

Abstract
Introduction:
Diabetes is an important public health problem of India. Studies have shown that increase in patients’ knowledge regarding the disease results in better compliance to treatment and decrease in complications. This study was planned to assess the knowledge about diabetes and its correlation with pharmacological and non-pharmacological compliance, among the diabetic patients attending rural health center from Sangli District, Maharashtra (India).
Materials and Methods:
The study was conducted during September to November 2014. The study subjects were all willing adult patients with type II diabetes mellitus attending a selected rural hospital. The study tool was pretested and self-administered questionnaire. Analysis was done using Microsoft Excel and SPSS-22.
Results:
Total study participants were 307 in number, with the mean age of 55.6 years. The mean morbidity with diabetes was 10.7 years. Only 23.8% had good knowledge regarding diabetes, while 19.2% participants had poor knowledge. Knowledge was significantly associated with the compliance to the pharmacological and non-pharmacological management.
Conclusion:
Although most of the patients were suffering with diabetes for many years there is lack of knowledge regarding the disease and self care. The compliance to the management of diabetes was better in patients with good knowledge. Seminars, counseling sessions and workshop should be arranged periodically for diabetic patients to increase their awareness.
Keywords: Awareness, diabetes mellitus, India, medication compliance, patients
Introduction
International diabetic federation estimated that in India there are 66.8 million patients in 2013, with nearly 50% undiagnosed. Diabetes was related to one million deaths and mortality was higher under age of 60 years.[1] By 2030 there will more than 79 million diabetics, making it one of the major public health challenge to the country.[2,3] There is high burden of diabetes-related complications in Indian patients. Agrawal et al. observed retinopathy in 28.9%, nephropathy in 32.5%, neuropathy in 30.1%, cardio-atherosclerotic diseases in 19.2% and peripheral vascular diseases in 18.1% diabetic patients.[4] The investigators of A1 cheive study observed high prevalence of macrovascular and microvascular complications among the Indian diabetic patients.[5]
Different studies conducted in countries like United States have observed the positive association of patient's knowledge regarding the disease and self care to the treatment compliance.[6,7] However, such studies in Indian scenario are few and concentrated around large cities. Hence, this study was planned to assess knowledge about diabetes and its correlation with pharmacological and non-pharmacological compliance, among the diabetics attending a rural health center from Sangli District, Maharashtra (India).
Material and Methods
This was a cross-sectional study conducted in a rural health center attached to a medical college from Sangli district of Maharashtra, India. It was undertaken after Institutional ethical committee approval and permissions from the respective authorities. Written informed consent from each participant was acquired. The study population was adult type-2 diabetes patients on oral hypoglycemic drugs for at least 6 months attending the rural health centre. The patients attending for routine check up or drug re-prescription and consenting to participate were included in the study. Minors, patients on insulin, hospitalized patients, patients who had undertook any sensitization program other than routine counseling by physician and those who cannot read in the local language were excluded from the study. Prevalence of knowledge regarding diabetes in the pilot study was 52.71%; considering level of significance as 5% and error 15%; the sample size derived was 265. Sampling technique was a convenience sampling and study duration was September to December 2014.
Study instrument was a pretested, prevalidated, self-administered questionnaire with good test-retest reliability (Spearman correlation coefficient, r = 0.81) and internal consistency (Cronbach's α, r = 0.78). It was developed in Marathi language with the help of subject experts and published literature[8,9,10,11] and finalized after the pilot study. It consists of initial section with general information of patient like age, gender etc., The occupations reported by patients were classified as sedentary work, moderate work and heavy work.[8] The second section consisted of questions regarding knowledge of patients about diabetes and its complications and the answers were scored. The maximum possible knowledge score was 24. Those scoring under 50%, 50–75% and more than 75% were considered to be having poor, moderate and good knowledge, respectively. Final section had self-reported pharmacological compliance and non-pharmacological compliance. Pharmacological compliance was self-reported, with participants reporting to have missed more than two doses in last 15 days were considered as non-compliant.[12] Non-pharmacological compliance means adherence to the measures like diet modification and exercises. Due to lack of exact definition of compliance to the non-pharmacological management, a scale was developed with equal importance to diet modifications and physical exercises. The maximum possible score was 12 and the participants scoring above 9 (75%) were considered as compliant to non-pharmacological management.
