

Abstract
Background:
Abdominal pain is one of the most common reasons for presenting to the emergency depatment (ED) and the etiology is varied.
Materials and Methods:
This prospective observational study was conducted in a large ED of a tertiary care center in India. All patients older than 15 years and presenting with non-traumatic abdominal pain to the ED from May 2012 to October 2012 were recruited and the demographic characteristics, diagnosis and outcome were analyzed.
Results:
The study cohort included 264 patients over a 6 month period. More than half (55.6%) were aged between 15 and 40 years. There was a male predominance (56.8%). Majority of the patients (76.9%) presented with abdominal pain of less than 72 hour duration. The pain was sudden in onset in 54.9% of patients. Dull type was the most common character of pain (36%) followed by colicky type (22.3%). The most common site of pain was the lower abdomen (45.8%). Upper abdominal pain was seen in 26.9% and the pain was generalized in 27.3% of patients. The common causes were uretericcolic (16.3%), urinary tract infection (12.5%), acute pancreatitis (11%), acute appendicitis (10.6%) and acute gastritis (8%). More than half (51.9%) discharged from ED and 37% of cases were managed by the emergency physicians. Surgical intervention was required in 25.8% of patients. The mortality rate was 2.3%.
Conclusions:
Abdominal pain is a common ED symptom and clinicians must consider multiple diagnoses, especially those that require immediate intervention to limit morbidity and mortality.
Keywords: Acute abdominal pain, emergency department, non-traumatic causes of abdominal pain
Introduction
Abdominal pain is one of the most common reasons for an emergency department (ED) visit, accounting to about 5% to 10% of all ED visits.[1] It poses a diagnostic challenge for the emergency physicians as the causes are numerous, ranging from benign to life-threatening conditions. Causes include gastro-intestinal, urological, and gynecological among others.[2] Despite extensive evaluation, a quarter of patients usually remained with a non-specific cause but now with latest radiological imaging advances that number has decreased.[3] The elderly patients have atypical presentations with longer duration of pain at presentation.[4] Associated features like vomiting, guarding, tachycardia were of diagnostic value while other features were not very useful.[5] Our study aims at studying the profile of non-traumatic acute abdominal pain in adult patients presenting to the ED of a tertiary hospital in south India.
Materials and Methods
This prospective observational study was conducted in a 56-bedded ED of Christian Medical College, Vellore, India between May and October 2012. The cut-off age for patients presenting to our ED (adult ED) is 15 years. Therefore, all patients above the age of 15 years who presented with abdominal pain were included in the study. As the age for consent in India is 18 years, an official consent was taken from the parent/guardian for those aged between 15 and 17 years. This study was approved by the Institutional Review Board of Christian Medical College, Vellore, and The Institutional ethics committee. Patient confidentiality was maintained using unique identifiers.
Patients with traumatic causes of abdominal pain were excluded. A detailed history on the onset, duration and type of pain and results of a thorough physical examination were entered on a standard data collection sheet after obtaining a written informed consent. Basic blood investigations were done for all patients. Radiological investigations like ultrasonography, computed tomography san and magnetic resonance imaging were done when indicated. Wong-Baker Faces Pain Rating Scale (WBF) was used to assess the severity of pain. The WBF scale uses a series of six faces with each describing an expression ranging from happy face, i.e., “no hurt”(score zero), to a crying face “hurts the worst” (score ten). The patients were asked to point out on the scale describing the severity of their pain. Pain relief was given through the oral route if mild or parenterally when severe. The patients were followed up till discharge from ED/admitted ward and the final diagnosis at discharge was noted.
Statistical methods
Statistical analysis was performed using SPSS software for Windows version 16.0. Descriptive data are given as a percentage.
Results
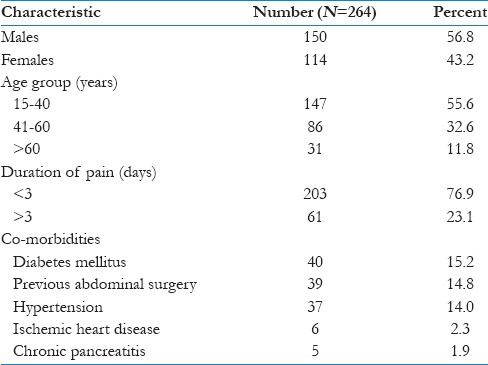
A total of 264 patients were included in the study. More than half (55.6%) were in the age group of 15–40 years. There was a slight male predominance (56.8%). Co-morbid conditions of diabetes mellitus, hypertension, ischemic heart disease and chronic pancreatitis were present in15.2%, 14.8%, 2.3% and 1.9% of patients, respectively. About 15% of patients had a past history of abdominal surgery [Table 1].
