

Abstract
Background
Autopsy studies of HIV/AIDS-related hospital deaths in sub-Saharan Africa reveal frequent failure of pre-mortem diagnosis of tuberculosis (TB), which is found in 34–64 % of adult cadavers. We determined the overall prevalence and predictors of TB among consecutive unselected HIV-positive adults requiring acute hospital admission and the comparative diagnostic yield obtained by screening urine and sputum samples obtained on day 1 of admission with Xpert MTB/RIF (Xpert).
Methods
To determine overall TB prevalence accurately, comprehensive clinical sampling (sputum, urine, blood plus other relevant samples) was done and TB was defined by detection of Mycobacterium tuberculosis in any sample using Xpert and/or mycobacterial liquid culture. To evaluate a rapid screening strategy, we compared the diagnostic yield of Xpert testing sputum samples and urine samples obtained with assistance from a respiratory study nurse in the first 24 h of admission.
Results
Unselected HIV-positive acute adult new medical admissions (n = 427) who were not receiving TB treatment were enrolled irrespective of clinical presentation or symptom profile. From 2,391 cultures and Xpert tests done (mean, 5.6 tests/patient) on 1,745 samples (mean, 4.1 samples/patient), TB was diagnosed in 139 patients (median CD4 cell count, 80 cells/μL). TB prevalence was very high (32.6 %; 95 % CI, 28.1–37.2 %; 139/427). However, patient symptoms and risk factors were poorly predictive for TB. Overall, ≥1 non-respiratory sample(s) tested positive in 115/139 (83 %) of all TB cases, including positive blood cultures in 41/139 (29.5 %) of TB cases. In the first 24 h of admission, sputum (spot and/or induced samples) and urine were obtainable from 37.0 % and 99.5 % of patients, respectively (P <0.001). From these, the proportions of total TB cases (n = 139) that were diagnosed by Xpert testing sputum, urine or both sputum and urine combined within the first 24 h were 39/139 (28.1 %), 89/139 (64.0 %) and 108/139 (77.7 %) cases, respectively (P <0.001).
Conclusions
The very high prevalence of active TB and its non-specific presentation strongly suggest the need for routine microbiological screening for TB in all HIV-positive medical admissions in high-burden settings. The incremental diagnostic yield from Xpert testing urine was very high and this strategy might be used to rapidly screen new admissions, especially if sputum is difficult to obtain.
Keywords: Tuberculosis, Pulmonary, Extrapulmonary, HIV, Diagnosis, Screening, Urine, Xpert, Africa
Background
Tuberculosis (TB) is the leading cause of HIV/AIDS-related mortality [1], accounting for approximately 37 % of HIV/AIDS-related adult facility-based deaths in resource-limited settings [2]. Most of these deaths occur in sub-Saharan Africa where multiple hospital post-mortem studies conducted over the past 20 years have shown that between 34 % and 64 % of HIV-positive patients had TB at the time of death [2–7]. Disease at autopsy was predominantly disseminated and frequently remained undetected pre-mortem [2], reflecting failure of existing approaches to screening and TB diagnosis in HIV-infected medical in-patients.
The global TB control strategy defined in the mid-1990s was based on passive detection of sputum smear-positive pulmonary TB (PTB) in patients presenting with chronic cough [8]. However, in HIV-infected patients with TB and advanced immunodeficiency, chronic cough is less frequent, clinical presentation is non-specific, sputum smears are often negative and extrapulmonary TB (EPTB) is common [9, 10]. We therefore hypothesized that all HIV-positive patients requiring medical admission to hospitals in sub-Saharan Africa might warrant systematic routine microbiological investigation for TB regardless of clinical presentation. Second, we hypothesized that useful incremental diagnostic yield might be gained from additional testing of a non-respiratory sample such as urine, which is easier to obtain than sputum.
The advent of semi-automated rapid molecular tests provides new effective means of diagnosing HIV-associated TB. The Xpert MTB/RIF (Xpert) assay was endorsed by the World Health Organization (WHO) in 2010 for diagnosis of TB from sputum [11] and guidelines were updated in 2013 to include TB diagnosis from a range of non-respiratory samples, including cerebrospinal fluid and tissue needle aspirates/biopsies [12]. Endorsement was not given for testing other sample types due either to low sensitivity (pleural fluid) or for sample types for which there were insufficient data (stool, urine and blood). Importantly, however, assay specificity was found to be uniformly high regardless of sample type [12–14]. Moreover, two studies using Xpert to test urine samples from HIV-infected patients with advanced immunodeficiency each reported very promising results with high specificity (98 % and 100 %) and useful diagnostic yield, especially among in-patients [15, 16].