Analysis was done using SPSS-22 and Microsoft Excel 2007. Mean, standard deviation, percentage, Chi-square and binary logistic regression were applied. Data from the pilot study and incomplete questionnaires were not included in the final analysis.
Results
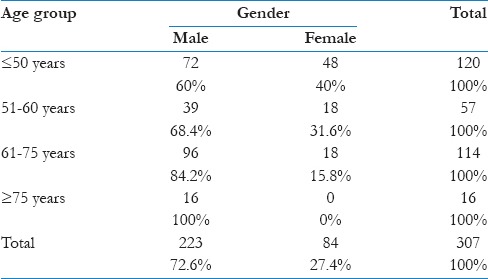
Out of 329 questionnaires collected, 307 were complete and hence used in the final analysis. Two hundred twenty-three (72.6%) participants were male while 84 (27.4%) were female [Table 1]. The mean age of study participants was 55.6 years (range 35–85 years and standard deviation ± 12.22 years). Two hundred ninety-two (95.1%) participants were married. While considering the educational status, 106 (34.5%) had studied up to secondary school and 201 (65.5%) had attended college. Among the participants: 208 (67.8%), 56 (18.2%) and 43 (14%) were sedentary, moderate and heavy workers, respectively. The mean morbidity with diabetes was 10.7 years (range: 1 to 44 years and; standard deviation: 10.02 years).
Table 1.
Age group and gender distribution of the participants
The pharmacological compliance was reported by 234 (76.2%) participants. The mean score for the non-pharmacological compliance was 8.35 (standard deviation: 2.8). Based on preset criteria of score, 156 (50.8%) participants were considered to compliant to the non-pharmacological management.
The mean score for knowledge regarding diabetes was 14.82 (standard deviation: 3.5). Only 29 (9.4%) participants had good knowledge, whereas 219 (71.3%) had moderate and 59 (19.2%) participants had poor knowledge. Age was not associated with the knowledge (Chi-square 5.47, P = 0.49), however, higher percentage of older age group (≥75 yrs) participants had poor knowledge. Gender was associated with knowledge (Chi-square 10.78, P = 0.005); higher percentage of male participants (81.6%) had moderate to good knowledge as compared to females (78.6%). Marital status and occupation were not associated with knowledge. Education was not associated with the knowledge (Chi-square 2.23, P = 0.33), however higher percentage of participants who had attended college had moderate to good knowledge.
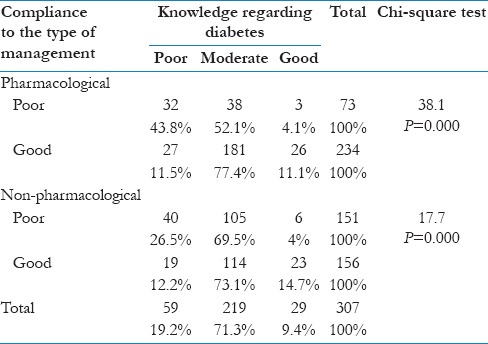
Pharmacological compliance was associated with knowledge. Among the participants with good compliance, 88.5% had moderate to good knowledge as compared to only 56.2% participants with poor compliance. Compliance to the non-pharmacological management was associated with the knowledge. The moderate to good knowledge was present in 87.8% participants with good compliance as compared to only 73.5% with poor compliance [Table 2].
Table 2.
