

Abstract
Objectives
To explore factors associated with short and long-term HBV DNA suppression in a multinational cohort of HIV-HBV co-infected subjects receiving HBV-active antiretrovirals.
Methods
115 HIV-HBV co-infected subjects participating in one of two global ACTG randomized clinical trials of different antiretroviral regimens received either HBV-monotherapy with either lamivudine or emtricitabine (N=56) or HBV-dual therapy with TDF plus lamivudine or emtricitabine (N=59). Associations of pre-treatment characteristics with the primary (HBV DNA <200 IU/ml at 24 weeks) and longitudinal outcomes through 144 weeks were explored using logistic regression. HBV drug-resistance mutations were determined by pol sequencing in those with viral rebound.
Results
The proportion with HBV DNA<200 IU/ml was 60% (95% CI 50%–69%) at 24 weeks and 79% (95% CI 69%–88%) at 144 weeks. Pre-treatment factors associated with the primary outcome were HBV DNA, CD4 T-cell count, and AST, but only pre-treatment HBV DNA remained associated with long-term suppression (P<0.0001). HBV therapy group was not significantly associated with the primary outcome at 24 weeks; however, longitudinally, a greater proportion in the dual therapy group achieved HBV DNA<200 IU/mL (P=0.007). A higher proportion of hepatitis B e antigen negative subjects (n=57) achieved HBV DNA <200 IU/ml at any point, regardless of therapy group. All 12 subjects with emergence of lamivudine-resistant mutants were in the monotherapy group.
Conclusions
TDF-based dual HBV-active antiretroviral therapy is preferred to treat HIV-HBV co-infected patients. In resource-limited settings where TDF may not be universally available, lamivudine or emtricitabine HBV-monotherapy is a reasonable option in patients with low HBV replication.
Keywords: hepatitis B, HIV, lamivudine, tenofovir, HBV treatment, emtricitabine
Introduction
Chronic hepatitis B, which is the leading cause of end stage liver disease worldwide, is common in human immunodeficiency virus type-1 (HIV)-infected individuals.[1–5] There are limited data on hepatitis B virus (HBV) treatment in HIV-infected patients from resource-limited settings where HBV endemicity is high. In most studies of HBV treatment from resource-rich settings, HIV-HBV co-infected individuals are usually positive for hepatitis B e antigen (HBeAg) and have high HBV DNA, characteristics associated with nearly all of these individuals having lamivudine-resistant HBV after 4 years of lamivudine.[6, 7] For these reasons and because tenofovir disoproxil fumarate (TDF) is widely available, TDF-based antiretroviral therapy (ART) regimens are recommended for HIV-HBV co-infected patients in these locations. However, in many resource-limited settings, TDF, even though recommended by World Health Organization (WHO) for first-line treatment, is still not affordable and not universally recommended for HIV-HBV co-infected patients.[8] In fact, 13 of 58 (22%) low- or medium-income focus countries have not adopted TDF with lamivudine or emtricitabine as the preferred first-line antiretroviral regimen.[8] Thus, ART regimens where lamivudine is the only drug active against HBV continue to be used.
HIV-HBV co-infection in resource-limited settings differs from that in resource-rich settings because there is a higher prevalence of HBeAg-negative disease and of individuals with HBV DNA levels <20,000 IU/ml.[9–12] Thus, the long-term efficacy of lamivudine-based ART in resource-limited settings may be different than in resource-rich settings. A Thai study of 11 HBeAg-negative and 19 HBeAg-positive HIV-HBV co-infected subjects taking lamivudine-based ART for up to 5 years found that all the HBeAg-negative subjects maintained suppression (HBV DNA <150 IU/ml) and none developed lamivudine-resistant HBV.[13] In contrast, of the HBeAg-positive subjects, only 7/19 (37%) maintained suppression, and 50% of those not suppressed developed lamivudine-resistant HBV.
To date, a comparison of lamivudine- or emtricitabine-based ART versus TDF-based ART in HIV-HBV co-infected subjects that includes resource-limited countries has not been performed. Previously, we reported on pre-ART characteristics of a subgroup of HIV-HBV co-infected subjects from two randomized clinical trials (RCT) conducted by the Adult AIDS Clinical Trials Group (ACTG) in diverse resource-limited settings. The first, ACTG A5175 (PEARLS), enrolled HIV-infected men and women in nine countries to compare three initial ART regimens.[14] The second, A5208 (OCTANE), compared the response to first-line ART in women who had and had not received single-dose nevirapine for prevention of mother-to-child transmission of HIV in 7 African countries.[15] Using this pre-defined subgroup of HIV-HBV co-infected individuals from these two trials, we compared outcomes between those who received only one agent with anti-HBV activity (lamivudine or emtricitabine) to those who received two anti-HBV agents (TDF plus lamivudine or emtricitabine) to test whether HBV outcomes differed between these groups and also within subgroups defined on baseline HBV DNA.
Methods
Study subjects
This study included HIV-HBV co-infected individuals followed in either A5175 or A5208, as previously described (Table 1).[14, 15] In brief, HIV-HBV co-infected participants in this study were hepatitis B surface antigen (HBsAg) positive at screening, negative for chronic hepatitis C, and met one of the following three criteria at the study entry visit: positive for HBeAg or hepatitis B e antibody (anti-HBe), or HBV DNA >200 IU/mL. For the 85 (74%) participants from A5175, the anti-HBV agent(s) included either once-daily lamivudine, emtricitabine, or TDF plus emtricitabine (often co-formulated). To complete their anti-HIV ART regimen, they also received either atazanavir or efavirenz, and if not assigned TDF plus emtricitabine, then another NRTI (either zidovudine, stavudine or ddI). Randomization to the ART regimen did not account for HBV infection status. However, sites could add a second anti-HBV agent if a co-infected subject were randomized to a regimen that included only emtricitabine or lamivudine (one subject added adefovir). Participants from A5208 received once-daily TDF plus emtricitabine with either nevirapine or lopinavir/ritonavir. The pre-ART characteristics of the subjects included in this study were described previously.[9]
Table 1.