The present study conducted in a South African district hospital first aimed to accurately determine the prevalence and predictors of microbiologically confirmed TB among unselected HIV-positive medical admissions using microbiological screening. We then planned to use these data to define which patient sub-groups were at highest risk of TB and might warrant routine microbiological investigation at the time of hospital admission. Finally, with the ultimate aim of defining an effective rapid microbiological screening strategy on the first day of hospital admission among unselected HIV-positive admissions, we compared the diagnostic yield (proportions of total diagnoses) that could be made from rapid testing sputum and urine samples obtained in the 24-h period following admission using Xpert MTB/RIF.
Methods
Setting and patients
A prospective observational study was conducted at GF Jooste Hospital in Cape Town, South Africa. This 200-bed adult district hospital serves township communities of around 1.3 million people and with high HIV seroprevalence. This pre-defined study protocol was approved by the human research ethics committees of the University of Cape Town, South Africa, and the London School of Hygiene & Tropical Medicine, UK. Patients provided written informed consent in their first language.
Adult patients aged ≥18 years were recruited on 4 days of each week from both male and female medical wards. On recruitment days, the study coordinator ascertained from the ward register all medical admissions in a 24-h period and recorded these in the study register. All patients with previously negative or undocumented HIV status were offered testing using two rapid tests. All patients with a positive test (either a new or an existing test result) were eligible and invited to participate in the study. Patients receiving TB treatment at the time of hospital admission, however, were excluded.
Procedures and samples
Demographic and clinical details (including the WHO symptom screen for HIV-associated TB [17]) were recorded as were medical history, use of antiretroviral therapy (ART), TB treatment and isoniazid preventive therapy (IPT). Patients were systematically investigated by the research team by obtaining sputum, urine and blood specimens for mycobacteriology between 9.00 am on the day of enrolment and 9.00 am the following day. Numerous additional samples for mycobacteriology were requested by the routine medical team as clinically indicated during the patient’s admission. These included sputum and a wide range of non-respiratory samples (Table 1).
Table 1.
Clinical samples sent for mycobacteriology
| Sample | Urine and sputum samples obtained in first 24 h | Total samples obtained during admission | |||||
|---|---|---|---|---|---|---|---|
| Number of patients producing ≥1 sample (%) | Total number of samples | Number of patients producing ≥1 sample (%) | Total number of samples | Total number of culture and Xpert tests done | Number of positive culture and Xpert tests (%) | Number of TB patients with ≥1 positive culture or Xpert test (%) | |
| Sputum | 158 (37.0) | 279 | 245 (57.4) | 615 | 871 | 210 (24.1) | 75 (54.0)a |
| Urine | 418 (97.9) | 418 | 418 (97.9) | 418 | 833 | 141 (16.9) | 89 (64.0) |
| Other non-respiratory samples | - | - | 418 (97.9) | 712 | 687 | 91 (13.2) | 69 (49.6) |
| Ascitic fluid | - | - | 5 (1.2) | 5 | 5 | 1 (20.0) | 1 (0.7) |
| Blood | - | - | 410 (96.0) | 469 | 469 | 41 (8.7) | 41 (29.5) |
| Bone marrow | - | - | 2 (0.5) | 2 | 2 | 0 | 0 |
| Cerebrospinal fluid (CSF) | - | - | 76 (17.8) | 94 | 94 | 8 (8.5) | 8 (5.8) |
| Fine needle aspirate (FNA) | - | - | 19 (4.4) | 23 | 10 | 6 (60.0) | 6 (4.3) |
| Gastric lavage | - | - | 5 (1.2) | 7 | 7 | 2 (28.6) | 1 (0.7) |
| Pus | - | - | 5 (1.2) | 6 | 6 | 4 (66.7) | 3 (2.2) |
| Pleural fluid | - | - | 21 (4.9) | 29 | 29 | 17 (58.6) | 13 (9.4) |
| Stoolb | - | - | 9 (2.1) | 10 | 0 | 0 | 0 |
| Urinec | - | - | 60 (14.1) | 63 | 61 | 11 (18.0) | 11 (7.9) |
| Other | - | - | 4 (0.9) | 4 | 4 | 1 (25.0) | 1 (0.7) |
| Total | 420 (98.4) | 697 | 427 (100) | 1,745 | 2,391 | 442 (18.5) | 139 (100) |
aOnly 39 (28.1 %) of total diagnoses could be made from sputum samples obtained in the first 24 h; btested by Ziehl–Neelsen staining only; curine samples requested later than the first 24-h period for culture (not part of Xpert screening strategy)
