

Abstract
Distal radioulnar joint (DRUJ) instability is a common clinical condition but a frequently missed diagnosis. Both surgical and nonsurgical treatments are possible for chronic cases of DRUJ instability. Nonsurgical treatment can be considered as the primary therapy in less active patients, while surgery should be considered to recover bone and ligament injuries if nonsurgical treatment fails to restore forearm stability and function. The appropriate choice of treatment depends on the individual patient and specific derangement of the DRUJ
Keywords: distal radioulnar joint, instability, triangular fibrocartilage complex, surgical management
Epidemiology
The stability of the distal radioulnar joint (DRUJ) is a result of both the bony structure and the integrity of the surrounding soft tissues including the triangular fibrocartilage complex (TFCC), pronator quadratus, and interosseous membrane (Figure 1). The dorsal and palmar radioulnar ligaments are regarded as the major factors of DRUJ stability, whereas the bony structure accounts for about only 20% of the stability.1 Distal radioulnar joint instability is a common, but often misdiagnosed, clinical condition. This instability often occurs in the setting of distal radius fractures (DRFs),2,3 with incidence rates following DRFs reported to be between 10% and 19%.4 As DRFs are commonly associated with fractures of the ulnar styloid from which the TFCC originates, it is plain to see how they may cause DRUJ instability.4
Figure 1.
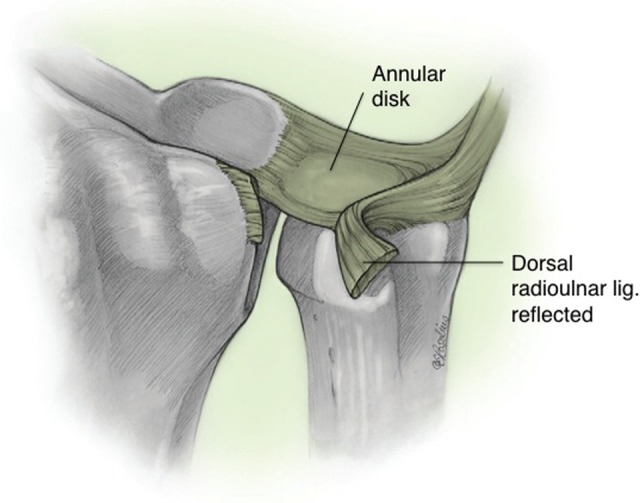
The distal radioulnar joint with the triangular fibrocartilage complex. Adapted with permission from Adams BD. Distal radioulnar joint instability. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, eds. Green’s Operative Hand Surgery. 6th ed. Philadelphia, PA: Churchill Livingstone Elsevier; 2011:524.
Diagnosis
Distal radioulnar joint instability is a commonly missed diagnosis that can be easily hidden from clinical and radiographic examinations. Clinical suspicion of DRUJ instability is strengthened with a history of wrist trauma, pain, and limited motion with supination and pronation.3 Patients may report feeling a “click” with forearm motion.6 Different physical tests for the diagnosis of DRUJ instability have been described, including the Ballottement test, radius pull test, clunk test, extensor carpi ulnaris (ECU) test, and press test.3 The Ballottement test is considered the most reliable physical examination test for DRUJ instability.6
The radiographic evaluation of DRUJ instability begins with posteroanterior (PA) and lateral radiographs of the wrist.7 In the PA view, relevant findings include widening of the distal radioulnar space as compared with the contralateral side. In the lateral view, DRUJ instability is suggested by a radioulnar distance of more than 6 mm.3,8 When conventional radiographic results are equivocal, a computed tomography (CT) scan can be of value in diagnosing DRUJ instability.9 With this modality, there are 4 methods to assess instability, including the Mino method, the congruency method, the epicenter method, and the radioulnar ratio method5 (Figure 2). The sensitivities of these methods vary from 55% to 100%,10,11 although malunions may often produce a false positive result. In particular, the Mino and congruency methods are associated with high false positive results.10,11 The epicenter method is considered the most specific method in detecting a dislocation.10 Compared with CT, a magnetic resonance imaging test has a higher sensitivity in evaluating soft tissue, rather than bony, details. While this modality has the ability to detect TFCC tears and ulnar styloid injuries, its role in evaluating DRUJ instability is still unclear.3 Arthroscopy has been utilized as a diagnostic and therapeutic intervention for the treatment of TFCC injuries, with recent literature suggesting that it may be able to detect pathology at the articular surfaces of the distal radioulnar joint.12
Figure 2.