Baseline characteristics by therapy group
| Characteristic | Monotherapy N=56 |
Dual therapya N=59 |
Overall N=115 |
Pg |
|---|---|---|---|---|
| Age, years (IQR)b | 35 (30, 39.5) | 34 (29, 40) | 34 (30, 40) | 0.15 |
| Country of origin (N, %)c,d | 0.001 | |||
| Botswana (M) | 0 (0) | 4 (6.8) | 4 (3.5) | |
| Haiti (L) | 4 (7.1) | 2 (3.4) | 6 (5.2) | |
| India (L) | 9 (16.1) | 4 (6.8) | 13 (11.3) | |
| Kenya (L) | 0 (0) | 3 (5.1) | 3 (2.6) | |
| Malawi (L) | 16 (28.6) | 8 (13.6) | 24 (20.9) | |
| Peru (M) | 4 (7.1) | 2 (3.4) | 6 (5.2) | |
| South Africa (M) | 3 (5.3) | 14 (23.7) | 17 (14.8) | |
| Thailand (M) | 4 (7.1) | 4 (6.8) | 8 (7.0) | |
| United States (H) | 8 (14.3) | 2 (3.4) | 10 (8.7) | |
| Zimbabwe (L) | 8 (14.) | 16 (27.1) | 24 (20.9) | |
| Male (N, %)e | 35 (62.5) | 19 (32.2) | 54 (47.0) | 0.001 |
| Race (N, %)c | ||||
| Asian | 13 (23.2) | 8 (13.6) | 21 (18.3) | 0.30 |
| African American | 37 (66.1) | 48 (81.4) | 85 (73.9) | |
| White | 2 (3.6) | 1 (1.7) | 3 (2.6) | |
| Other | 4 (7.1) | 2 (3.4) | 6 (5.2) | |
| CD4 count groups (cells/mm3) (N,%)c | ||||
| < 50 | 11 (19.6) | 7 (11.9) | 18 (15.7) | 0.06 |
| 50 – 99 | 10 (17.9) | 13 (22.0) | 23 (20.0) | |
| 100 – 149 | 7 (12.5) | 18 (30.5) | 25 (21.7) | |
| 150 – 199 | 7 (12.5) | 10 (16.9) | 17 (14.8) | |
| 200 – 249 | 13 (23.2) | 5 (8.5) | 18 (15.7) | |
| 250 – 299 | 8 (14.3) | 6 (10.2) | 14 (12.2) | |
| HIV RNA, log cp/mlb (IQR) | 4.9 (4.5, 5.4) | 5.3 (4.7, 5.8) | 5.1 (4.6.5.6) | 0.02 |
| Hemoglobin, g/dLb (IQR) | 12.4 (11.2, 13.8) | 11.5 (10.2, 13.3) | 11.9 (10.9, 13.7) | 0.009 |
| ALT, U/Lb (IQR) | 28 (20.5, 37.5) | 25 (18, 44) | 25.5 (19, 38) | 0.64 |
| AST U/Lb (IQR) | 35.1 (24.5, 49.5) | 33 (27.2, 42) | 34 (27, 44) | 0.88 |
| HBeAg+ (N, %)f | 27 (48.2) | 29 (49.1) | 57 (49.6) | 0.92 |
| HBV DNA >200 IU/ml (N, %)c,f | 49 (87.5) | 54 (91.5) | 103 (89.6) | 0.52 |
| HBV DNA, log10 IU/mlb (IQR) | 5.2 (2.8, 8.2) | 4.9 (2.6,7.52) | 5.1 (2.7, 8.1) | 0.58 |
| HBV DNA categories | ||||
| < 2,000 IU/mL | 19 (33.9) | 21 (35.6) | 40 (34.8) | |
| 2,000 – 20,000 IU/mL | 3 (5.4) | 5 (8.5) | 8 (7.0) | |
| > 20,000 IU/mL | 33 (58.9) | 32 (54.2) | 65 (56.5) | |
| Missing | 1 (1.8) | 1 (1.8) | 2 (1.7) | |
| HBV DNA genotype (n,%)f | 0.64 | |||
| A | 29 (51.8) | 40 (67.8) | 69 (60.0) | |
| C | 3 (5.4) | 2 (3.4) | 5 (4.3) | |
| D | 9 (16.1) | 6 (10.2) | 15 (13.0) | |
| E | 2 (3.6) | 2 (3.4) | 4 (3.5) | |
| F | 2 (3.6) | 1 (1.7) | 3 (2.6) | |
| Missing | 11 (19.6) | 8 (13.6) | 19 (16.5) | |
| HDV antibody negative (N,%)c | 54 (96.4) | 44 (74.6) | 98 (85.2) | <0.01 |
one person received adefovir plus emtricitabine
median values
Fisher’s Exact
The L, M, H designation after the country name represent the income level as classified by the World Bank (http://data.worldbank.org/country) with L representing low and low middle, M upper middle, and H high income.
Chi-Square
HBV characteristics determined among 113 of the 115 subjects. Two subjects did not have serum available at baseline.
P-values represent difference between the monotherapy and dual therapy groups
Informed consent for the parent RCTs was obtained from the study subjects in their native language. This study was approved by the local IRBs and Johns Hopkins University IRB.
The following study entry variables were used in the current analysis: age, sex, race, body-mass index (BMI), history of liver disease, hemoglobin, HIV disease stage, plasma HIV RNA, CD4+ T-cell count, ALT, and AST. At 24-week intervals during follow-up, plasma HIV RNA and CD4+ T-cell count, and ALT/AST (only available from A5175) were extracted from the parent study database. During the same follow-up intervals, stored serum samples were tested for HBeAg, anti-HBe, and HBV DNA. HBV pol sequencing was performed on samples from the following scenarios: 1) visits exhibiting evidence of rebound, defined as >1 log10 IU/ml HBV DNA increase from nadir level or HBV DNA >1000 IU/ml after being undetectable (<200 IU/mL), 2) week 48 visit if HBV DNA decline from baseline ≤1 log10 IU/ml.