In the first 24 h of admission, two sputum samples were requested from each patient with careful instruction and supervision by the study coordinator who was a trained respiratory nurse. A spot specimen was obtained first followed by a second sample that was induced using nebulized 3 % hypertonic saline. If necessary, both specimens were induced. Alternatively, for patients too unwell for sputum induction (for example, those with respiratory failure, bronchospasm or other danger signs), two spot specimens were requested instead. Urine samples were systematically collected using single-use disposable bed pans (Litha Healthcare Group, Johannesburg, South Africa) and a sterile syringe was used to transfer 50 ml to a polypropylene tube (Becton Dickinson, Sparks, MD, USA). Fresh aliquots (2.0 ml) were sent for immediate Xpert testing and the remaining urine was stored at −20°C for repeat Xpert testing after defrosting and concentration by centrifugation. Venous blood (5.0 ml) was inoculated into BACTEC™ Myco/F Lytic culture vials (Becton Dickinson, Franklin Lakes, NJ, USA).
Laboratory procedures
Specimens were processed using standardized protocols and quality assurance procedures in centralized accredited laboratories of the South African National Health Laboratory Service (NHLS) as described elsewhere [18, 19]. Decontaminated, centrifuged deposits of sputum samples obtained in the first 24 h were resuspended in phosphate buffer and equal volumes were tested using culture and Xpert MTB/RIF. Mycobacterial growth indicator tubes (MGIT; Becton Dickinson) were inoculated and incubated for up to 6 weeks. Culture isolates were identified as Mycobacterium tuberculosis complex with the MTBDRplus line probe assay (Hain Lifescience, Nehren, Germany).
Additional sputum samples requested by the medical team were tested by MGIT culture and/or Xpert according to prevailing policy. Blood cultures from all patients were done in BACTEC™ Myco/F Lytic culture vials and other non-respiratory samples, such as pleural fluid, cerebrospinal fluid and tissue fine needle aspirates, were tested using MGIT culture.
Urine was tested using Xpert in two ways. Fresh urine samples (2.0 ml) were centrifuged and resuspended in 0.75 ml of phosphate buffer and then tested using the Xpert MTB/RIF assay as previously described [15]. In light of study-related logistical considerations and laboratory workflow, batches of frozen urine samples were defrosted and tested on a weekly basis. Each urine sample of between 30 ml and 40 ml was defrosted and centrifuged at 3,000 g for 15 min. Following removal of the supernatant, the pellet was resuspended in the residual urine volume and 0.75 ml was tested using Xpert.
Data analysis
The proportions of patients able to produce urine and/or sputum samples during the first 24 h of admission were calculated and compared. New TB diagnoses were defined by detection of M. tuberculosis from any clinical sample obtained at any time during the admission period using MGIT culture or Xpert. The total yield of microbiologically confirmed TB diagnoses was used to calculate TB prevalence with 95 % exact confidence intervals (95 % CI). Then, using the total number of microbiological diagnoses as the denominator, we calculated the comparative yield of TB diagnoses from Xpert testing samples of urine and sputum obtained during the initial 24 h of admission. In addition, the proportions of patients whose TB diagnoses were derived from testing sputum samples (pulmonary TB (PTB)) and/or non-respiratory samples (extrapulmonary TB (EPTB)) were compared and these data were displayed using Venn diagrams.
Patients were characterized using simple descriptive statistics. Moderate and severe anaemia was defined using WHO criteria (haemoglobin ≤10.9 g/dL for both males and females) [20]. Medians were compared using either Wilcoxon rank-sum tests or Kruskal–Wallis tests as appropriate and means were compared using unpaired t-tests. Chi-squared, Fisher’s exact and McNemar’s tests were used as appropriate to compare proportions. Logistic regression analyses were used to identify patient factors associated with TB diagnosis. All variables in the univariable model meeting a cut-off of P ≤0.1 were included in the multivariable model. Statistical tests were two-sided at α = 0.05.