Association between knowledge regarding diabetes with pharmacological compliance and non-pharmacological management compliance
Binary logistic regression was applied with knowledge regarding diabetes as dependent variable, while age, gender, education, occupation, pharmacological compliance and non-pharmacological management compliance as independent variables. Enter method was used to identify most significant predictors of knowledge. The chance accuracy rate for the model is 83.6%, which was greater than calculated chance accuracy rate (67.3%). Pharmacological and non-pharmacological management compliance were the highly significant predictors, while education and age were also significant predictors for knowledge regarding diabetes [Table 3].
Table 3.
Binary logistic regression model-association of age, gender, education occupation, pharmacological compliance and non-pharmacological management compliance with knowledge regarding to diabetes

Discussion
In the current study, we observed that the patients compliant with pharmacological and non-pharmacological management had good knowledge regarding diabetes.
Al-Qazaz HKh et al., (2010), observed significant correlations between the knowledge about diabetes and adherence to the treatment in subjects from Penang.[13] Sweileh et al., when carried out a study at Al-Makhfia governmental diabetes primary healthcare clinic in Nablus, Palestine in 2012, observed that diabetic patients with high knowledge were less likely to be non-adherent.[14] These observations are similar to the results obtained in the current study. This reflects the importance of knowledge regarding diabetes among the patients for better compliance.
Chaudhary et al., from Multan (Pakistan) in 2010, observed that male gender, higher education and older age (>40 years) were associated with the knowledge regarding diabetes mellitus. The observations from the current study are similar.[15] However, age groups used by them were only two: <40 years and >40 years, while in the current study four age groups were considered with lowest being 35–50 years. Abdella and Mohammad studied awareness of diabetic patients about their illness and associated complications in Ethiopia (2012); majority of patients (67%) had good knowledge on actions to be taken on the occurrence of acute complications and reasons for developing acute complications.[16] While we observed that less than 10% participants had good knowledge. However, there is difference in the questionnaire used in both the studies and most of the participants from Abdella study had undergone sensitization unlike the current study subjects. This could be the reason behind the difference in the observations.
Mumu et al., at Daka (Bangladesh) 2013, observed that 19% respondents had poor knowledge, while 68% had average and 13% had good knowledge. They also deduced that male gender and higher educated people are likely to have better knowledge regarding Diabetes.[17] Muninarayana et al. conducted a study on adults in Tamaka village, Kolar (India) in 2009. They observed 74.2% of diabetics were aware of the complications. This study also revealed that knowledge regarding diabetes was very poor in rural areas.[18] Rujul et al. observed that male gender, higher education and younger age of respondents was significantly associated with level of knowledge, while type of occupation is not associated with it.[19] These studies have similar results as our observations.
Bansal et al. observed compliance to medication in 82.5% patients from rural area of Ludhiana district, India.[20] Rao et al. observed that 83.6% patients from Southern Karnataka were on regular medication.[21] Santhanakrishnan et al. observed compliance to oral hypoglycemic agents in 76% subjects, dietary modifications in 81.4% and physical activity in 37% subjects from Puducherry, India.[12] While in the current study, pharmacological compliance was reported by 76.2% participants and compliance to the non-pharmacological management was reported by 50.8% participants. The results observed by us were similar to the above-mentioned findings.
Being a self-administered questionnaire reporting bias cannot be totally eliminated; there may be over-estimation of compliance. Confounders like economical state, availability of medications, counseling by health professionals, exposure to information through media, additional use of ayurvedic/homeopathic/other indigenous systems of medicines etc., may be present and are not considered in the current study. Only self-reported compliance was considered without confirming.
Conclusion
Compliance to the management of diabetes depends on knowledge regarding it. However, many of the patients have poor knowledge regarding the disease, the situation is worse among the females. Lower level of literacy and old age hinder the presence of knowledge regarding the diabetes. Seminars, counseling sessions and workshop should be arranged periodically for diabetic patients to increase their awareness regarding diabetes disease in total per say.
Footnotes
Source of Support: Nil.
Conflict of Interest: None.