Laboratory testing
All serum specimens were stored at −80°C. Serological testing for HBeAg (ETI-EBK Plus, Diasorin, Stillwater MN) and anti-HBe (ETI-AB-EBK Plus, Diasorin) were performed according to manufacturer’s instructions. HBV DNA was determined with real-time PCR using either RealART™ HBV LC PCR v 3.0 (Qiagen, Valencia, CA) or Abbott RealTime HBV DNA (Abbott Molecular, Des Plains, IL). The highest common lower limit of detection of these assays was 200 IU/ml, which is the value used as undetectable in the analyses. HBV genotype and drug-resistance mutations were determined by HBV pol sequencing, performed as previously described.[6]
Statistical analysis
Comparison groups were defined as those who started two anti-HBV medications (primarily emtricitabine plus TDF—dual therapy group) versus those who started only one anti-HBV medication (emtricitabine or lamivudine—monotherapy group). The primary outcome was HBV DNA <200 IU/ml at 24 weeks following treatment initiation and was compared in an intent-to-treat analysis between groups using Fisher’s exact test. Associations between pre-treatment characteristics and the primary outcome were tested using Chi-square or Fisher’s Exact Tests for discrete covariates and Wilcoxon Rank-Sum Test for continuous covariates, and fit to logistic regression models one at a time (univariable). To adjust for possible confounding, multivariable logistic regression modeling included variables having P<0.10 in univariable models, treatment comparison group, and covariates associated with treatment group. For significantly associated continuous covariates, linearity in the logit was graphically examined, and if rejected, categories were formulated as suggested by the data (e.g. quartiles).
Secondary outcomes included HBV DNA <200 IU/ml at each 24-week follow-up time through week 144, ALT and AST normalization or elevations, HBeAg seroconversion, and durability of HBV DNA suppression. Longitudinal analyses of HBV DNA <200 IU/mL over time used marginal longitudinal modeling estimated via generalized estimating equations, with a logit link, and an exchangeable log odds ratio structure for within participant correlation. ALT and AST levels were graded according to standard ACTG definitions.[16] Among the subgroup of HBeAg-positive subjects at entry, the outcome of HBeAg seroconversion was defined as negative HBeAg and positive anti-HBe. Durability of HBV DNA suppression was formulated in two ways. First, for the subset who achieved HBV DNA <200 IU/ml, it was examined as time to loss of HBV DNA < 200 IU/mL grouped in 24-week intervals. Second, durability was examined as time to loss of a 1 log10 IU/mL HBV DNA decline or time to loss of HBV DNA <200 IU/ml (among those whose low HBV DNA at baseline did not permit a 1 log10 decline) grouped in 24-week intervals.
As-treated analyses, which excluded subjects once they were no longer taking the same number of anti-HBV medications as assigned at entry (e.g. persons adding TDF when assigned to emtricitabine alone), were performed as sensitivity analyses to the primary, intent-to-treat comparisons, which did not consider treatment information after ART initiation. Subgroup analyses were performed according to baseline HBeAg status and HBV DNA. Additionally, a post-hoc subgroup analysis was performed to further explore the hypothesis that monotherapy with lamivudine or emtricitabine may be effective in people with low baseline HBV DNA (<20,000 IU/ml), a level chosen because there is a greater risk for poor liver outcomes above this level [17]. We estimated the proportion of participants with baseline HBV DNA <20,000 IU/ml who achieved HBV DNA <200 IU/ml at 24-week intervals stratified by therapy group.
For all analyses, missing data were ignored and significance was set at 0.05 without adjustment for multiple comparisons.
Results
Of the 115 HIV-HBV co-infected subjects, 56 (49%) received either lamivudine (n=25) or emtricitabine (n=31) as the only anti-HBV drug (monotherapy) and 59 (51%) received dual therapy with 58/59 subjects receiving TDF and emtricitabine and one receiving adefovir and emtricitabine. At least 88% of the expected HBV DNA results were available among participants in follow-up through week 144 (N=89).
All the subjects in the monotherapy group and 28 (47%) in the dual therapy group were from A5175. Of the demographic and HIV pre-treatment characteristics, the two comparison groups differed by sex (P=0.001), country of origin (P=0.001), CD4+ T-cell count distribution (P=0.06), plasma HIV RNA (P=0.02), and hemoglobin (P=0.009) (Table 1). The differences in sex and country of origin were expected due to the distribution of the subjects from the two RCTs. None of the HBV characteristics were significantly different between monotherapy and dual therapy groups with 50% being HBeAg negative (Table 1). The median HBV DNA in the mono and dual therapy groups was 5.2 and 4.9 log10 IU/ml, respectively. Forty-eight (41.8%) subjects had HBV DNA <20,000 IU/ml prior to ART while 46 (45.2%) were >2.0 × 107 IU/ml. Genotype A HBV was the most common (60%) followed by genotype D (15%); the genotype distributions in the two comparison groups were similar.
HBV DNA <200 IU/ml
The proportion of subjects achieving HBV DNA <200 IU/ml was 60% (66/100; 95% CI 50–69%) for the primary outcome at week 24 and 79% at week 144 (62/78; 95% CI 69–88%) (Figure 1). In the comparison groups at week 24, 57% (30/53; 95% CI 42–70%) in the monotherapy and 63% (36/57; 95% CI 49% to 76%) in the dual therapy group (exact P = 0.56) achieved HBV DNA <200 IU/ml. However, the estimated proportion with HBV DNA <200 IU/mL increased more over time in the dual than in the monotherapy group (p=0.007) (Figure 1). This between group difference over time remained statistically significant (P=0.02) when adjusted for baseline HBV DNA and HBeAg. The as-treated analysis, which included 98.5% of the expected visits, was similar to the ITT analysis.
Figure 1.
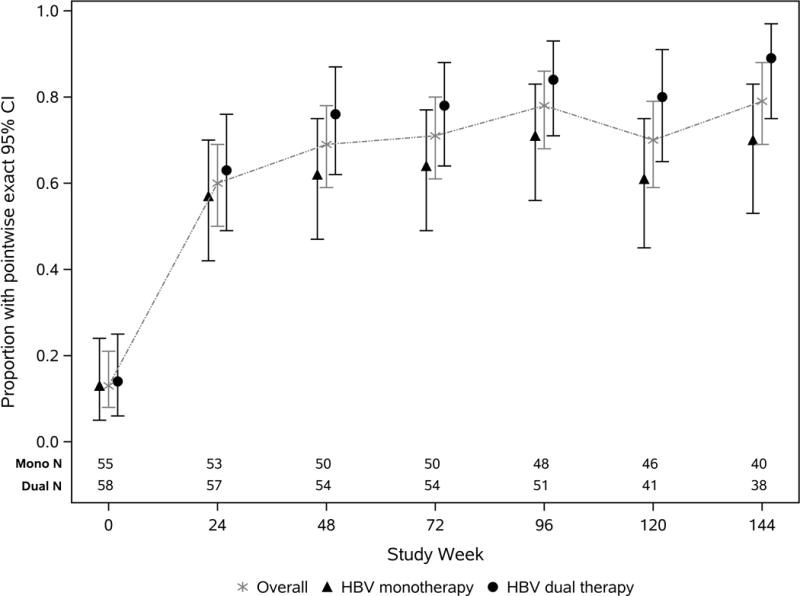
Estimated proportion of HBV DNA < 200 IU/mL (y-axis) through 144 weeks stratified by HBV treatment group.