Results
Patients
Between 6th June 2012 and 4th October 2013, the HIV status of 1,013 of 1,018 (99.5 %) unselected new admissions to the adult medical wards was ascertained (Fig. 1). Of the 609 patients who were HIV-positive, 585 (96.1 %) were enrolled in the study and investigated for TB. Those already receiving treatment for an existing diagnosis of TB at the time of admission (n = 158) were excluded, leaving 427 patients eligible for inclusion. These were typically young adults of whom a majority knew their positive HIV status before admission and more than one half had previously started ART (Table 2). Immunodeficiency was typically advanced and CD4 cell counts (median, 149 cells/μL) were lower among those who were ART-naive compared to those currently receiving ART (115 cells/μL versus 212 cells/μL; P <0.001). Two-thirds of all patients had moderate or severe anaemia. A history of previous TB was very common. No patients had received IPT. The vast majority of all patients had a positive WHO TB symptom screen regardless of TB status.
Fig. 1.
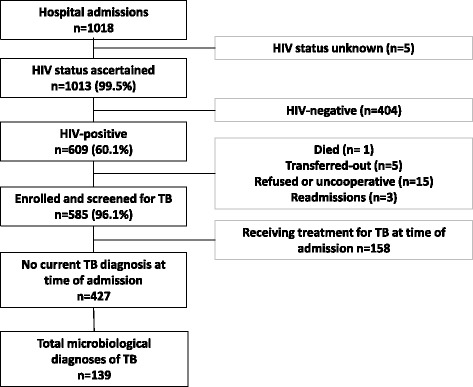
Flow diagram showing the study population
Table 2.
Patient characteristics
| Characteristic | All patients | Patients with a TB diagnosis | Patients without a TB diagnosis | P value |
|---|---|---|---|---|
| (n = 427) | (n = 139) | (n = 288) | ||
| Age (years), median (IQR) | 36.1 (28.9–42.4) | 33.8 (27.2–39.7) | 37.1 (30.0–44.0) | 0.008 |
| Female | 259 (60.7) | 90 (64.8) | 169 (58.7) | 0.229 |
| New HIV diagnosis on admission | 82 (19.2) | 34 (24.5) | 48 (16.7) | 0.055 |
| History of previous TBa | 196 (46.1) | 50 (36.2) | 146 (50.9) | 0.005 |
| ART status | ||||
| ART-naive | 177 (41.5) | 71 (51.1) | 106 (36.8) | 0.019 |
| ART interrupted | 71 (16.6) | 19 (13.7) | 52 (18.1) | |
| Current ART use | 179 (41.9) | 49 (35.3) | 130 (45.1) | |
| If currently on ART, treatment duration (years), median (IQR) | 1.6 (0.6–3.6) | 1.3 (0.2–2.9) | 1.7 (0.6–3.7) | 0.157 |
| CD4 cell count (cells/uL) (n = 424) | ||||
| Median (IQR) cells/μL | 149 (55–312) | 80 (33–182) | 191 (73–392) | <0.001 |
| <50 | 94 (22.2) | 53 (38.4) | 41 (14.3) | |
| 50–99 | 66 (15.6) | 21 (15.2) | 45 (15.7) | |
| 100–149 | 53 (12.5) | 19 (13.8) | 34 (11.9) | |
| 150–199 | 42 (9.9) | 16 (11.6) | 26 (9.1) | |
| ≥200 | 169 (39.9) | 29 (21.0) | 140 (49.0) | |
| Haemoglobin levels (n = 421) | ||||
| Median (IQR) | 9.6 (7.7–11.6) | 8.4 (6.8–10.2) | 10.2 (8.2–12.2) | <0.001 |
| No/mild anaemia | 144 (34.2) | 28 (20.1) | 116 (41.1) | |
| Moderate/severe anaemia | 277 (65.8) | 111 (79.9) | 166 (58.9) | |
| Symptoms | ||||
| Cough ≥2 weeksa | 34 (8.0) | 18 (13.0) | 16 (5.6) | 0.008 |
| Sputum productiona | 161 (38.3) | 51 (37.5) | 110 (38.7) | 0.808 |
| Current cougha | 201 (47.4) | 84 (60.9) | 117 (40.9) | <0.001 |
| Current fevera | 63 (14.9) | 24 (17.5) | 39 (13.6) | 0.294 |
| Current night sweatsa | 174 (41.0) | 73 (52.9) | 101 (35.3) | 0.001 |
| Current reported weight lossa | 189 (44.5) | 76 (55.1) | 113 (39.4) | 0.002 |
| Positive WHO symptom screena | 389 (91.5) | 134 (97.1) | 255 (88.9) | 0.005 |
Data presented are numbers (%) unless otherwise stated. aBetween two and seven values missing. IQR, interquartile range
Clinical samples obtained
During hospital admission, clinical samples for mycobacteriology were obtained from all study participants (n = 427) with a total of 1,745 samples (average, 4.1 samples per patient). At least two samples were obtained from all patients except one and these samples were from a median of three anatomic locations per patient (Table 1).