References
- 1.6th ed. Brussels, Belgium: International Diabetes Federation; 2013. [Last cited on 2015 Jan 06]. International Diabetes Federation. IDF Diabetes Atlas. Available from: http://www.idf.org/diabetesatlas . [Google Scholar]
- 2.Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes-estimates for the year 2000 and projections for 2030. [Last cited on 2015 Jan 06];Diabetes Care. 2004 27:1047–53. doi: 10.2337/diacare.27.5.1047. Available from: http://care.diabetesjournals.org/content/27/5/1047.long . [DOI] [PubMed] [Google Scholar]
- 3.Mohan V, Sandeep S, Deepa R, Shah B, Varghese C. Epidemiology of type 2 diabetes: Indian scenario. Indian J Med Res. 2007;125:217–30. [PubMed] [Google Scholar]
- 4.Agrawal RP, Ranka M, Beniwal R, Sharma S, Purohit VP, Kochar DK, et al. Prevalence of micro and macro vascular complications in type 2 diabetes and their risk factors. [Last cited on 2015 Jan 06];Int J Diab Dev Ctries. 2004 24:11–6. Available from: http://diabetes.org.in/journal/2004_jan-mar/original_article1.pdf . [Google Scholar]
- 5.Mohan V, Shah S, Saboo B. Current glycemic status and diabetes related complications among type 2 diabetes patients in India: Data from the A1chieve study. [Last cited on 2015 Jan 06];J Assoc Physicians India. 2013 61(Suppl 1):12–5. Available from: http://www.japi.org/january_special_issue_2013_a1chieve/04_oa_current_glycemic_status_and.pdf . [PubMed] [Google Scholar]
- 6.Heisler M, Piette JD, Spencer M, Kieffer E, Vijan S. The relationship between knowledge of recent HbA1c values and diabetes care understanding and self-management. [Last cited on 2015 Jan 06];Diabetes Care. 2005 28:816–22. doi: 10.2337/diacare.28.4.816. Available from: http://care.diabetesjournals.org/content/28/4/816.long . [DOI] [PubMed] [Google Scholar]
- 7.Norris SL, Engelgau MM, Narayan KM. Effectiveness of self-management training in type 2 diabetes: A systematic review of randomized controlled trials. [Last cited on 2015 Jan 06];Diabetes Care. 2001 24:561–87. doi: 10.2337/diacare.24.3.561. Available from: http://care.diabetesjournals.org/content/24/3/561.long . [DOI] [PubMed] [Google Scholar]
- 8.Basavanthappa BT. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd; 2008. Community Health Nursing; p. 278. [Google Scholar]
- 9.Ahmad B, Ramadas A, Quek KF. The development and validation of diabetes knowledge questionnaire for the Indigenous population in Malaysia. [Last cited on 2015 Jan 09];Med J Malaysia. 2010 65:273–6. Available from: http://www.e-mjm.org/2010/v65n4/Diabetes_Knowledge.pdf . [PubMed] [Google Scholar]
- 10.Sweileh WM, Zyoud SH, Abu Nab’a RJ, Deleq MI, Enaia MI, Nassar SM, et al. Influence of patients’ disease knowledge and beliefs about medicines on medication adherence: Findings from a cross-sectional survey among patients with type 2 diabetes mellitus in Palestine. [Last cited on 2015 Jan 09];BMC Public Health. 2014 14:94. doi: 10.1186/1471-2458-14-94. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/pmid/24479638 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Diabetes Initiative. Princeton, New Jersey: Robert Wood Johnson Foundation 2009; 2009. [Last cited on 2015 Jan 09]. Patient's diabetes knowledge questionnaire. Available from: http://www.diabetesinitiative.org/resources/type/assessmentInstruments.html . [Google Scholar]
