

Abstract
Objective
The objective of this meta-analysis is to estimate the pooled prevalence of suicidal ideation and suicide attempts in the general population of Mainland China.
Methods
A systematic literature search was conducted via the following databases: PubMed, PsycINFO, MEDLINE, China Journals Full-Text Databases, Chongqing VIP database for Chinese Technical Periodicals and Wan Fang Data. Statistical analysis used the Comprehensive Meta-Analysis program.
Results
Eight studies met the inclusion criteria for the analysis; five reported on the prevalence of suicidal ideation and seven on that of suicide attempts. The estimated lifetime prevalence figures of suicidal ideation and suicide attempts were 3.9% (95% Confidence interval [CI]: 2.5%–6.0%) and 0.8% (95% CI: 0.7%–0.9%), respectively. The estimated female-male ratio for lifetime prevalence of suicidal ideation and suicide attempts was 1.7 and 2.2, respectively. Only the difference of suicide attempts between the two genders was statistically significant.
Conclusion
This was the first meta-analysis of the prevalence of suicidal ideation and suicide attempts in the general population of Mainland China. The pooled lifetime prevalence of both suicidal ideation and suicide attempts are relatively low; however, caution is required when assessing these self-report data. Women had a modestly higher prevalence for suicide attempts than men. The frequency for suicidal ideation and suicide attempts in urban regions was similar to those in rural areas.
Keywords: Suicide attempts, suicidal ideation, prevalence, meta-analysis, China
Introduction
Suicide has been a major public health challenge for many years in China. It is estimated that during the period of 1995–1999 the annual suicide rate was 23/10,000 and there were 287,000 suicide deaths/year in China [1]. Suicide is the fifth most common cause of death in China [2] accounting for 43.6% of all suicide cases worldwide [3]. Even as suicide rates have apparently decreased substantially during the past few years [4], numbers alone underscore China’s heavy contribution to the world’s overall suicide burden, especially for women.
Suicidal thoughts and plans (ideation; SI) and suicide attempts (SA) often may be the prodrome for later suicide [5–8], and by themselves indicate great personal distress and psychological burden. It is crucial to understand the patterns of SI/SA for implementing effective suicide prevention measures. In developed countries the lifetime prevalence of SI/SA are approximately 3.0–15.9% and 0.5–5%, respectively with women at higher risk than men [9]. These findings may not be applicable to the Chinese population due to the different political, economic and socio-cultural contexts.
Several studies have examined the patterns of SI/SA in China. The figures varied considerably across studies. The estimated lifetime prevalence of SI and SA ranged between 2.3% [10] and 23.6% [11] and between 0.5% [12] and 1.0% [10], respectively.
A systematic review on the prevalence of suicidality in Chinese aging population has been published [13]; the lifetime prevalence of SI among community-dwelling older adults ranged between 2.2% and 16.7% and that of SA among older adults with psychiatric disorders was between 25% and 60%. However, there has been no systematic review on this subject in the general adult population of China. This paper is a systematic, quantitative meta-analysis that targeted the prevalence of SI and SA in the general adult population in China.
Methods
Search strategy
Studies on the prevalence of SI and SA in general Chinese population were retrieved through a search of major electronic databases. Comprehensive literature search was conducted in the following databases: PubMed (1979–2013), Medline (1946–2013), PsycINFO (1806–2013), China Journals Full-Text Databases (1915–2013), Chongqing VIP database for Chinese Technical Periodicals (1989–2013) and WanFang Data using the terms ‘suicide’, ‘suicidality’, ‘suicide attempts’, ‘suicidal idea’, ‘suicidal ideation’, ‘self-destruction’, ‘self-harm’, ‘self-inflicted death’, ‘suicide morbidity’, ‘prevalence’, ‘epidemiology’, ‘cross-sectional survey’ and ‘China’, ‘Chinese’ and ‘Chinese general population’. Duplicates were removed using Endnote X5. Two authors (CXL and ZBL) independently screened the papers by reviewing titles and abstracts. Then full texts of potentially relevant papers were downloaded for a second round of screening. Papers eligible for inclusion were identified according to pre-defined inclusion and exclusion criteria detailed below. A third author (XYT) was consulted when the two authors disagreed about the inclusion of a paper and a consensus decision was made after a discussion.