Initial multivariable models included pre-treatment characteristics associated with HBV comparison groups or with the primary outcome. Sex, HIV-1 RNA, hemoglobin, CD4 cell count, and HDV status were all associated with HBV DNA comparison groups (Table 1), while AST, HBeAg, and HBV DNA were associated with the primary outcome. Hemoglobin was removed from the multivariable model due to co-linearity with sex and CD4 count. The linearity in the logit was rejected for CD4 cell count and AST; therefore, these variables were grouped in quartiles. In the multivariable model for the primary outcome, HBV therapy group was not associated (OR 1.8, 95% CI: 0.5–7.9, Table 2). Participants with baseline CD4 cell count <70 cells/mm3 were 14.8-fold (95% CI: 1.9–201.7) more likely to achieve HBV DNA <200 IU/mL at week 24 compared to those with >140 cells/mm3. However, change in CD4+ T-cell count from baseline to 24 weeks was not associated. Higher AST (>44 IU/mL) compared to lower levels (< 33 U/L) were associated with HBV DNA <200 IU/mL at 24 weeks (OR 14.1, 95% CI: 1.9 – 228.6) as was lower baseline HBV DNA (OR 4.6/log10 HBV DNA decrease, 95% CI: 2.7 – 10.9). Lower baseline HBV DNA was the only variable that remained significantly associated longitudinally (P<0.0001).
Table 2.
Multivariable logistic regression model primary outcome of HBV DNA <200 IU/ml at 24 weeks
| Univariate OR (95% CI) | Multivariate OR (95% CI) | |
|---|---|---|
| Dual vs. monotherapy (i) | 1.4 (0.6–3.0) | 1.8 (0.5–7.9) |
| Baseline CD4+ T-cell count (ii) | ||
| <70 cells/mm3 (lowest observed quartile) | 1.5 (0.6–4.0) | 14.8 (1.9–201.7) |
| 70–140 cells/mm3 (observed second quartile) | 1.0 (0.4–2.6) | 1.7 (0.3–9.6) |
| >140 cells/mm3 (above observed median) | 1.0 (ref) | 1.0 (ref) |
| Baseline AST Value (iii) | ||
| < 33 (U/L) (below observed median) | 1.0 (ref) | 1.0 (ref) |
| 33–44 (U/L) (observed third quartile) | 0.7 (0.3–1.9) | 3.1 (0.5 – 25.0) |
| >44 (U/L) (highest observed quartile) | 0.5 (0.2–1.3) | 14.1 (1.9 – 228.6) |
| Baseline HBV DNA (per 1 log10 IU/ml decrease) (iv) | 2.7 (2.0–4.0) | 4.6 (2.7–10.9) |
Forced into all models – tests for interaction terms between this comparison group and CD4 group, AST group, and HBV DNA (in separate models) were not significant.
Actual CD4 cell count entered into initial multivariable model due to association with HBV comparison group, retained by stepwise selection, and groups formed due to linearity in the logit being rejected
Actual AST value entered into initial multivariable model due to association with primary outcome, retained by stepwise selection, and groups formed due to linearity in the logit being rejected
Actual HBV DNA levels entered into initial multivariable model due to association with primary outcome, retained by stepwise selection, and linearity in the logit not rejected.
Other baseline covariates entered into initial multivariable model due to association with HBV comparison group included the following: sex, plasma HIV-1 RNA, hemoglobin, and HDV antibody. Hemoglobin removed due to collinearity.
HBeAg at baseline entered into initial multivariable model due to association with primary outcome, but was not retained in stepwise selection process.
A subgroup analysis to determine if achieving HBV DNA <200 IU/ml differed based on pre-treatment HBeAg status demonstrated that a greater proportion of HBeAg-negative subjects achieved HBV DNA <200 IU/mL at week 24 (47 of 53, 89%) than HBeAg-positive subjects (18 of 56, 32%). This finding was true over both HBV therapy groups, and this difference significantly increased over time (P=0.04).
HBeAg seroconversion
Overall, 16 of the 53 (30%) HBeAg-positive subjects had HBeAg seroconversion, with 10 occurring in the first 48 weeks. These seroconversions were maintained throughout follow-up in 11 (69%). A significant difference was not observed between the mono and dual therapy groups with 27% and 33% seroconversions, respectively. Seroconversion was associated with higher baseline AST (median 47 versus 33 U/L)(P< 0.001), a lower baseline HBV DNA (median 2.30 versus 3.26 log10 IU/ml)(P< 0.001), and trended towards a lower baseline CD4+ T-cell count (median 63 versus 139 cells/uL)(P=0.07). Multivariable models were not informative due to the small number of outcomes.
ALT and AST outcomes
Of the 23 subjects from A5175 with grade 1–4 ALT or AST at baseline, only three did not experience normalization (one died at week 9 from bacterial pneumonia and two were lost to follow-up after weeks 4 and 16). Normalization occurred between weeks 2 and 34. Of the 74 participants from A5175 with grade 0 ALT or AST at baseline, 45 (61%) experienced an elevation to grades 1–4 during follow-up. Only two experienced a severe elevation (grade 3) and one was life-threatening (grade 4). All three subjects normalized after the elevation. The life-threatening elevation required temporary discontinuation of ART but was later successfully restarted.
Durability of HBV DNA suppression or of 1 log10 HBV DNA decline
Of the 105 subjects with ≥48 weeks of follow-up, 85 (81%) achieved HBV DNA <200 IU/ml and were followed for durability of this outcome. Nineteen (22.4%) of them did not maintain an HBV DNA <200 IU/mL and the time to rebound was similar between the monotherapy and dual therapy groups (logrank P=0.8). In particular, nine of 36 (25%) in the monotherapy group compared to 10 of 49 (20%) in the dual therapy group did not have a durable HBV DNA <200 IU/ml response. Of the 19 individuals, only four had HIV RNA >400 copies/ml at the same time as the HBV DNA rebound, and these individuals came from both the monotherapy and dual therapy groups. Of the 66 subjects who maintained HBV DNA <200 IU/ml throughout their follow-up, 53 (80%) did so for ≥24 months.