Table 1.
Patients baseline characteristics
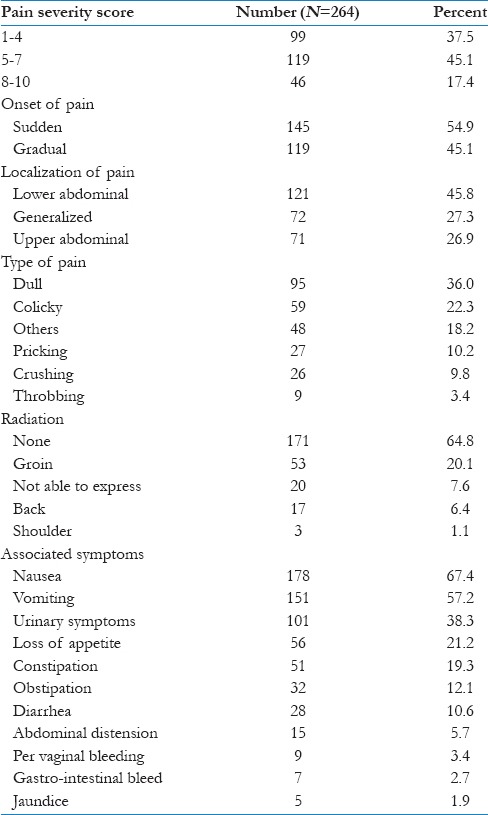
The pain was sudden in onset in 54.9% of patients. WBF scale was used to grade the severity of pain. WBF scale score of 1-4, 5–7 and 8–10 was seen in 37.5%, 45.1%and 17.4% of patients, respectively. Common types of pain included dull aching (36%), colicky (18.2%), pricking (10.2%), crushing (9.8%), and throbbing (3.4%). Eighteen percent of patients were unable to characterize their pain. Lower abdominal pain was reported by 45.8% of participants, while 26.9% had upper abdominal location. The pain was generalized in 27.3% of patients. The majority of patients (64.8) did not have any radiation of the pain. The groin, back and shoulder were the common sites of radiating pain in 20.1%, 6.4% and 1.1%, respectively. Associated symptoms helped in identifying the cause and sometimes to the presence or absence of complications. Common associated symptoms included nausea (67.4%), vomiting (57.2%), urinary symptoms (38.3%), loss of appetite (21.2%), constipation (19.3%), obstipation (12.1%), diarrhea (10.6%), abdominal distension (5.7%), per vaginal bleeding (3.4%), gastro-intestinal bleed (2.7%), and jaundice (1.9) [Table 2].
Table 2.
Pain characteristics
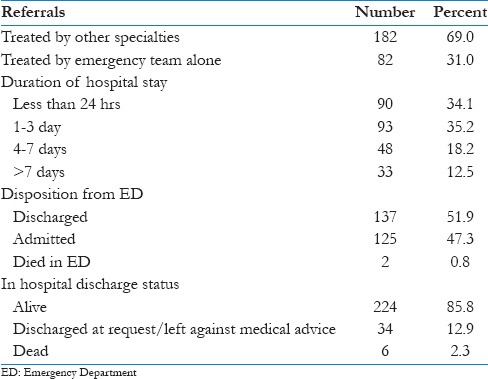
Outcomes of acute abdominal pain were described in terms of mortality and duration of hospital stay. Emergency department physicians were able to treat and discharge 31% of patients, while 69% of the patients needed referrals to other specialties. More than half the patients (51.9%) were discharged stable from the emergency department and 47.3% required hospital admission. Surgical intervention was needed in 25.8% of patients and 6.1% required admission in medical or surgical intensive care units. About 70% of participants were discharged from hospital by the third day and half of these patients were discharged within 24 hours. Longer duration of hospital stay (>3 days) was needed in 30.7% of patients. The majority of patients (85.8%) were discharged alive from the hospital while the mortality rate was 2.3% (6/294). Discharged at request or left against medical advice accounted for 12.9% of the patients [Table 3].
Table 3.