Inclusion and exclusion criteria
Studies included were: (i) cross-sectional surveys on prevalence of SI and SA in community-dwelling general populations in mainland China, either lifetime or one-year prevalence; (ii) the age of subjects was 15 years or above; (iii) employing clear definitions of SI and SA; (iv) having information on prevalence rates and sample size; and (v) full texts either written in English or Chinese. Studies focused on subjects with a limited age range (e.g., youth or elderly) or in special settings (e.g., hospitals or schools), were excluded.
Data extraction
Data extraction was independently conducted by two of the authors (CXL and ZBL). Relevant variables from eligible studies included the name of first author, the year of publication, region of the studies, sampling methods, sample size, number of cases and the lifetime and one-year prevalence of SI and SA for the whole sample and different demographic subgroups.
Following the methodology in earlier studies [14, 15], we evaluated the quality of reports in this review with the 22-item Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) [16]. This form consists of 22 criteria addressing key elements of methods, presentation and interpretation of the results. One point is given for each item. Studies with a score of 11 or less were classified as ‘poor quality’ [14].
Statistical analysis
The data were analyzed using the Comprehensive Meta Analysis software, Version 2 (Biosta, Inc. USA). Rates were logit transformed before pooling [17]. Forest plots were drawn to visualize the combined prevalence and extent of heterogeneity of studies. The I2 statistic was used to assess the heterogeneity across studies. When I2 statistic was less than 50% and the p-value for the test of heterogeneity was ≧ 0.1, studies were considered homogenous and a fixed effects meta-analysis was used to estimate the overall prevalence. Otherwise, a random effects meta-analysis was used [18]. When heterogeneity was present, sensitivity analysis and subgroup analysis were used to explore the potential reasons for heterogeneity.
Results
Studies identified
As shown in Figure 1, the literature search has identified 2,574 potential papers including duplicates; 456 duplicates were removed using Endnote X5. Having reviewed the titles and abstracts, further 2,088 papers were excluded and 30 papers were identified for detailed examination. Finally, 8 papers were included in the meta-analysis [10–12, 19–23]. Five papers reported the prevalence of SI and seven studies reported that of SA. Details of the studies are shown in Table 1.
FIGURE 1.

Flowchart for the Selection of Studies
TABLE 1.
Summary of selected studies on suicidal ideations and suicide attempts
| Study | Region | Years study conducted | Sampling method | Age (years) | Sample size | Response rate (%) | Cases with suicidal behavior | |
|---|---|---|---|---|---|---|---|---|
| Lifetime | One year | |||||||
| Ma WJ 2010 | mixed | 2007 | PPS | 16 above | 6670 | 99.3 | - | SAa: 52 |
| Sun XL 2010 | mixed | 2004–2005 | M, C | 18 above | 24000 | 86.3 | SAa: 170 | SAa: 37 |
| Yao J 2010 | Mixed | 2005–2006 | PPS | 15 above | 5060 | 99.5 | SIb: 304; SA: 40 | - |
| Feng SS 2004 | rural | 2003 | S, R | 18 above | 946 | 90.2 | SIc: 201 | SIc: 114 |
| Wang WQ 2012 | Mixed | 2010 | M, C | 18 above | 12051 | 89.2 | SAa: 59 | SAa: 9 |
| Lee S 2007 | urban | 2001–2002 | M, C | 18 above | 5201 | 74.6 | SIb: 160; SAa: 49 | - |
| Ma X 2009 | mixed | 2003 | M, S | 15 above | 6251 | 94.8 | SIb: 136; SAa: 59 | - |
| Wang ZZ 2013 | Mixed | 2011–2012 | PPS | 18 above | 5526 | 86.7 | SIb: 252, SAa: 37 | SIb: 94, SAa: 9 |
Sample method: M: multistage sampling; C: cluster sampling, S: stratified sampling, R: random sampling; PPS: sampling with probability proportional to size. SI: suicidal ideation, SA: suicide attempt.