In the first 24 h of admission, urine samples were produced by 425 of 427 (99.5 %) patients, although seven samples were misplaced in transit to the laboratory, leaving 418 urine samples available for testing. In contrast, only 158 (37.0 %) patients were able to produce sputum in the same 24-h period (P <0.001) despite assistance from a respiratory nurse. Of these sputum samples, 37 (23.4 %) were obtained following sputum induction. The remaining patients who did not produce sputum were typically too sick or uncooperative to tolerate sputum induction, or it was unsuccessful.
Sputum was eventually produced by a total of 245 (57.4 %) patients at some point during their admission. The ability of patients to produce sputum samples was strongly related to the presence or absence of respiratory symptoms prior to admission. Of 161 patients who self-reported sputum production prior to admission, 143 (88.8 %) were able to produce a sputum sample for testing. Of 201 patients reporting current cough at admission, 159 (79.1 %) produced a sputum sample. Of 34 patients with chronic cough ≥2 weeks, 27 (79.4 %) produced a sputum sample.
A large number (n = 712) of various other non-respiratory samples were obtained (Table 1). A total of 2,391 Xpert and mycobacterial cultures were done on all the accumulated samples collected (mean, 5.6 tests per patient). The mean number of tests was similar for patients in whom TB was or was not diagnosed (5.8 tests versus 5.5 tests, respectively; P = 0.154). Results were missing for a small proportion of samples: 4.3 % (n = 12) of sputum cultures were contaminated; and 4.3 % (n = 12) of sputum Xpert tests and 3.1 % (n = 26) of urine Xpert tests gave indeterminate results.
TB prevalence and risk factors
A microbiological diagnosis of TB was made in 139 patients (mean, 3.2 positive samples per case diagnosed) and the characteristics of those with and without TB are summarized in Table 2. The overall prevalence of TB was 32.6 % (95 % CI, 28.1–37.2; 139/427). Thus, the number of patients that had to be screened (number needed to screen (NNS)) to diagnose one additional case was just 3.1 (95 % CI, 2.7–3.6). Overall, ≥1 non-respiratory sample(s) tested positive (indicating extrapulmonary involvement) in 115/139 (83 %) of all TB cases, including positive blood cultures in 41/139 (29.5 %). When patients were stratified by various demographic or clinical characteristics or by presenting symptoms, TB prevalence ranged from 11.1 % to 52.9 %, and in univariable analyses was associated with younger adults, those with a new HIV diagnosis, those who were ART-naive, those with lower CD4 cell counts and those with moderate or severe anaemia (Table 3). The corresponding NNS in these groups ranged from 1.9 to 9.0.
Table 3.