101 subjects met criteria for inclusion into the analysis for durability of ≥ l log10 IU/ml HBV DNA decline from baseline. In subjects whose baseline HBV DNA was <2000 IU/ml, achieving HBV DNA <200 IU/mL was considered a 1 log10 decline. Of the 101 subjects, 21 (20.8%) did not have a durable 1 log10 decline with the majority of failures (n=16) occurring within 18 months of having an initial response. In the monotherapy group, 17/47 (36.2%) individuals failed to maintain this outcome compared to 4/54 (7.4%) in the dual therapy group. Interestingly, the failures in the monotherapy group were primarily in those with HBV DNA >20,000 IU/ml (Figure 2).
Figure 2.
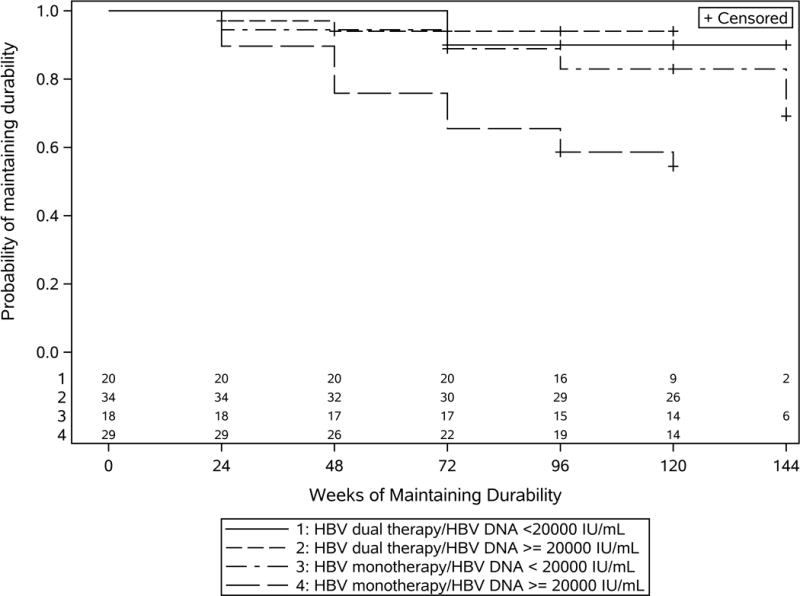
Time to loss of maintaining durability by HBV therapy group and baseline HBV DNA level stratified at 20,000 IU/ml. Durability is defined as a composite of: i) Maintaining a ≥ 1 log IU/mL HBV DNA decline from baseline or ii) maintaining HBV DNA < 200 IU/mL if baseline HBV DNA was < 2000 IU/mL. The numbers at each week describe the number of participants who were at risk of not maintaining durability. There were only a limited number of participants who were at risk for not maintaining durability at week 144.
HBV resistance
For 22 subjects, HBV pol sequencing was performed with 12 having emergence of known lamivudine-resistance mutations including one rtM204V/I, eight rtM204V/I+ rtL180M, two rtV173+rtL180M+ rtM204V/I, and one rtM204V/I+ rtM250L. These mutants all emerged in subjects in the monotherapy group (seven on lamivudine, four on emtricitabine, and one changed from lamivudine to emtricitabine).
Post-hoc subgroup analysis
Since most of the subjects who did not maintain a 1 log decline in HBV DNA over time were in the monotherapy group with HBV DNA >20,000 IU/ml, a post-hoc analysis was designed to test the hypothesis that when pre-therapy HBV DNA levels are <20,000 IU/ml, lamivudine or emtricitabine monotherapy can achieve and maintain HBV DNA <200 IU/ml. Among the 21 subjects in the monotherapy group and 25 in the dual therapy group with baseline HBV DNA <20,000 IU/ml, all were <200 IU/mL at week 24 and they were likely (>89%) to have HBV DNA <200 IU/mL at all follow-up time points regardless of whether they received mono or dual HBV therapy.
Discussion
This is the largest multinational HIV-HBV co-infected study to compare HBV outcomes between lamivudine/emtricitabine monotherapy versus TDF-based dual therapy as part of ART through 144 weeks of treatment. Another unique aspect is that ~40% of the subjects had HBV DNA <20,000 IU/ml, a group that is not included in clinical trials of anti-HBV therapies since they do not meet treatment criteria [18]. Overall, we found no difference in becoming undetectable at 24 weeks between treatment groups, but a higher proportion on TDF-based dual therapy achieved an undetectable HBV DNA over time, a finding driven primarily by those with higher baseline HBV replication. In the subgroup analysis, individuals with HBV DNA <20,000 IU/ml responded well regardless of treatment regimen through 144 weeks of therapy. In addition, the subjects in the monotherapy group who failed to maintain a response to therapy over time had HBV DNA ≥ 20,000 IU/ml. Taken together, our data support that when possible, TDF-based dual ART should be used to treat HIV-HBV co-infected patients, but in resource-limited settings where TDF may not be universally available, baseline HBV replication status, as measured by HBV DNA or HBeAg, may help determine whether lamivudine or emtricitabine monotherapy for HBV is a therapeutic option.
In many resource-limited settings the transition from stavudine-based to TDF-based ART has been slow. One challenge in phasing out stavudine is uncertainty about how to prioritize the phase-out. In resource-limited settings, studies demonstrate that HIV-HBV co-infected patients who have HBeAg-negative disease are likely to have low HBV DNA [9, 19]. This fact taken together with our current findings demonstrating that the subjects with HBV DNA <20,000 IU/ml on lamivudine-based therapy were able to maintain HBV DNA suppression through nearly three years of therapy suggests that one potential strategy is to phase out stavudine in the HIV-HBV co-infected patients who are HBeAg-positive since they will derive the most benefit. Also, our data support that for patients with known renal insufficiency where TDF is not an option, lamivudine or emtricitabine as the only HBV-active drug may be a reasonable alternative if they are HBeAg-negative or have a pre-treatment HBV DNA <20,000 IU/ml.