Computed tomography (CT) methods for assessing distal radioulnar joint (DRUJ) instability. A, Radioulnar lines (Mino method). B, Congruency. C, Epicenter. D, Radioulnar ratio. Adapted with permission from Adams BD. Distal radioulnar joint instability. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, eds. Green’s Operative Hand Surgery. 6th ed. Philadelphia, PA: Churchill Livingstone Elsevier; 2011:529.
Nonsurgical Management of DRUJ Instability
Nonsurgical treatment of chronic DRUJ instability is possible in some cases. In less active patients, functional bracing can be considered as the primary therapy.13 However, this treatment can only be used as an initial therapy in more active patients, and surgery is ultimately needed if nonsurgical treatment fails to restore normal function and stability of the forearm.
Overview of Surgical Treatment Options
Surgery should be considered for DRUJ instability to recover bone and ligament injuries if nonsurgical treatment fails to restore forearm stability and function. To recover bone deformities, osteotomies of the radius,14,15 ulna,16 or, in some cases, sigmoid notch osteoplasty17 are used. Consideration is given to soft tissue injury once the bone injuries are recovered. In cases where there is no DRUJ arthritis and the sigmoid notch is intact, reconstructive procedures are considered, including techniques of extrinsic radioulnar tether,18 ulnocarpal sling,19 tenodesis procedures,20 and reconstruction of the volar and dorsal radioulnar ligaments.21 In cases where DRUJ instability is associated with ulnocarpal impaction and arthrosis, various salvage procedures are proposed.22
Darrach Procedure
The most common surgical procedure performed for DRUJ instability is the Darrach procedure23 that involves resection of the entire ulnar head.24 However, several studies have described various complications with this technique such as pain and ulnar stump clicking, loss of grip strength, loss of ulnar support, and radioulnar impingement as a result of ulnar stump instability.25,26 In their series of patients treated with the Darrach procedure, Field et al27 reported satisfactory results in only 50% of their patients, which was lower than previously published reports.28 Some authors have recommended that this technique not be used in young patients due to these complications.23,29 Tulipan et al28 used a modified Darrach procedure that involved minimal bone resection and reported good to excellent results in 91% of their patients. They reported an increase in the mean ranges of supination (from 52° preoperatively to 83° postoperatively) and pronation (from 60° preoperatively to 84° postoperatively) accompanied by a 38% increase in grip strength.28 In another study, Di Benedetto et al30 studied 18 patients over an 8-year period who underwent Darrach surgery with minimal bone resection and observed that mean supination and pronation values increased from 45° and 63°, respectively, to 82°. Furthermore, grip strength increased to 76% of the contralateral side. Of the 18 patients, 4 experienced ulnar carpal translocation. No evidence of distal ulnar instability was observed. One of the most common reasons for progressive pain after the Darrach procedure is convergence instability of the ulnar stump that is inclined to the radius.27,31–35 To alleviate this instability, several techniques have been proposed such as a transfer of the pronator quadratus origin to a more dorsal position36 and extensor carpi ulnaris and flexor carpi ulnaris tenodesis.20 However, these methods are not the best solutions. Moreover, several methods of endoprosthesis have been created to replace the ulnar head in patients undergoing Darrach surgery or another salvage procedure.24 Sauerbier et al24 observed better results when applying a prosthesis and therefore recommended an ulnar head endoprosthetic replacement instead of a soft tissue stabilization technique in recovering distal forearm instability following a Darrach resection.24
Sauvé-Kapandji Procedure
Another technique for treating chronic DRUJ instability with articular surface destruction is the Sauvé-Kapandji (S-K) technique. The S-K procedure differs from the Darrach technique in that it does not eliminate ulnar support at the wrist. Instead, the S-K technique creates joint fusion to alleviate DRUJ dislocation.25 Theoretically, the S-K technique has several advantages compared to the Darrach technique when employed in younger patients, including retention of the TFCC, ulnar head, and the origin of the ulnocarpal ligaments; a more natural force transmission pattern from the hand to the forearm; and prevention of extensor carpi ulnaris movement.37,38 This technique may also require less time for immobilization after surgery. In their review of 28 patients with DRUJ instability, Rothwell et al39 