Respondents answering “yes” to “have you ever attempted suicide?”.
Respondents answering “yes” to “have you ever seriously thought about committing suicide?”.
Respondents answering “yes” to “have you ever thought of ending your life?”.
Evaluation of the quality of the studies
The mean ± standard deviation score for the papers based on the STROBE items was 19.1±1.6 (range: 17 to 22). Common problems were inadequate description of the sample size estimation (5 reports) and that of potential sources of bias (6 reports).
Pooled prevalence of suicidal behaviors and the heterogeneity of studies Suicidal ideation
As shown in Table 1, five studies reported the lifetime prevalence of SI. Four of them [10, 19, 20, 23] used the same question on SI [24] (“Have you ever seriously thought about committing suicide?”) with the prevalence being between 2.3% and 6.0%. Using a broader question (“Have you ever thought of terminating your life?”) the lifetime prevalence of SI was 23.6% (Feng, 2004). Given the different nature of the questions on SI and the outlier result of Feng, we excluded it in further analyses for the pooled prevalence estimates of SI.
There was wide variation in lifetime prevalence of SI (Figure 2). The heterogeneity was large (I2=97.5%), therefore a random effect model was used to pool rates of the four studies. The lifetime prevalence of SI in the pooled sample of 20,949 was 3.9% (95% CI, 2.5%–6.0%).
FIGURE 2.
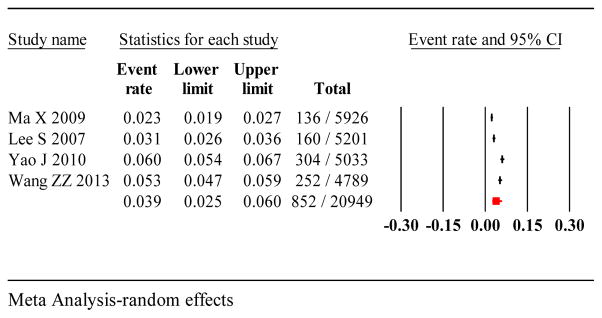
Forest plot of lifetime prevalence of suicidal ideation
Suicide attempts
The heterogeneity in lifetime prevalence estimates of SA was less than that in SI (I2=60.9%). As shown in Figure 3, using the random effect model, the pooled lifetime prevalence of SA was 0.8% (95% CI: 0.7%–0.9%). Four studies reported the one-year prevalence of SA and the variation between these studies was also wide (I2=95.8%). However, sensitivity analysis could not identify factors that could exclude any study. Results of the studies were pooled using the random effect model: the one-year prevalence of SA was 0.2% (95% CI: 0.1%–0.6%) (Figure 4).
FIGURE 3.
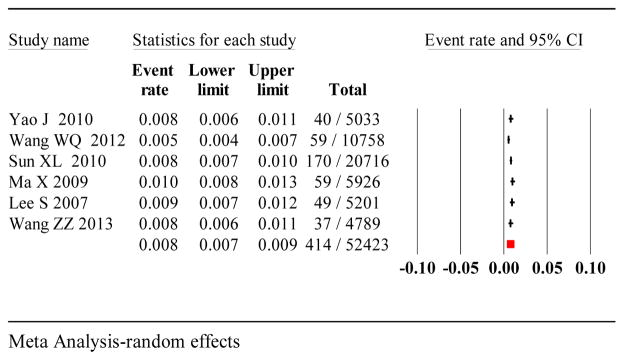
Forest plot of lifetime prevalence of suicide attempts
FIGURE 4.