Lower baseline HBV DNA was the only factor in multivariable analysis that was associated with achieving HBV DNA <200 IU/ml throughout follow-up, which is consistent with other studies [20–22]. In the ALLRT cohort, 68 treatment-naïve HIV-HBV co-infected subjects received either lamivudine or TDF-based HAART, and baseline HBV DNA was the only factor associated with HBV DNA suppression at 48 weeks [21]. Interestingly, that study did not find a difference in HBV DNA suppression between the 21 subjects on TDF-based dual therapy and the 47 subjects on lamivudine monotherapy (OR 1.42, p=0.63). Similar to our study, but different from other clinical trials, the ALLRT cohort included subjects with low HBV DNA. Due to the smaller number of subjects, they could not stratify response by baseline HBV DNA.
The difference between the therapy groups in the durability of HBV DNA suppression outcome was only observed with the >1 log10 decline in HBV DNA and not with the HBV DNA <200 IU/ml outcome. This discrepancy is likely due to including more subjects with higher HBV DNA levels in the >1 log10 decline outcome compared to the HBV DNA <200 IU/ml durability outcome.
It is also important to note that at 48 weeks only 69% had undetectable HBV DNA and that even amongst those receiving TDF-based dual therapy, only 76% were undetectable, a proportion that is comparable to studies of HBV monoinfected subjects on entecavir or TDF [23–26]. Even at 144 weeks, 11% of those on TDF-based dual therapy still had a detectable HBV DNA, which is consistent with long-term data of HIV-HBV co-infected subjects from resource-rich settings[27]. Notably, those who did not suppress had baseline HBV DNA ≥ 20,000 IU/ml.
We observed unexpectedly that those with the lowest baseline CD4+ T-cell count were more likely to achieve an undetectable HBV DNA at 24 weeks but not at later time points. This may be due to differences in the robustness of the immune reconstitution in the period immediately after ART initiation. However, change in the CD4 T-cell count in the first 24 weeks was not associated with HBV DNA suppression. Since CD4+ T-cell count increase is a crude measure of immune reconstitution with ART, it is possible that those with a lower baseline CD4+ T-cell count had greater change in a different arm of the immune response in the first 24 weeks or in a specific subset of CD4+ T cells. Further studies of immune reconstitution with ART are needed to explore these hypotheses.
The rates of HBeAg seroconversion and ALT normalization did not differ between therapy groups, as is consistent with prior studies [18]. We also found that drug-resistant HBV only emerged in those on lamivudine or emtricitabine monotherapy, which is consistent with data showing no resistance with TDF-based therapy [22, 28, 29].
There are several limitations to this study. First, this was not a RCT in terms of HBV therapy, so there were differences in baseline characteristics between the groups; however, none of these differences were in HBV parameters. Second, subjects were only followed through 144 weeks, so whether other differences occur between therapy groups with longer follow-up is not known. Third, we did not have data on adherence; however, as stated in the Results, few subjects who did not have a durable HBV DNA response also lost HIV RNA suppression. Thus, adherence did not explain a large proportion of the HBV relapse.
In summary, for HIV-HBV co-infected subjects in a multinational setting, TDF/emtricitabine dual therapy for HBV as part of ART should be the first-line therapy if available and cost-effective especially in patients with HBV DNA levels ≥20,000 IU/ml or with HBeAg-positivity. For subjects with lower levels of replication, lamivudine or emtricitabine-based monotherapy is a possible alternative at least through 144 weeks of therapy. In resource-limited settings, these data may inform strategic plans regarding which patients to transition to or to initiate on TDF-based ART.
Acknowledgments
The authors would like to acknowledge the efforts of the investigators at each of the sites participating in this study, Amanda Zadzilka and James Tutko for managing the database, and the A5175 and A5208 study participants.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Allergy and Infectious Diseases or the National Institutes of Health.
Funding support: This work was supported by the National Institute of Allergy and Infectious Diseases at the National Institutes of Health [R01 AI071820 (CT), K24 AI56933 (JC), AI068636 (AIDS Clinical Trials Group), AI69450 (TC), U01 AI068634 (Statistical and Data Management Center of the AIDS Clinical Trials Group), R01CA120206 (AM), R01CA136607 (AM)]. It was also supported by Award Number U01AI068636 from the National Institute of Allergy and Infectious Diseases, the National Institute of Mental Health (NIMH), and the National Institute of Dental and Craniofacial Research (NIDCR). Study drugs were provided by Abbott Laboratories, Boehringer Ingelheim Pharmaceuticals, Gilead Sciences, Bristol-Myers Squibb, GlaxoSmithKline, and Merck & Co. Inc.
Additional funding for each site includes:
UZ-Parirenyatwa CRS (Site 30313) CTU Grant: 1U01AI069436-01
Wits HIV CRS (Site 11101) CTU Grant: 1U01AI069463-01
University of North Carolina Project, Kamuzu Central Hospital (Site 12001) CTU Grant: 1U01AI069518-01
Durban Adult HIV CRS (Site 11201) CTU Grant: 1U01AI069426-01
YRG CARE Medical Ctr., VHS CRS (Site 11701) CTU Grant: 1U01AI069432-01
Instituto de Pesquisa Clinica Evandro Chagas CRS (Site 12101) CTU Grant: 1U01AI069476-01
College of Med. JHU CRS (Site 30301) CTU Grant: 1U01AI069518-01