Tuberculosis (TB) prevalence stratified by patient characteristics and the number needed to screen (NNS) to identify one TB case in different risk groups
| Characteristic | Number of TB cases | TB prevalence, % (95 % CI) | P value | NNS (95 % CI) |
|---|---|---|---|---|
| All patients | 139 | 32.6 (28.1–37.2) | - | 3.1 (2.7–3.6) |
| Age (years) | ||||
| <35 (n = 199) | 75 | 37.7 (30.8–44.6) | 0.034 | 2.7 (2.2–3.2) |
| ≥35 (n = 228) | 64 | 28.1 (22.3–34.4) | 3.6 (2.9–4.5) | |
| Gender | ||||
| Male (n = 168) | 49 | 29.2 (22.4–36.6) | 0.260 | 3.4 (2.7–4.5) |
| Female (n = 259) | 90 | 34.8 (29.0–40.9) | 2.9 (2.4–3.4) | |
| HIV diagnosis | ||||
| New (n = 82) | 34 | 41.5 (32.1–53.1) | 0.055 | 2.4 (1.9–3.1) |
| Existing (n = 345) | 105 | 30.4 (25.0–35.1) | 3.3 (2.8–4.0) | |
| Previous history of TB | ||||
| No (n = 229) | 88 | 38.4 (32.1–45.1) | 0.005 | 2.6 (2.2–3.1) |
| Yes (n = 196) | 50 | 25.5 (19.6–32.2) | 3.9 (3.1–5.1) | |
| ART status | ||||
| Naive (n = 177) | 71 | 40.1 (32.8–47.7) | 0.007 | 2.5 (2.1–3.0) |
| Any ART exposure (n = 250) | 68 | 27.2 (21.8–33.2) | 3.7 (3.0–4.6) | |
| CD4 cell count (cells/μL) | ||||
| <100 (n = 160) | 74 | 46.3 (38.3–54.3) | <0.001 | 2.2 (1.8–2.6) |
| 100–199 (n = 95) | 35 | 36.8 (27.2–47.4) | 2.7 (2.1–3.7) | |
| ≥200 (n = 169) | 29 | 17.2 (11.8–23.7) | 5.8 (4.2–8.5) | |
| WHO anaemia grade | ||||
| No/mild anaemia (n = 144) | 28 | 19.4 (13.3–26.9) | <0.001 | 5.2 (3.7–7.5) |
| Moderate/severe anaemia (n = 277) | 111 | 40.0 (34.3–46.1) | 2.5 (2.2–2.9) | |
| Sputum production | ||||
| No (n = 259) | 85 | 32.8 (27.1–38.9) | 0.814 | 3.0 (2.6–3.7) |
| Yes (n = 161) | 51 | 31.7 (24.6–39.5) | 3.2 (2.5–4.1) | |
| Current cough | ||||
| No (n = 223) | 54 | 24.2 (18.7–30.4) | <0.001 | 4.1 (3.3–5.3) |
| Yes (n = 201) | 84 | 41.8 (34.9–48.9) | 2.4 (2.0–2.9) | |
| Cough duration | ||||
| <2 weeks (n = 389) | 120 | 30.8 (26.3–35.7) | 0.008 | 3.2 (2.8–3.8) |
| ≥2 weeks (n = 34) | 18 | 52.9 (35.1–70.2) | 1.9 (1.4–2.8) | |
| Current fever | ||||
| No (n = 360) | 113 | 31.4 (26.6–36.5) | 0.294 | 3.2 (2.7–3.8) |
| Yes (n = 63) | 24 | 38.1 (26.1–51.2) | 2.6 (2.0–3.8) | |
| Current night sweats | ||||
| No (n = 250) | 65 | 26.0 (20.7–31.9) | 0.001 | 3.8 (3.1–4.8) |
| Yes (n = 174) | 73 | 42.0 (34.5–49.7) | 2.4 (2.0–2.9) | |
| Recent weight loss | ||||
| No (n = 236) | 62 | 26.3 (20.8–32.4) | 0.002 | 3.8 (3.1–4.8) |
| Yes (n = 189) | 76 | 40.2 (33.2–47.6) | 2.5 (2.1–3.0) | |
| WHO symptom screen | ||||
| Negative (n = 36) | 4 | 11.1 (3.1–26.1) | 0.005 | 9.0 (3.8–32.3) |
| Positive (n = 389) | 134 | 34.5 (29.7–39.4) | 2.9 (2.5–3.4) | |
We next examined the predictive value of symptoms for identifying those with TB. Although the sensitivity of the WHO symptom screen [17] for HIV-associated TB was 97.1 % (92.7–99.2 %), the specificity was only 11.1 % (7.8–15.4 %) and the positive predictive value was just 34.5 % (29.7–39.4 %). In multivariable analyses, neither a positive WHO symptom screen nor a patient report of pre-admission sputum production was a significant independent predictor of TB diagnosis (Table 4). In contrast, lower CD4 cell counts and moderate and severe anaemia were independently associated with a higher risk of TB, while a history of previous treatment for TB was protective (Table 4).
