. Ann Epidemiol. 2014;24:801–8. doi: 10.1016/j.annepidem.2014.08.001. [DOI] [PubMed] [Google Scholar]
- 8.Bausell RB. Health-seeking behavior among the elderly. Gerontologist. 1986;26:556–9. doi: 10.1093/geront/26.5.556. [DOI] [PubMed] [Google Scholar]
- 9.Tudiver F, Talbot Y. Why don’t men seek help? Family physicians’ perspectives on help-seeking behavior in men. J Fam Pract. 1999;48:47–52. [PubMed] [Google Scholar]
- 10.Norcross WA, Ramirez C, Palinkas LA. The influence of women on the health care-seeking behavior of men. J Fam Pract. 1996;43:475–80. [PubMed] [Google Scholar]
- 11.Nutbeam D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. 2000;15:259–67. [Google Scholar]
- 12.World Health Organization. Health Promotion Glossary. [Last cited on 2014 Oct 24]. Available from: http://www.who.int/healthpromotion/about/HPR%20Glossary%201998.pdf .
- 13.Koh D, Ng V, Naing L. Alpha amylase as a salivary biomarker of acute stress of venepuncture from periodic medical examinations. Front Public Health. 2014;2:121. doi: 10.3389/fpubh.2014.00121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Consedine NS, Adjei BA, Horton D, Joe AK, Borrell LN, Ramirez PM, et al. Fear and loathing in the Caribbean: Three studies of fear and cancer screening in Brooklyn's immigrant Caribbean subpopulations. Infect Agent Cancer. 2009;4(Suppl 1):S14. doi: 10.1186/1750-9378-4-S1-S14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Consedine NS, Adjei BA, Ramirez PM, McKiernan JM. An object lesson: Source determines the relations that trait anxiety, prostate cancer worry, and screening fear hold with prostate screening frequency. Cancer Epidemiol Biomarkers Prev. 2008;17:1631–9. doi: 10.1158/1055-9965.EPI-07-2538. [DOI] [PubMed] [Google Scholar]
- 16.American Family Physician. Introduction to AAFP Summary of Recoommendations for Periodic Health Examinations. [Last cited on 2014 Oct 24]. Available from: http://www.aafp.org/afp/2002/0401/p1467.html . [PubMed]
- 17.Milone SD, Milone SL. Evidence-based periodic health examination of adults. Memory aid for primary care physicians. Can Fam Physician. 2006;52:40–7. [PMC free article] [PubMed] [Google Scholar]
- 18.Al-Ansary LA, Khoja TA. The place of evidence-based medicine among primary health care physicians in Riyadh region, Saudi Arabia. Fam Pract. 2002;19:537–42. doi: 10.1093/fampra/19.5.537. [DOI] [PubMed] [Google Scholar]
- 19.Alhowaish AK. Economic costs of diabetes in Saudi Arabia. J Family Community Med. 2013;20:1–7. doi: 10.4103/2230-8229.108174. [DOI] [PMC free article] [PubMed] [Google Scholar]