- 12.Santhanakrishnan I, Lakshminarayanan S, Kar SS. Factors affecting compliance to management of diabetes in Urban Health Center of a tertiary care teaching hospital of south India? [Last cited on 2014 Dec 14];J Nat Sc Biol Med. 2014 5:365–8. doi: 10.4103/0976-9668.136186. Available from: http://www.jnsbm.org/text.asp?2014/5/2/365/136186 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Al-Qazaz HKh, Sulaiman SA, Hassali MA, Shafie AA, Sundram S, Al-Nuri R, et al. Diabetes knowledge, medication adherence and glycemic control among patients with type 2 diabetes. [Last cited on 2014 Jan 13];Int J Clin Pharm. 2011 33:1028–35. doi: 10.1007/s11096-011-9582-2. Available from: http://link.springer.com/article/10.1007%2Fs11096-011-9582-2#page-1 . [DOI] [PubMed] [Google Scholar]
- 14.Sweileh WM, Zyoud SH, Abu Nab’a RJ, Deleq MI, Enaia MI, Nassar SM, et al. Influence of patients’ disease knowledge and beliefs about medicines on medication adherence: Findings from a cross-sectional survey among patients with type 2 diabetes mellitus in Palestine. [Last cited on 2014 Jan 13];BMC Public Health. 2014 14:94. doi: 10.1186/1471-2458-14-94. Available from: http://www.biomedcentral.com/1471-2458/14/94 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chaudhary FM, Chaudhary SM. Awareness about diabetes risk factors and complications in diabetic patients: A cross-sectional study. [Last cited on 2014 Jan 13];Nishtar Medical Journal. 2010 2:84–8. Available from: http://www.thenmj.com/archives/7/AWARENESS%20ABOUT%20DIABETES%20RISK%20FACTORS%20and%20COMPLICATIONS%20IN%20DIABETIC%20 PATIENTS%20A%20CROSS-SECTIONAL%20STUDY.pdf . [Google Scholar]
- 16.Abdella SH, Mohammed MA. Awareness of Diabetic Patients about their Illness and Associated Complications in Ethiopia. [Last cited on 2015 Jan 13];Med Sci. 2013 2:512–22. Available from: http://www.scopemed.org/fulltextpdf.php?mno=29340 . [Google Scholar]
- 17.Mumu SJ, Saleh F, Ara F, Haque MR, Ali L. Awareness regarding risk factors of type 2 diabetes among individuals attending a tertiary-care hospital in Bangladesh: A cross-sectional study. [Last cited on 2015, Jan 13];BMC Res Notes. 2014 7:599. doi: 10.1186/1756-0500-7-599. Available from: http://www.biomedcentral.com/1756-0500/7/599 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Muninarayana C, Balachandra G, Hiremath SG, Iyengar K, Anil NS. Prevalence and awareness regarding diabetes mellitus in rural Tamaka, Kolar. Int J Diabetes Dev Ctries. 2010;30:18–21. doi: 10.4103/0973-3930.60005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rujul D, Vadgama P, Parth D. Effect of Awareness of diabetes on clinical outcomes of diabetes: An observational study at a private hospital in Gujarat. Natl J Med Res. 2012;2:493–6. [Google Scholar]
- 20.Bansal P, Chaudhary A, Gupta VK, Satija M, Giridhar S, Kaushal P. Compliance of known diabetics regarding treatment and monitoring in rural Ludhiana. [Last cited on 2015 Jan 13];Int J Res Health Sci. 2014 2:172–6. Available from: http://www.ijrhs.com/issues.php?val=Volume2andiss=Issue1 . [Google Scholar]
- 21.Rao CR, Kamath VG, Shetty A, Kamath A. Treatment compliance among patients with Hypertension and Type 2 Diabetes mellitus in a coastal population of Southern India. [Last cited on 2015, Jan 13];Int J Prev Med. 2014 5:992–8. Available from: http://www.ijpm.mui.ac.ir/index.php/ijpm/article/view/1342/1657 . [PMC free article] [PubMed] [Google Scholar]