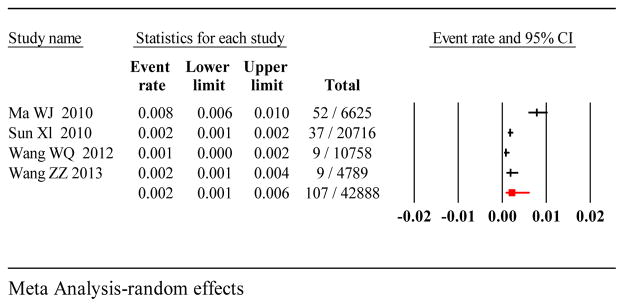
Forest plot of one-year prevalence of suicide attempts
Subgroup analysis
The lifetime prevalence of SI in women was 1.7-fold the prevalence in men (4.9% vs. 2.8%), although this apparent difference was not statistically significant in light of the large degree of variability among the studies. The lifetime prevalence of SA in women was significantly greater than that in men (1.1% vs. 0.5%), approximately 2.2 times the rates in men (p<0.05) (table 2).
TABLE 2.
Overall and subgroup prevalence of suicidal ideations and suicide attempt
| Subgroup | Number of studies | Number of cases | Sample size | Prevalence (%) | 95%CI | I2 (P value) | Q value (p value) |
|---|---|---|---|---|---|---|---|
| Lifetime prevalence of suicidal ideation | |||||||
| Female | 4 | 582 | 11415 | 4.9 | 3.2–7.5 | 96.8 (<0.001) | 3.3 (0.06) |
| Male | 4 | 285 | 9859 | 2.8 | 1.8–4.3 | 90.7 (<0.001) | |
| Urban | 4 | 432 | 12114 | 3.3 | 2.0–5.7 | 97.6 (<0.001) | 0.3 (0.5) |
| rural | 3 | 415 | 8835 | 4.3 | 2.3–7.8 | 93.6 (<0.001) | |
| Lifetime prevalence of suicide attempts | |||||||
| Female | 5 | 275 | 24775 | 1.1 | 0.8–1.5 | 81.4 (<0.001) | 12.9 (0.0001) |
| Male | 5 | 115 | 23184 | 0.5 | 0.4–0.7 | 58.2 (0.003) | |
| Urban | 5 | 152 | 22067 | 0.7 | 0.5–0.9 | 74.5 (0.003) | 2.3 (0.1) |
| rural | 4 | 234 | 25567 | 0.9 | 0.8–1.0 | 30.9 (0.2)* | |
CI: confidence interval, I2: heterogeneity coefficient.
the pooled prevalence was computed using fixed-effect model. Other prevalence was computed using random-effect model.
The lifetime prevalence of SI among rural populations was 1.3 fold that of their urban counterparts (4.3% vs. 3.3%). The lifetime prevalence of SA in rural populations was homogeneous (I2=30.9%). The result was pooled using fixed effect model resulting a prevalence of 0.9% in rural population, which was higher than that reported from urban areas (0.7%). The differences in terms of lifetime prevalence of SI and SA were not statistically significant between rural and urban areas.
Discussion
Eight studies were eligible for inclusion in a meta-analysis on the prevalence of SI and SA in the Chinese general population; five focused on prevalence of SI and seven on SA. These data should be helpful for policy makers who are responsible for suicide prevention in China.
The pooled lifetime prevalence of SI and SA was 3.9% and 0.8%, respectively. These figures are within the range of SI and SA in general populations of other Asian countries (SI: 1.7%–15.2%; SA: 0.4%–4.2%) [25–29], but lower than those reported from Western countries (SI: 10%–20%; SA: 2%–8%) [30–33]. A systematic review examining suicide between 1997 and 2007 showed that the lifetime prevalence of SI among adults varied from 3.1% to 56.0% and that of SA was between 0.9% and 19.5% [34], indicating the prevalence of SI and SA in China are at a low level.