Chiang Mai Univ. ACTG CRS (Site 11501) CTU Grant: 1U01AI069399-01
Hospital Nossa Senhora da Conceicao CRS (Site 12201) CTU Grant: 1U01AI069401-01
Les Centres GHESKIO CRS (Site 30022) CTU Grant: 1U01AI069421-01
NARI Pune CRS (Site 11601) CTU Grant: 1U01AI069417-01
Asociacion Civil Impacta Salud y Educacion, Sede Barranco(Site 11301) CTU Grant: 5U01 AI069438
Walter Reed Project - Kenya Med. Research Institute (Site 12501) CTU Grant: IAA#Y1-AI-8374-01
AMPATH at MOI Univ. Teaching Hosp. Eldoret CRS (Site 12601) CTU Grant: IAA#Y1-AI-8374-01
Kalingalinga Clinic CRS (Site 12801) CTU Grant: 1U01AI069518-01
Gaborone and Molepolole Prevention/Treatment Trials CRSs in Botswana (Sites 12701 and 12702) CTU Grant: 1U01AI069456-01
(Site 12401) CTU Grant: 1U01AI069456-01
San Miguel CRS (Site 11302) CTU Grant: 5U01AI069438
Molepolole Prevention/Treatment Trials CRS (Site 12702) CTU Grant: 1U01AI069456-01
University of Texas Southwestern Medical Center (Site 3751) Grant: AI 046376
NARI Clinic at NIV CRS (Site 11603) CTU Grant: 1U01AI069417-01
University of Cincinnati (Site 2401) CTU Grant: AI-069513
Univ. of California Davis Med. Ctr., ACTU (Site 3851) Grant: AI38858-09S1
NARI Clinic at Gadikhana Dr. Kotnis Municipal Disp (Site 11602) CTU Grant: 1U01AI069417-01
University of Colorado Hospital CRS (Site 6101) CTU Grant: AI69450
The Ohio State University (Site 2301) CTU Grant: AI069474
Northwestern University CRS (Site 2701) CTU Grant: AI069471
University of Minnesota (Site 1501) CTU Grant: AI27661
Washington U CRS CTU (Site 2101) Grant: 1U01AI069495
Beth Israel Med. Ctr., ACTU (Site 2851) CTU Grant: AI46370
The Miriam Hospital (Site 2951) CTU Grant: AI069472-01
Duke University Medical Center CRS (Site 1601) CTU Grant: AI069484-06
University of Southern California CRS (Site 1201) CTU Grant: AI069428
Harbor-UCLA Medical Center (Site 603) CTU Grant: U01-A1 069424
UNC AIDS CRS (Site 3201) CTU Grant: AI069423; RR 025747; AI050410
Hospital of the Univ. of Pennsylvania CRS (Site 6201) CTU Grant: U01-AI- AI69467-05; CFAR Grant: P30-AI-045008-12
HIV Prevention & Treatment CRS (Site 30329) CTU Grant: 1U01AI069470
Vanderbilt Therapeutics CRS (Site 3652) CTU Grant: U01-AI069439
Rush Univ. Med. Ctr. ACTG CRS (Site 2702) CTU Grant: 1U01AI069471-01
University of Texas, Galveston (Site 6301) Grant: AI32782
New York University/NYC HHC at Bellevue Hospital (Site 401) CTU Grant: Al-27665; Al069532
Christine Hurley, RN and Roberto Corales, DO- AIDS Care CRS (Site 1108) CTU Grant: U01AI069511-02 (as of 2/12/08); CTSI: UL1 RR 024160
UCLA CARE Center CRS (Site 0601) CTU Grant: 1U01AI069424-01
University of Rochester (Site 1101) CTU Grant: U01AI069511-02 (as of 2/12/08); CRC: UL1 RR 024160
Cook County Hosp. CORE Ctr. (Site 2705) CTU Grant:1U01AI069471-01
SSTAR, Family Healthcare Ctr. (Site 2954) Grant: AI46381
Wake County Health and Human Services Clinical Research Site (Site 3206) CTU Grant: AI25868
University of Hawaii at Manoa, Leahi Hosp. (Site 5201) Grant: AI34853
Todd Stroberg, R.N., and Christina Megill, PA-C. -Cornell CTU (Site 7804) CTU Grant # AI069419 CTSC# RR024996
Footnotes
Author contributions: Study design (CT, JH, MN, UL, SL, TC, JC), data analysis (CT, LS, KH, JC), data collection (MS, HS, SS, SK, HI, AM), drafting of manuscript (CT, LS, KH, JC), critical reading of manuscript (all authors).
None of the authors have a potential conflict of interest.
References
- 1.Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol. 2006;44:S6–S9. doi: 10.1016/j.jhep.2005.11.004. [DOI] [PubMed] [Google Scholar]
- 2.Zhou J, Dore GJ, Zhang F, Lim PL, Chen YM. Hepatitis B and C virus coinfection in The TREAT Asia HIV Observational Database. J Gastroenterol Hepatol. 2007;22:1510–1518. doi: 10.1111/j.1440-1746.2007.05062.x. [DOI] [PubMed] [Google Scholar]
- 3.Nyirenda M, Beadsworth MB, Stephany P, Hart CA, Hart IJ, Munthali C, et al. Prevalence of infection with hepatitis B and C virus and coinfection with HIV in medical inpatients in Malawi. J Infect. 2008;57:72–77. doi: 10.1016/j.jinf.2008.05.004. [DOI] [PubMed] [Google Scholar]
- 4.Diop-Ndiaye H, Toure-Kane C, Etard JF, Lo G, Diaw P, Ngom-Gueye NF, et al. Hepatitis B, C seroprevalence and delta viruses in HIV-1 Senegalese patients at HAART initiation (retrospective study) J Med Virol. 2008;80:1332–1336. doi: 10.1002/jmv.21236. [DOI] [PubMed] [Google Scholar]
- 5.Lee HC, Ko NY, Lee NY, Chang CM, Ko WC. Seroprevalence of viral hepatitis and sexually transmitted disease among adults with recently diagnosed HIV infection in Southern Taiwan, 2000–2005: upsurge in hepatitis C virus infections among injection drug users. J Formos Med Assoc. 2008;107:404–411. doi: 10.1016/S0929-6646(08)60106-0. [DOI] [PubMed] [Google Scholar]
- 6.Matthews GV, Bartholomeusz A, Locarnini S, Ayres A, Sasaduesz J, Seaberg E, et al. Characteristics of drug resistant HBV in an international collaborative study of HIV-HBV-infected individuals on extended lamivudine therapy. AIDS. 2006;20:863–870. doi: 10.1097/01.aids.0000218550.85081.59. [DOI] [PubMed] [Google Scholar]
- 7.Benhamou Y, Bochet M, Thibault V, Di MV, Caumes E, Bricaire F, et al. Long-term incidence of hepatitis B virus resistance to lamivudine in human immunodeficiency virus-infected patients. Hepatology. 1999;30:1302–1306. doi: 10.1002/hep.510300525. [DOI] [PubMed] [Google Scholar]
- 8.World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: Recommendations for a public health approach. 2013 Jun;:2013. [PubMed] [Google Scholar]