introduced a new method of the S-K procedure and reported mean pronation and supination values of more than 80° in 19 and 20 cases, respectively. Twenty-seven patients experienced pain relief.39 The S-K technique is often employed after malunited fractures of the distal radius. This technique is also indicated in cases of isolated DRUJ instability created after ligament ruptures and chronic TFCC tears. However, this technique is not without complications. These include (1) osseous or fibrous union, (2) delayed union or nonunion of the arthrodesis, and (3) painful proximal ulnar stump instability. Like the Darrach resection, complication rates in young and active patients are relatively high with this technique.39 Nakamura et al25 compared the Darrach and S-K techniques and concluded that the latter had more satisfactory results in patients with chronic DRUJ dislocation accompanied by deformity and joint damage. However, in another comparative study that evaluated radiographic results of the S-K and Darrach procedures in the rheumatoid wrist, the 2 techniques provided comparable restoration of carpal anatomy. The authors observed a decrease in the carpal height ratio (CHR) and an increase in the ulnocarpal distance ratio (UCDR) in both groups with no statistical significant differences between them.40 In another study, George et al23 compared these 2 methods in the treatment of DRUJ derangement following malunion of dorsally displaced, unstable, intra-articular fractures of the distal radius. They found no differences in both the Disabilities of the Arm, Shoulder, and Hand (DASH) score and objective outcomes. Ross et al41 introduced a new salvage procedure for a failed S-K procedure, which involved ulnar lengthening using a bone graft from the iliac crest. In this manner, the ulnar bony continuity is preserved and is followed by resection of the pseudoarthrosis with the use of a matched hemiresection interposition arthroplasty. This was conducted on 3 patients and they found no signs of instability after the surgery. The mean supination and pronation values in this series were 60° and 65°, respectively.41
Hemiresection Interposition Arthroplasty
Hemiresection interposition arthroplasty was introduced as a salvage procedure by Bowers.42 The characteristic feature of this technique is that the TFCC remains intact. The ulnar articular head is resected, while the styloid is left in place. The advantages of this procedure include shorter immobilization time and decreased risk of nonunion. Moreover, the risk of immobility and instability are decreased after this operation.43 Bain et al44 conducted a retrospective review of patients with DRUJ derangement who underwent hemiresection interposition arthroplasty after failing nonsurgical treatment. They reported pain improvement and patient satisfaction in 72% and 84% of patients, respectively. Final values for supination and pronation were 72°. In another study conducted by Ahmed et al,45 patients were exposed to matched hemiresection interposition arthroplasty and 84% reported complete resolution of pain. Moreover, grip strength and range of motion were significantly improved with final pronation and supination values of 74° and 81°, respectively. Imbriglia and Matthews43 recommended hemiresection interposition arthroplasty for cases of chronic posttraumatic dorsal subluxation of the distal ulna and for patients who are symptomatic, despite ligamentous stabilization. In their study, 17 of 23 patients showed good or excellent results with increases in the final range of motion and grip strength of 90% and 75%, respectively, compared to the contralateral side. Thirteen patients experienced complete pain relief in their series. In their cadaveric study, Sauerbier et al46 found that the Darrach technique caused more forearm instability than the hemiresection interposition technique and thus concluded that hemiresection interposition arthroplasty was superior to the Darrach technique for treatment of DRUJ arthrosis. Minami et al47 examined the results of all 3 salvage procedures for treatment of patients with osteoarthritis of the DRUJ. After a mean 10-year follow-up, they found that both the S-K and hemiresection interposition arthroplasty techniques performed better with regard to pain improvement, flexion and extension, grip strength, and overall complications when compared to the Darrach procedure. Of note, supination and pronation values improved significantly for all groups. The authors recommended the Darrach technique for elderly patients with severe osteoarthritic changes in the DRUJ, hemiresection interposition arthroplasty for patients with a reconstructible or intact TFCC, and the S-K technique for the patients with a non-reconstructible TFCC or positive ulnar variance more than 5 mm in spite of a functional TFCC.