In traditional Chinese culture, suicide is heavily stigmatized; thus it is shameful to report suicide behaviors, which may explain the low prevalence found in China [10]. Thus, while these are the most rigorous studies, to date, caution must be exercised when considering these results. They likely serve as a floor rather than a ceiling for judging rates of SI and SA in China. At the same time, the included studies were conducted during the past decade, when China’s GDP increased from 10.9 trillion to 40.1 trillion Chinese Yuan [35]. These rapid socioeconomic changes are substantially improving living conditions across China, including many rural regions, which in turn may influence the context in which suicidal distress occurs. Better economic circumstances may have lessened financial distress in families; however, the impact of high levels of internal migration could have served to exacerbate other stressors. Given the large population of China, prevalence figures for SI and SA of 3.9% and 0.8%, respectively, indicate approximately 50 million and 10 million people suffer a level of distress that involves thought and actions to kill oneself. Despite any welcome reductions in the suicide rates in China, these figures underscore that preventing suicide behaviors remains a major public health challenge.
In our analyses, rural dwellers were not more likely to have SI and SA than urban ones. Phillips and colleagues [1, 2] have suggested that the the relatively low income and living standards, and limited access to social and health services in rural areas may contribute to the oft noted greater prevalence of suicide in rural regions. However, given the results of these community surveys, difference in fatal outcomes from attempts may more likely reflect the more common use of highly toxic pesticides when making an attempt. That is, the case fatality percent (or rate) of rural attempts is higher than urban counterparts because of readily accessible methods. It is highly plausible that the falling suicide described by Wang et al [4] reflects relatively recent efforts to decrease the availability of first generation organophosphate pesticides, rather than a specific decrease in attempts (Caine 2013). Determining whether this premise is correct will require future study.
Another factor potentially contributing to declining suicide rate in China involves its rapid urbanization. The proportion of the Chinese rural population has decreased from 79.4% to 69.7% [1, 35] during the past decade, with access to better work, education, and often, health services. Moreover, internal migrant workers in China also number beyond 200 million; while they retain their rural hukou and residence, with many of their family members left behind, they pump substantial income from cities to support their home communities. Throughout the world, urban areas generally experience lower suicide rates than rural regions in the same countries.
The ratio of estimated suicide rates in rural and urban areas varied between 1.5 and 2.5 in China [4]. However, in our meta-analysis, the corresponding ratios of SI and SA were both 1.3. In addition to the impact of means selection on the case fatality percent, another explanation for the relatively low ratio of pooled SI and SA rates between rural and urban areas in the meta-analysis may be selection bias; rural areas in the majority of the studies were in the immediate vicinity of major cities like Beijing, Guangdong and Xiamen, and as such are probably far more affluent than most of rural China. This may have the effect of lowering the prevalence of suicide-related behaviors in the study regions.
Subgroup analysis revealed that the prevalence of SI in women was higher than that in men although the difference did not reach significant level, which is in line with most [30, 36, 37] but not all studies (Hintikka et al., 2001; Renberg, 2001). We also found that women’s lifetime prevalence of SA was significantly higher than that of men’s, which is consistent with earlier findings on suicide patterns in China [1]. Of note, the report from Wang et al [4] suggests that men now exceed women in their suicide rates. Women around the world have more frequent attempts than men; it is uncertain whether women have more frequent attempts than men in China for specific cultural reasons, or whether we are seeing common gender-specific behaviors across culture.
There are several limitations of the study, beyond others previously noted. The number of the included studies was small; five for SI and seven for SA. Moreover, no studies reported the one-year prevalence of SI by sub-groups, thus subgroup analysis of SI could not be conducted. In addition, there is a potential measurement bias in the pooled prevalence of SI due to inconsistent SI definitions in the included studies. One SI definition - “ever seriously thought about committing suicide”, is more stringent than the other one - “ever thought of ending your life”, which may underestimate the pooled SI prevalence. Publication bias was not assessed as a minimum of 10 studies are required for such analysis [14].
Conclusions
This is the first meta-analysis of the prevalence of SI and SA in Chinese general population. The lifetime prevalence figures of SI and SA are lower than those reported from Western countries. Prevalence of SA in women was higher than that in men, but the risk for SI and SA was similar between urban and rural areas.
Acknowledgments
Dr. Caine is supported, in part, by PHS NIH grant D43 TW009101 and PHS CDC grant R49 CE002093.