Outcome
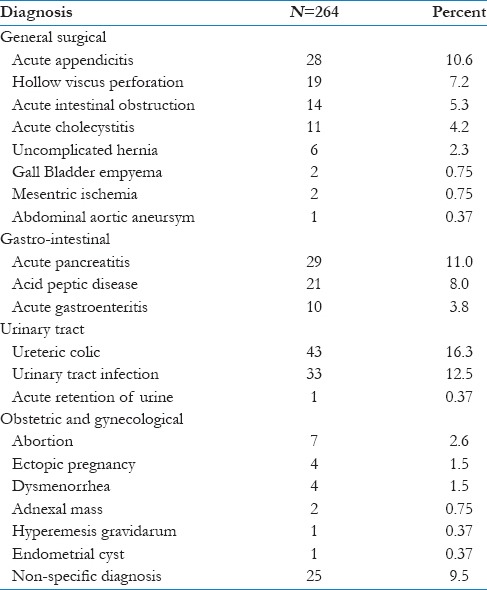
The final diagnosis at discharge was grouped as follows: Surgical (31.5%), gastro-intestinal (22.8%), urinary tract related (29.2%), obstetrics and gynecology related (7%) and non-specific diagnosis (9.5%). Among the surgical causes, acute appendicitis (10.6%), hollow viscus perforation (7.2%), intestinal obstruction (5.3%) and acute cholecystitis (4.2%) were common etiologies. Gastro-intestinal included acute pancreatitis (11%), acid peptic disease (8.0%) and acute gastroenteritis (3.8%). Ureteric colic (16.3%), urinary tract infection (12.5%) and acute urinary retention (0.37%) were common urological causes. Obstetrics and gynecological diagnosis constituted 7.2% of the total cases. Common conditions were abortion (2.6%), ectopic pregnancy (1.5%), dysmenorrhea (1.5%), adnexal mass (0.8%), hyperemesis gravidarum (0.4%) and endometrial cyst (0.4%). The cause of the abdominal pain could not be determined in 25/294 (9.5%) patients [Table 4].
Table 4.
Final diagnosis
Discussion
Acute abdominal pain is one of the most frequent complaints of patients presenting to the ED. It continues to pose diagnostic challenges for emergency clinicians and primary care doctors.[1] To the patients, the risks are missed diagnosis, over-investigation and even an undue intervention. All patients with abdominal pain do not require extensive diagnostic tests. Sometimes, adequate history and physical evaluation alone is sufficient to accurately diagnose the condition and treat accordingly. Patients may present with vague complaints and varying associated symptoms making diagnosis difficult which ranges from benign to life-threatening conditions.[2]
Abdominal pain can be the manifestation of a spectrum of disease processes.
Conditions causing acute abdominal pain may vary, from conditions needing immediate intervention, to relatively mild presentations needing careful observation to avoid over investigation and unnecessary interventions. Patients may have acute exacerbations of chronic problems (e.g., peptic ulcer disease, pancreatitis, and inflammatory bowel disease), acute surgical abdomens (e.g., appendicitis, intestinal perforation, and acute volvulus) or non-surgical abdominal emergencies (e.g. ureteric colic, biliary colic, and acute gastroenteritis).
In our study, most patients (45.1%) presented with a pain score of 5–7 on the WBS score. WBS is a standard scoring system used to assess the severity of pain and had been validated in our regional population by Bashir et al.[6] Half of them reported their pain as sudden onset while the remainder described their pain onset as gradual.
Acute-onset pain, especially if severe, should prompt immediate concern about a potential intra-abdominal catastrophe, like a ruptured abdominal aortic aneurysm, perforated viscus, mesenteric ischemia or torsion. The neural pathways give rise to predictable patterns of referred pain and radiation. In our study, the groin was the most common site of radiation and was reported by 20.1% of our patients. This correlates with the large number of ureteric colic patients in our study. Though many other associated symptoms were recorded, their value in establishing a firm diagnosis could not be established. Medical literature also suggests that associated symptoms often lack specificity and atypical presentations are common.[3,5]
Causes of acute abdominal pain include both medical and surgical.[5] In an observational study by Tariq et al. from Pakistan the most common cause of acute abdomen was acute appendicitis followed by acute pancreatitis and duodenal ulcer.[7] A study done in Ghana, Africa, also reported acute appendicitis followed by typhoid fever with ileal perforation and acute intestinal obstruction as most commonest causes of acute abdominal pain.[8] In another retrospective study done at Institute of Surgery of the University of Rome on 450 patients presenting with acute abdominal pain to the emergency department, appendicitis was the most common cause followed by non-specific abdominal pain (15.5%), cholelithiasis (12.5%) and abdominal malignancy (10.3%).[9] In our study, ureteric colic (16.3%), UTI (12.5%), acute pancreatitis (11%) and acute appendicitis (10.6%) were the most common reasons for ED visits due to abdominal pain. No specific diagnosis could be established in 9.5% of patients.