Conclusion
Distal radioulnar joint instability is a common, but frequently missed, clinical condition that typically occurs in the setting of associated distal radius and ulnar styloid fractures. Computed tomography has emerged as a valuable tool in assessing the integrity of the DRUJ, and the roles of additional imaging modalities continue to be explored. Both surgical and nonsurgical treatments are available for chronic cases of DRUJ instability. Nonsurgical treatment can be considered as the primary therapy in less active patients, while surgery should be considered to recover bone and ligament injuries if nonsurgical treatment fails to restore forearm stability and function. Several salvage techniques have been described for DRUJ instability, including the Darrach procedure, the S-K technique, and hemiresection interposition arthroplasty. Each has its set of advantages and disadvantages, and the appropriate choice of treatment depends on the individual patient and specific derangement of the DRUJ. Further studies are warranted to compare the techniques to better elucidate their role in the treatment of DRUJ instability.
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Carlsen BT, Dennison DG, Moran SL. Acute dislocations of the distal radioulnar joint and distal ulna fractures. Hand Clin. 2010;26(4):503–516. [DOI] [PubMed] [Google Scholar]
- 2. Mulford JS, Axelrod TS. Traumatic injuries of the distal radioulnar joint. Hand Clin. 2010;26(1):155–163. [DOI] [PubMed] [Google Scholar]
- 3. Wijffels M, Brink P, Schipper I. Clinical and non-clinical aspects of distal radioulnar joint instability. Open Orthop J. 2012;6:204–210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Kazemian GH, Bakhshi H, Lilley M, et al. DRUJ instability after distal radius fracture: A comparison between cases with and without ulnar styloid fracture. Int J Surg. 2011;9(8):648–651. [DOI] [PubMed] [Google Scholar]
- 5. Squires JH, England E, Mehta K, Wissman RD. The role of imaging in diagnosing diseases of the distal radioulnar joint, triangular fibrocartilage complex, and distal ulna. AJR Am J Roentgenol. 2014;203(1):146–153. [DOI] [PubMed] [Google Scholar]
- 6. Huang JI, Hanel DP. Anatomy and biomechanics of the distal radioulnar joint. Hand Clin. 2012;28(2):157–163. [DOI] [PubMed] [Google Scholar]
- 7. Schuind F, An KN, Berglund L, et al. The distal radioulnar ligaments: a biomechanical study. J Hand Surg Am. 1991;16(6):1106–1114. [DOI] [PubMed] [Google Scholar]
- 8. Nakamura R, Horii E, Imaeda T, Tsunoda K, Nakao E. Distal radioulnar joint subluxation and dislocation diagnosed by standard roentgenography. Skeletal Radiol. 1995;24(2):91–94. [DOI] [PubMed] [Google Scholar]
- 9. Rüegger C, Schmid MR, Pfirrmann CW, Nagy L, Gilula LA, Zanetti M. Peripheral tear of the triangular fibrocartilage: depiction with MR arthrography of the distal radioulnar joint. AJR Am J Roentgenol. 2007;188(1):187–192. [DOI] [PubMed] [Google Scholar]
- 10. Chiang CC, Chang MC, Lin CF, Liu Y, Lo WH. Computerized tomography in the diagnosis ofsubluxation of the distal radioulnar joint. Zhonghua Yi Xue Za Zhi (Taipei). 1998;61(12):708–715. [PubMed] [Google Scholar]
- 11. Nakamura R, Horii E, Imaeda T, Nakao E. Criteria for diagnosing distal radioulnar joint subluxation by computed tomography. Skeletal Radiol. 1996;25(7):649–653. [DOI] [PubMed] [Google Scholar]