Footnotes
Conflict of Interest
None.
References
- 1.Phillips MR, Li X, Zhang Y. Suicide rates in China, 1995–99. Lancet. 2002;359(9309):835–840. doi: 10.1016/S0140-6736(02)07954-0. [DOI] [PubMed] [Google Scholar]
- 2.Phillips MR, Yang G, Zhang Y, Wang L, Ji H, Zhou M. Risk factors for suicide in China: a national case-control psychological autopsy study. Lancet. 2002;360(9347):1728–1736. doi: 10.1016/S0140-6736(02)11681-3. [DOI] [PubMed] [Google Scholar]
- 3.Phillips MR, Liu H, Zhang Y. Suicide and social change in China. Culture, Medicine and Psychiatry. 1999;23(1):25–50. doi: 10.1023/a:1005462530658. [DOI] [PubMed] [Google Scholar]
- 4.Wang CW, Chan CL, Yip PS. Suicide rates in China from 2002 to 2011: an update. Soc Psychiatry Psychiatr Epidemiol. 2013 doi: 10.1007/s00127-013-0789-5. [DOI] [PubMed] [Google Scholar]
- 5.Kessler RC, Berglund P, Borges G, Nock M, Wang PS. Trends in suicide ideation, plans, gestures, and attempts in the United States, 1990–1992 to 2001–2003. JAMA. 2005;293(20):2487–2495. doi: 10.1001/jama.293.20.2487. [DOI] [PubMed] [Google Scholar]
- 6.Harkavy-Friedman JM, Restifo K, Malaspina D, Kaufmann CA, Amador XF, Yale SA, Gorman JM. Suicidal behavior in schizophrenia: characteristics of individuals who had and had not attempted suicide. American Journal of Psychiatry. 1999;156(8):1276–1278. doi: 10.1176/ajp.156.8.1276. [DOI] [PubMed] [Google Scholar]
- 7.Drake R, Whitaker A, Gates C, Cotton P. Suicide among schizophrenics: A review. Comprehensive Psychiatry. 1985;26(1):90–100. doi: 10.1016/0010-440x(85)90053-7. [DOI] [PubMed] [Google Scholar]
- 8.De Leo D, Cerin E, Spathonis K, Burgis S. Lifetime risk of suicide ideation and attempts in an Australian community: prevalence, suicidal process, and help-seeking behaviour. Journal of Affective Disorders. 2005;86(2–3):215–224. doi: 10.1016/j.jad.2005.02.001. [DOI] [PubMed] [Google Scholar]
- 9.Nock MK, Borges G, Bromet EJ, Alonso J, Angermeyer M, Beautrais A, Bruffaerts R, Chiu WT, de Girolamo G, Gluzman S, de Graaf R, Gureje O, Haro JM, Huang Y, Karam E, Kessler RC, Lepine JP, Levinson D, Medina-Mora ME, Ono Y, Posada-Villa J, Williams D. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry. 2008;192(2):98–105. doi: 10.1192/bjp.bp.107.040113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ma X, Xiang YT, Cai ZJ, Li SR, Xiang YQ, Guo HL, Hou YZ, Li ZB, Li ZJ, Tao YF, Dang WM, Wu XM, Deng J, Chan SS, Ungvari GS, Chiu HF. Lifetime prevalence of suicidal ideation, suicide plans and attempts in rural and urban regions of Beijing, China. Australian and New Zealand Journal of Psychiatry. 2009;43(2):158–166. doi: 10.1080/00048670802607170. [DOI] [PubMed] [Google Scholar]
- 11.Feng SS. Liu Yang City, editor. Prevalence and risk factors of suicidal ideation in rural population from Yong’an town. Hu Nan: Central South Universtiy; 2004. in Chinese. [Google Scholar]
- 12.Wang WQ, Ding LJ, Wen C, Liao ZH, Wu SY. Attempters suicide in people aged 18 and older in Xiamen City. (in chinese) Chinese Mental Health Journal. 2012;26:332–336. [Google Scholar]