Table 4.
Multivariable logistic regression of patient characteristics associated with tuberculosis (TB) diagnosis
| Characteristic | Unadjusted odds ratio | P value | Adjusted odds ratio | P value |
|---|---|---|---|---|
| Age (years) | ||||
| ≥35 | 1 | 0.034 | 1 | 0.313 |
| <35 | 1.55 (1.03–2.33) | 1.26 (0.81–1.96) | ||
| Gender | ||||
| Male | 1 | 0.227 | 1 | 0.170 |
| Female | 1.29 (0.85–1.97) | 1.40 (0.87–2.25) | ||
| Previous history of TB | ||||
| Yes | 1 | 0.004 | 1 | 0.038 |
| No | 1.82 (1.20–2.77) | 1.66 (1.03–2.69) | ||
| HIV diagnosis | ||||
| Existing | 1 | 0.059 | 1 | 0.744 |
| New | 1.62 (0.99–2.66) | 0.89 (0.46–1.75) | ||
| ART status | ||||
| Ever received ART | 1 | 0.005 | 1 | 0.206 |
| Never received ART | 1.79 (1.19–2.70) | 1.44 (0.82–2.51) | ||
| Sputum production | ||||
| Yes | 1 | 0.808 | ||
| No | 1.05 (0.69–1.61) | |||
| WHO symptom screen | ||||
| Negative | 1 | 0.002 | 1 | 0.068 |
| Positive | 4.20 (1.46–12.14) | 2.59 (0.85–7.92) | ||
| CD4 cell count (cells/μL) | ||||
| ≥200 | 1 | <0.001 | 1 | <0.001 |
| 100–199 | 2.77 (1.56–4.93) | 2.32 (1.26–4.26) | ||
| <100 | 4.15 (2.50–6.89) | 3.17 (1.81–5.56) | ||
| Anaemia severity | ||||
| No/mild anaemia | 1 | <0.001 | 1 | 0.011 |
| Moderate/severe anaemia | 2.77 (1.72–4.47) | 1.96 (1.16–3.36) | ||
Diagnostic yield from urine and sputum samples obtained in first 24 h
With the aim of defining a day 1 rapid microbiological screening strategy for new admissions, we next compared the diagnostic yields of Xpert when testing whatever sputum and urine samples could be obtained during the first 24 h of admission (Table 5). The number (%) of cases diagnosed from urine was substantially increased by prior concentration of urine by centrifugation (unconcentrated urine yielded 59 of 139 (42.4 %) diagnoses, whereas concentrated urine yielded 82 of 139 (59.0 %) diagnoses; P = 0.006). Overall, 64.0 % (89 of 139) of all cases could be diagnosed from urine. In contrast, only 39 (28.1 %) cases could be diagnosed by Xpert testing sputum (Fig. 2a) (P <0.001), reflecting in large part the small proportion of patients able to produce sputum in the first 24 h of admission. Combined urine and sputum Xpert results gave the greatest diagnostic yield, detecting 108 of 139 (77.7 %) cases (Table 5).
Table 5.