- 12. Atzei A. New trends in arthroscopic management of type 1-B TFCC injuries with DRUJ instability. J Hand Surg Eur Vol. 2009;34(5):582–591. [DOI] [PubMed] [Google Scholar]
- 13. Millard GM, Budoff JE, Paravic V, Noble PC. Functional bracing for distal radioulnar joint instability. J Hand Surg Am. 2002;27(6):972–977. [DOI] [PubMed] [Google Scholar]
- 14. Adams BD. Effects of radial deformity on distal radioulnar joint mechanics. J Hand Surg Am. 1993;18(3):492–498. [DOI] [PubMed] [Google Scholar]
- 15. Kihara H, Palmer AK, Werner FW, Short WH, Fortino MD. The effect of dorsally angulated distal radius fractures on distal radioulnar joint congruency and forearm rotation. J Hand Surg Am. 1996;21(1):40–47. [DOI] [PubMed] [Google Scholar]
- 16. Chidgey LK. Treatment of acute and chronic instability of the distal radio-ulnar joint. Hand Clin. 1998;14(2):297–303. [PubMed] [Google Scholar]
- 17. Wallwork NA, Bain GI. Sigmoid notch osteoplasty for chronic volar instability of the distal radioulnar joint: a case report. J Hand Surg Am. 2001;26(3):454–459. [DOI] [PubMed] [Google Scholar]
- 18. Fulkerson JP, Watson HK. Congenital anterior subluxation of the distal ulna. A case report. Clin Orthop Relat Res. 1978;(131):179–182. [PubMed] [Google Scholar]
- 19. Hui FC, Linscheid RL. Ulnotriquetral augmentation tenodesis: a reconstructive procedure for dorsal subluxation of the distal radioulnar joint. J Hand Surg Am. 1982;7(3):230–236. [DOI] [PubMed] [Google Scholar]
- 20. Breen TF, Jupiter JB. Extensor carpi ulnaris and flexor carpi ulnaris tenodesis of the unstable distal ulna. J Hand Surg Am. 1989;14(4):612–617. [DOI] [PubMed] [Google Scholar]
- 21. Adams BD, Berger RA. An anatomic reconstruction of the distal radioulnar ligaments for post traumatic distal radioulnar joint instability. J Hand Surg Am. 2002;27(2):243–251. [DOI] [PubMed] [Google Scholar]
- 22. Kakar S, Carlsen BT, Moran SL, Berger RA. The management of chronic distal radioulnar instability. Hand Clin. 2010;26(4):517–528. [DOI] [PubMed] [Google Scholar]
- 23. George MS, Kiefhaber TR, Stern PJ. The Sauve–Kapandji procedure and the Darrach procedure for distal radio-ulnar joint dysfunction after Colles’ fracture. J Hand Surg Br. 2004;29(6):608–613. [DOI] [PubMed] [Google Scholar]
- 24. Sauerbier M, Hahn ME, Berglund LJ, An KN, Berger RA. Biomechanical evaluation of the dynamic radioulnar convergence after ulnar head resection, two soft tissue stabilization methods of the distal ulna and ulnar head prosthesis implantation. Arch Orthop Trauma Surg. 2011;131(1):15–26. [DOI] [PubMed] [Google Scholar]
- 25. Nakamura R, Tsunoda K, Watanabe K, Horii E, Miura T. The Sauvé-Kapandji procedure for chronic dislocation of the distal radio-ulnar joint with destruction of the articular surface. J Hand Surg Br. 1992;17(2):127–132. [DOI] [PubMed] [Google Scholar]
- 26. Saffar P. The pathology of the long ulna: anatomy and treatment. J Hand Surg Eur Vol. 2007;32(6):608–619. [DOI] [PubMed] [Google Scholar]
- 27. Field J, Majkowski RJ, Leslie IJ. Poor results of Darrach’s procedure after wrist injuries. J Bone Joint Surg Br. 1993;75:53–57. [DOI] [PubMed] [Google Scholar]
- 28. Tulipan DJ, Eaton RG, Eberhart RE. The Darrach procedure defended, technique redefined and long-term follow-up. J Hand Surg Am. 1991;16:438–444. [DOI] [PubMed] [Google Scholar]
- 29. Ota N, Nakamura T, Iwamoto T, Sato K, Toyama Y. Radiographic parameter analysis on modified sauvé-kapandji procedure. J Wrist Surg. 2013;2(1):19–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. DiBenedetto MR, Lubbers LM, Coleman CR. Long-term results of the minimal resection Darrach procedure. J Hand Surg Am. 1991;16(3):445–450. [DOI] [PubMed] [Google Scholar]