- 9.Thio CL, Smeaton L, Saulynas M, Hwang H, Kumarasamy N, Flanigan T, et al. Characterization of HIV-HBV coinfeciton in a multinational HIV-infected cohort. AIDS. 2010;27:191–201. doi: 10.1097/QAD.0b013e32835a9984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Idoko J, Meloni S, Muazu M, Nimzing L, Badung B, Hawkins C, et al. Impact of hepatitis B virus infection on human immunodeficiency virus response to antiretroviral therapy in Nigeria. Clin Infect Dis. 2009;49:1268–1273. doi: 10.1086/605675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hoffmann CJ, Charalambous S, Martin DJ, Innes C, Churchyard GJ, Chaisson RE, et al. Hepatitis B virus infection and response to antiretroviral therapy (ART) in a South African ART program. Clin Infect Dis. 2008;47:1479–1485. doi: 10.1086/593104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ive P, MacLeod W, Mkumla N, Orrell C, Jentsch U, Wallis CL, et al. Low prevalence of liver disease but regional differences in HBV treatment characteristics mark HIV/HBV co-infection in a South African HIV clinical trial. PLoS One. 2013;8:e74900. doi: 10.1371/journal.pone.0074900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Khamduang W, Gaudy-Graffin C, Ngo-Giang-Huong N, Jourdain G, Moreau A, Luekamlung N, et al. Long-Term Hepatitis B Virus (HBV) Response to Lamivudine-Containing Highly Active Antiretroviral Therapy in HIV-HBV Co-Infected Patients in Thailand. PLoS ONE. 2012;7:e42184. doi: 10.1371/journal.pone.0042184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Campbell TC, Smeaton L, Kumarasamy N, Flanigan TP, Klingman KL, Firnhaber C, et al. Efficacy and safety of of three antiretroviral regimens for initial treatment of HIV-1: a randomized clinical trial in diverse multinational settings. PLoS Med. 2012;9(8):e1001290. doi: 10.1371/journal.pmed.1001290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lockman S, Hughes MD, McIntyre J, Zheng Y, Chipato T, Conradie F, et al. Antiretroviral therapies in women after single-dose nevirapine exposure. N Engl J Med. 2010;363:1499–1509. doi: 10.1056/NEJMoa0906626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Aids Do. Table for grading the severity of adult and pediatric adverse events 2009. 2009 Available at http://rsc.tech-res.com/Document/safetyandpharmacovigilance/Table_for_Grading_Severity_of_Adult_Pediatric_Adverse_Events.pdf.
- 17.Iloeje UH, Yang HI, Su J, Jen CL, You SL, Chen CJ. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology. 2006;130:678–686. doi: 10.1053/j.gastro.2005.11.016. [DOI] [PubMed] [Google Scholar]
- 18.Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology. 2009;50:661–662. doi: 10.1002/hep.23190. [DOI] [PubMed] [Google Scholar]
- 19.Idoko J, Meloni S, Muazu M, Hawkins C, Badung B, Gwamzi N, et al. Hepatitis B Virus Co-Infection Impacts Baseline HIV parameters and HAART-related Hepatotoxicity Risk in an HIV-infected Nigerian Cohort. Clinical Infectious Diseases. 2007;49:1268–1273. [Google Scholar]
- 20.Childs K, Joshi D, Byrne R, Bruce M, Carey I, Agarwal K, et al. Tenofovir-based combination therapy for HIV/HBV co-infection: factors associated with a partial HBV virological response in patients with undetectable HIV viraemia. AIDS. 2013;27:1443–1448. doi: 10.1097/QAD.0b013e32836011c2. [DOI] [PubMed] [Google Scholar]
- 21.Kang M, Hollabaugh K, Pham V, Koletar SL, Wu K, Smurzynski M, et al. Virologic and serologic outcomes of mono versus dual HBV therapy and characterization of HIV/HBV coinfection in a US cohort. J Acquir Immune Defic Syndr. 2014;66:172–180. doi: 10.1097/QAI.0000000000000149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Boyd A, Gozlan J, Maylin S, Delaugerre C, Peytavin G, Girard PM, et al. Persistent viremia in human immunodeficiency virus/hepatitis B coinfected patients undergoing long-term tenofovir: Virological and clinical implications. Hepatology. 2014;60:497–507. doi: 10.1002/hep.27182. [DOI] [PubMed] [Google Scholar]
- 23.Marcellin P, Heathcote EJ, Buti M, Gane E, De Man RA, Krastev Z, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med. 2008;359:2442–2455. doi: 10.1056/NEJMoa0802878. [DOI] [PubMed] [Google Scholar]
- 24.Chang TT, Gish RG, De Man R, Gadano A, Sollano J, Chao YC, et al. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med. 2006;354:1001–1010. doi: 10.1056/NEJMoa051285. [DOI] [PubMed] [Google Scholar]
- 25.Wong DK, Kopaniszen M, Omagari K, Tanaka Y, Fong DY, Seto WK, et al. Effect of hepatitis B virus reverse transcriptase variations on entecavir treatment response. J Infect Dis. 2014;210:701–707. doi: 10.1093/infdis/jiu133. [DOI] [PubMed] [Google Scholar]
- 26.Lai CL, Shouval D, Lok AS, Chang TT, Cheinquer H, Goodman Z, et al. Entecavir versus lamivudine for patients with HBeAg-negative chronic hepatitis B. N Engl J Med. 2006;354:1011–1020. doi: 10.1056/NEJMoa051287. [DOI] [PubMed] [Google Scholar]
- 27.Kosi L, Reiberger T, Payer BA, Grabmeier-Pfistershammer K, Strassl R, Rieger A, et al. Five-year on-treatment efficacy of lamivudine-, tenofovir- and tenofovir + emtricitabine-based HAART in HBV-HIV-coinfected patients. J Viral Hepat. 2012;19:801–810. doi: 10.1111/j.1365-2893.2012.01601.x. [DOI] [PubMed] [Google Scholar]
- 28.Matthews GV, Seaberg EC, Avihingsanon A, Bowden S, Dore GJ, Lewin SR, et al. Patterns and Causes of Suboptimal Response to Tenofovir-Based Therapy in Individuals Coinfected With HIV and Hepatitis B Virus. Clin Infect Dis. 2013;56:e87–94. doi: 10.1093/cid/cit002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kitrinos KM, Corsa A, Liu Y, Flaherty J, Snow-Lampart A, Marcellin P, et al. No detectable resistance to tenofovir disoproxil fumarate after 6 years of therapy in patients with chronic hepatitis B. Hepatology. 2014;59:434–442. doi: 10.1002/hep.26686. [DOI] [PubMed] [Google Scholar]