- 13.Simon M, Chang ES, Zeng P, Dong X. Prevalence of suicidal ideation, attempts, and completed suicide rate in Chinese aging populations: a systematic review. Archives of Gerontology and Geriatrics. 2013;57(3):250–256. doi: 10.1016/j.archger.2013.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wan YM, Hu Q, Li T, Jiang LJ, Du YS, Feng L, Wong JC-M, Li CB. Prevalence of autism spectrum disorders among children in China: a systematic review. Shanghai Archives of Psychiatry. 2013;25:70–80. doi: 10.3969/j.issn.1002-0829.2013.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Qian J, Hu Q, Wan YM, Li T, Wu MD, Ren ZQ, Yu DH. Prevalence of eating disorders in the general population :a systematic review. Shanghai Archives of Psychiatry. 2013;25:212–223. doi: 10.3969/j.issn.1002-0829.2013.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. doi: 10.1371/journal.pmed.0040296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Williams JG, Higgins JP, Brayne CE. Systematic review of prevalence studies of autism spectrum disorders. Archives of Disease in Childhood. 2006;91(1):8–15. doi: 10.1136/adc.2004.062083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yao J, Huang YQ, Yuan Y, Lu J, Gao CQ, Dang WM, Luo C. The prevalence and related factors of suicide in persons aged 15 or over in Kuming City. (in Chinese) Chinese Mental Health Journal. 2010;24:536–540. [Google Scholar]
- 20.Wang ZZ, Qin Y, Zhang YH, Zhang B, Li L, Li T, Ding L. Prevalence and correlated factors of lifetime suicidal ideaition in adults in Ningxia, China. (in Chinese) Shanghai Archives of Psychiatry. 2013;25:287–295. doi: 10.3969/j.issn.1002-0829.2013.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sun XL, Li KQ, Cui LJ, Jiang QP, Gao LH, Liu YQ, Han YC, Yang LH, Li JF, Yan BP, Zhang Y, Lv H. The prevalence of suicide attempters in people aged 18 and older in Hebei Province. (in Chinese) Chinese Mental Health Journal. 2010;24:362–365. [Google Scholar]
- 22.Ma WJ, Yan QH, Xu YJ, Xu XJ, Cai QM, Xu HF, Song XL, Nie SP. Features on suicide attempts and its influencing factors among residents in Guangdong. (in Chinese) Chinese Journal of epidemiology. 2010;31:413–416. [PubMed] [Google Scholar]
- 23.Lee S, Fung SC, Tsang A, Liu ZR, Huang YQ, He YL, Zhang MY, Shen YC, Nock MK, Kessler RC. Lifetime prevalence of suicide ideation, plan, and attempt in metropolitan China. Acta Psychiatrica Scandinavica. 2007;116(6):429–437. doi: 10.1111/j.1600-0447.2007.01064.x. [DOI] [PubMed] [Google Scholar]
- 24.Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56(7):617–626. doi: 10.1001/archpsyc.56.7.617. [DOI] [PubMed] [Google Scholar]
- 25.Tran Thi Thanh H, Tran TN, Jiang GX, Leenaars A, Wasserman D. Life time suicidal thoughts in an urban community in Hanoi, Vietnam. BMC Public Health. 2006;6:76. doi: 10.1186/1471-2458-6-76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ono Y, Kawakami N, Nakane Y, Nakamura Y, Tachimori H, Iwata N, Uda H, Nakane H, Watanabe M, Naganuma Y, Furukawa TA, Hata Y, Kobayashi M, Miyake Y, Tajima M, Takeshima T, Kikkawa T. Prevalence of and risk factors for suicide-related outcomes in the World Health Organization World Mental Health Surveys Japan. Psychiatry and Clinical Neurosciences. 2008;62(4):442–449. doi: 10.1111/j.1440-1819.2008.01823.x. [DOI] [PubMed] [Google Scholar]