- 31. Bell MJ, Hill RJ, McMurtry RY. Ulnar impingement syndrome. J Bone Joint Surg. 1985;67(3):126–129. [DOI] [PubMed] [Google Scholar]
- 32. Bieber EJ, Linscheid RL, Dobyns JH, Beckenbaugh RD. Failed distal ulna resections. J Hand Surg Am. 1988;13(2):193–200. [DOI] [PubMed] [Google Scholar]
- 33. Fraser KE, Diao E, Peimer CA, Sherwin FS. Comparative results of resection of the distal ulna in rheumatoid arthritis and post-traumatic conditions. J Hand Surg Br. 1999;24(6):667–670. [DOI] [PubMed] [Google Scholar]
- 34. Kleinman WB, Greenberg JA. Salvage of the failed Darrach procedure. J Hand Surg Am. 1995;20(6):951–958. [DOI] [PubMed] [Google Scholar]
- 35. Lees VC, Scheker LR. The radiological demonstration of dynamic ulnar impingement. J Hand Surg Am. 1997;22(4):448–450. [Google Scholar]
- 36. Johnson RK. Stabilization of the distal ulna by transfer of the pronator quadratus origin. Clin Orthop Relat Res. 1992;(275):130–132. [PubMed] [Google Scholar]
- 37. Carter PB, Stuart PR. The Sauve–Kapandji procedure for posttraumatic disorders of the distal radio-ulnar joint. J Bone Joint Surg. 2000;82(7):1013–1018. [DOI] [PubMed] [Google Scholar]
- 38. Lluch A. The Sauvé-Kapandji procedure: indications and tips for surgical success. Hand Clin. 2010;26(4):559–572. [DOI] [PubMed] [Google Scholar]
- 39. Rothwell AG, O’Neill L, Cragg K. Sauvé-Kapandji procedure for disorders of the distal radioulnar joint: a simplified technique. J Hand Surg Am. 1996;21(5):771–777. [DOI] [PubMed] [Google Scholar]
- 40. Kobayashi A, Futami T, Tadano I, Fujita M, Watanabe T, Moriguchi T. Radiographic comparative evaluation of the Sauve-Kapandji procedure and the Darrach procedure for rheumatoid wrist reconstruction. Mod Rheumatol. 2005;15(3):187–190. [DOI] [PubMed] [Google Scholar]
- 41. Ross M, Thomas J, Couzens G, Coleman S. Salvage of the unstable Sauve-Kapandji procedure: a new technique. Tech Hand Up Extrem Surg. 2007;11(1):87–92. [DOI] [PubMed] [Google Scholar]
- 42. Bowers WH. Distal radioulnar joint arthroplasty: the hemiresection-interposition technique. J Hand Surg Am. 1985;10(2):169–178. [DOI] [PubMed] [Google Scholar]
- 43. Imbriglia JE, Matthews D. Treatment of chronic post-traumatic dorsal subluxation of the distal ulna by hemiresection-interposition arthroplasty. J Hand Surg Am. 1993;18(5):899–907. [DOI] [PubMed] [Google Scholar]
- 44. Bain GI, Pugh DM, MacDermid JC, Roth JH. Matched hemiresection interposition arthroplasty of the distal radioulnar joint. J Hand Surg Am. 1995;20(6):944–950. [DOI] [PubMed] [Google Scholar]
- 45. Ahmed SK, Cheung JP, Fung BK, Ip WY. Long term results of matched hemiresection interposition arthroplasty for DRUJ arthritis in rheumatoid patients. Hand Surg. 2011;16(2):119–125. [DOI] [PubMed] [Google Scholar]
- 46. Sauerbier M, Fujita M, Hahn ME, Neale PG, Berger RA. The dynamic radioulnar convergence of the Darrach procedure and the ulnar head hemiresection interposition arthroplasty: a biomechanical study. J Hand Surg Br. 2002;27(4):307–316. [DOI] [PubMed] [Google Scholar]
- 47. Minami A, Iwasaki N, Ishikawa J, Suenaga N, Yasuda K, Kato H. Treatments of osteoarthritis of the distal radioulnar joint: long-term results of three procedures. Hand Surg. 2005;10(2-3):243–248. [DOI] [PubMed] [Google Scholar]