An audit done by Irvin on 1190 acute surgical admissions of which 47% were operated upon.[10] In our study, surgery was performed on 25.8% of patients. The significant difference in percentages may be due to the fact that this study was done in the emergency department, while the one by Irvin was in an acute surgical set-up.[10] The mortality rate among our study group was 2.3%, which is comparable with other studies.[8]
In our study no specific diagnosis could be established in 9.5% of patients. Conditions like dengue can also cause abdominal pain as reported by Wong et al., where a search for abdominal cause of abdominal pain may prove futile.[11] The approach becomes further difficult with special groups of population like the pregnant and the elderly presenting differently.[1] Due to these reasons, designing a common approach to acute abdominal pain is difficult. A study by Staniland et al. suggests that diagnostic accuracy in acute abdomen is around 65% and is mostly by pattern matching and for this reason a common approach or policy would result in missing a third of all the patients because they present atypically.[12] The approach to such a common complaint with complex presentations and spectrum of etiologies is not easy, but a conscious effort on part of the emergency physician can reduce mortality and morbidity.
A limitation of our study is that gold standards were not used for confirmation of the diagnosis as this is an ED-based study.
Conclusion
Abdominal pain is a common presenting complaint in the ED and clinicians must consider multiple diagnoses, especially in those cases that require immediate intervention in order to limit morbidity and mortality. It is extremely important for emergency physicians to develop the skill of identifying patients with an “acute abdomen” requiring immediate surgical intervention.
Four Cs: Caution, Consultation, Careful investigation and Close observation should be the four pillars of ED care for an acute abdomen.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Kamin RA, Nowicki TA, Courtney DS, Powers RD. Pearls and Pitfalls in the Emergency Department Evaluation of Abdominal Pain. Emerg Med Clin North Am. 2003;21:61–72. doi: 10.1016/s0733-8627(02)00080-9. [DOI] [PubMed] [Google Scholar]
- 2.Agboola JO, Olatoke SA, Rahman GA. Pattern and Presentation of Acute Abdomen in a Nigerian Teaching Hospital. Niger Med J. 2014;55:266–70. doi: 10.4103/0300-1652.132068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Powers RD, Guertler AT. Abdominal Pain in the ED: Stability and Change over 20 Years. Am J Emerg Med. 1995;13:301–3. doi: 10.1016/0735-6757(95)90204-X. [DOI] [PubMed] [Google Scholar]
- 4.Laurell H, Hansson LE, Gunnarsson U. Acute Abdominal Pain among Elderly Patients. Gerontology. 2006;52:339–44. doi: 10.1159/000094982. [DOI] [PubMed] [Google Scholar]
- 5.Saleh MA, Troy S, Etienne T. What Clinical and Laboratory Parameters Determine Significant intra-abdominal Pathology for Patients Assessed in Hospital with Acute Abdominal Pain? World J Emerg Surg. 2007;2:26. doi: 10.1186/1749-7922-2-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bashir MS, Khade A, Borkar P, Saleem M, Lingaswamy V, Reddy D. A Comparative Study between Different Pain Rating Scales in Patients of Osteoarthritis. Indian J Physiol Pharmacol. 2013;57:205–8. [PubMed] [Google Scholar]
- 7.Muhammad TA, Asma H, Waqar SH, Shah SF, Zafar IM, Zahid MA. Presentation and Outcome of Acute Abdomen in a Tertiary Care Unit. Ann Pak Inst Med Sci. 2011;7:137–44. [Google Scholar]
- 8.Ohene-Yeboah M. Acute surgical admissions for abdominal pain in adults in Kumasi, Ghana. ANZ J Surg. 2006;76:898–903. doi: 10.1111/j.1445-2197.2006.03905.x. [DOI] [PubMed] [Google Scholar]
- 9.Caterino S, Cavallini M, Meli C, Murante G, Schiffino L, Lotito S, et al. Acute abdominal pain in emergency surgery. Clinical epidemiologic study of 450 patients. Ann Ital Chir. 1997;68:807–17. [PubMed] [Google Scholar]
- 10.Irvin TT. Abdominal Pain: A Surgical Audit of 1190 emergency admissions. Br J Surg. 1989;76:1121–5. doi: 10.1002/bjs.1800761105. [DOI] [PubMed] [Google Scholar]
- 11.Wong JG, Gan VC, Ng EL, Leo YS, Chan SP, Choo R, et al. Self-Reported Pain Intensity with the Numeric Reporting Scale in Adult Dengue. PloS One. 2014;9:e96514. doi: 10.1371/journal.pone.0096514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Staniland JR, Ditchburn J, DeDombal FT. Clinical presentation of acute abdomen: Study of 600 patients. Br Med J. 1972;3:393–8. doi: 10.1136/bmj.3.5823.393. [DOI] [PMC free article] [PubMed] [Google Scholar]