- 27.Maniam T, Marhani M, Firdaus M, Kadir AB, Mazni MJ, Azizul A, Salina AA, Fadzillah AR, Nurashikin I, Ang KT, Jasvindar K, Noor Ani A. Risk factors for suicidal ideation, plans and attempts in Malaysia - Results of an epidemiological survey. Compr Psychiatry. 2013:121–125. doi: 10.1016/j.comppsych.2013.08.004. [DOI] [PubMed] [Google Scholar]
- 28.Jeon HJ, Lee JY, Lee YM, Hong JP, Won SH, Cho SJ, Kim JY, Chang SM, Lee D, Lee HW, Cho MJ. Lifetime prevalence and correlates of suicidal ideation, plan, and single and multiple attempts in a Korean nationwide study. Journal of Nervous and Mental Disease. 2010;198(9):643–646. doi: 10.1097/NMD.0b013e3181ef3ecf. [DOI] [PubMed] [Google Scholar]
- 29.Bertolote JM, Fleischmann A, De Leo D, Bolhari J, Botega N, De Silva D, Tran Thi Thanh H, Phillips M, Schlebusch L, Varnik A, Vijayakumar L, Wasserman D. Suicide attempts, plans, and ideation in culturally diverse sites: the WHO SUPRE-MISS community survey. Psychological Medicine. 2005;35(10):1457–1465. doi: 10.1017/S0033291705005404. [DOI] [PubMed] [Google Scholar]
- 30.Weissman MM, Bland RC, Canino GJ, Greenwald S, Hwu HG, Joyce PR, Karam EG, Lee CK, Lellouch J, Lepine JP, Newman SC, Rubio-Stipec M, Wells JE, Wickramaratne PJ, Wittchen HU, Yeh EK. Prevalence of suicide ideation and suicide attempts in nine countries. Psychological Medicine. 1999;29(1):9–17. doi: 10.1017/s0033291798007867. [DOI] [PubMed] [Google Scholar]
- 31.Ten Have M, van Dorsselaer S, de Graaf R. Prevalence and risk factors for first onset of suicidal behaviors in the Netherlands Mental Health Survey and Incidence Study-2. Journal of Affective Disorders. 2013;147(1–3):205–211. doi: 10.1016/j.jad.2012.11.005. [DOI] [PubMed] [Google Scholar]
- 32.Nicoli M, Bouchez S, Nieto I, Gasquet I, Kovess V, Lepine JP. Prevalence and risk factors for suicide ideation, plans and attempts in the French general population: results from the ESEMeD study. Encephale. 2012;38(4):296–303. doi: 10.1016/j.encep.2011.02.006. [DOI] [PubMed] [Google Scholar]
- 33.Aschan L, Goodwin L, Cross S, Moran P, Hotopf M, Hatch SL. Suicidal behaviours in South East London: prevalence, risk factors and the role of socio-economic status. Journal of Affective Disorders. 2013;150(2):441–449. doi: 10.1016/j.jad.2013.04.037. [DOI] [PubMed] [Google Scholar]
- 34.Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, Lee S. Suicide and Suicidal Behavior. Epidemiol Rev. 2008;30:133–154. doi: 10.1093/epirev/mxn002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.China NBoSo. China statistical yearbook 2011. Beijing: China Statistics Press; 2012. [Google Scholar]
- 36.Maniam T, Marhani M, Firdaus M, Kadir AB, Mazni MJ, Azizul A, Salina AA, Fadzillah AR, Nurashikin I, Ang KT, Jasvindar K, Noor Ani A. Risk factors for suicidal ideation, plans and attempts in Malaysia - Results of an epidemiological survey. Compr Psychiatry. 2013 doi: 10.1016/j.comppsych.2013.08.004. [DOI] [PubMed] [Google Scholar]
- 37.Botega NJ, Barros MB, Oliveira HB, Dalgalarrondo P, Marin-Leon L. Suicidal behavior in the community: prevalence and factors associated with suicidal ideation. Rev Bras Psiquiatr. 2005;27(1):45–53. doi: 10.1590/s1516-44462005000100011. [DOI] [PubMed] [Google Scholar]