Diagnostic yield of tuberculosis (TB) cases from different sample types and the proportion of diagnoses that could be made using Xpert testing of urine samples
| Sample | Number of TB diagnoses | Diagnostic yield, % (95 % CI) | Number diagnosed by urine Xpert | Proportion diagnosed by urine Xperta, % (95 % CI) |
|---|---|---|---|---|
| All clinical samples | 139 | 100 (97.4–100) | 89 | 64.0 (55.5–72.0) |
| Samples collected during the first 24 h of admission | ||||
| Urine | ||||
| Urine Xpert (unconcentrated) | 59 | 42.4 (34.1–51.1) | 59 | - |
| Urine Xpert (concentrated) | 82 | 59.0 (50.3–67.3) | 82 | - |
| Urine Xpert (either sample) | 89 | 64.0 (55.5–72.0) | 89 | - |
| Sputum | ||||
| Xpert (first sample only) | 37 | 26.6 (19.5–34.8) | 20 | 54.1 (36.9–70.5) |
| Xpert (either sample) | 39 | 28.1 (20.8–36.3) | 20 | 51.3 (34.8–67.6) |
| Sputum and urine | ||||
| Xpert (all samples) | 108 | 77.7 (69.8–84.3) | 89 | 82.4 (73.9–89.1) |
| All other samples collected during admission | ||||
| Sputum | ||||
| Xpert | 57 | 41.0 (32.7–49.7) | 30 | 52.6 (39.0–66.0) |
| Culture | 58 | 41.7 (33.4–50.4) | 33 | 56.9 (43.2–69.8) |
| Either culture or Xpert | 75 | 54.0 (453–62.4) | 42 | 56.0 (44.1–67.5) |
| Cultures of non-respiratory samples | ||||
| All non-respiratory samples | 70 | 50.3 (41.8–58.9) | 46 | 65.7 (53.4–76.7) |
| Blood | 41 | 29.5 (22.1–37.8) | 32 | 78.0 (62.4–89.4) |
| Pleural fluid | 13 | 9.4 (5.1–15.5) | 6 | 46.2 (19.2–74.9) |
| Urine | 11 | 7.9 (4.0–13.7) | 8 | 72.7 (39.0–94.0) |
| Cerebrospinal fluid (CSF) | 8 | 5.8 (2.5–11.0) | 3 | 37.5 (8.5–75.5) |
| Lymph node fine needle aspirate (FNA) | 6 | 4.3 (1.6–9.2) | 4 | 66.7 (22.2–95.7) |
| Other | 5 | 3.6 (1.2–8.2) | 4 | 80.0 (28.4–99.5) |
aAny positive result from testing unconcentrated and concentrated samples
Fig. 2.
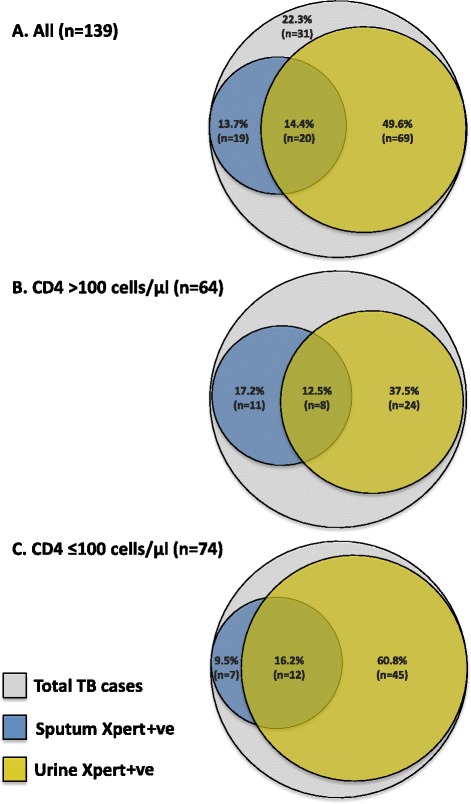
Tuberculosis (TB) diagnoses made by Xpert from urine and sputum samples collected in the first 24 h of hospital admission. Venn diagrams show diagnostic yields as proportions of (a) total TB diagnoses (n = 139), (b) TB diagnoses in patients with CD4 cell counts >100 cells/μL (n = 64) and (c) TB diagnoses in patients with CD4 cell counts ≤100 cells/μL (n = 74). Note: the CD4 cell count result was missing for one patient with TB
The diagnostic yield obtained from urine but not sputum was associated with the CD4 cell count. In those with CD4 cell counts >100 and ≤100 cells/μL, the proportions diagnosed from sputum were similar (29.7 % versus 25.7 %, respectively; P = 0.70) whereas the yield from Xpert testing urine was substantially greater among those with lower CD4 cell counts (50.0 % versus 77.0 %, respectively; P = 0.001) (Fig. 2b,c).
Diagnostic yield from total clinical samples collected during admission
We next compared the diagnostic yield from Xpert tests done on admission urine samples (n = 418) with the yield from all other samples (615 sputum samples and 712 non-respiratory samples) collected during the entire period of hospital admission (Table 5 and Fig. 3). The yield from Xpert testing urine was slightly greater (but this did not reach statistical significance) than that obtained from the combined yield from Xpert and culture tests done on sputum samples (64.0 % versus 54.0 %, respectively; P = 0.146), but did exceed that from cultures of other non-respiratory samples (64.0 % vs 50.4 %, respectively; P = 0.028) (Fig. 3a).
Fig. 3.
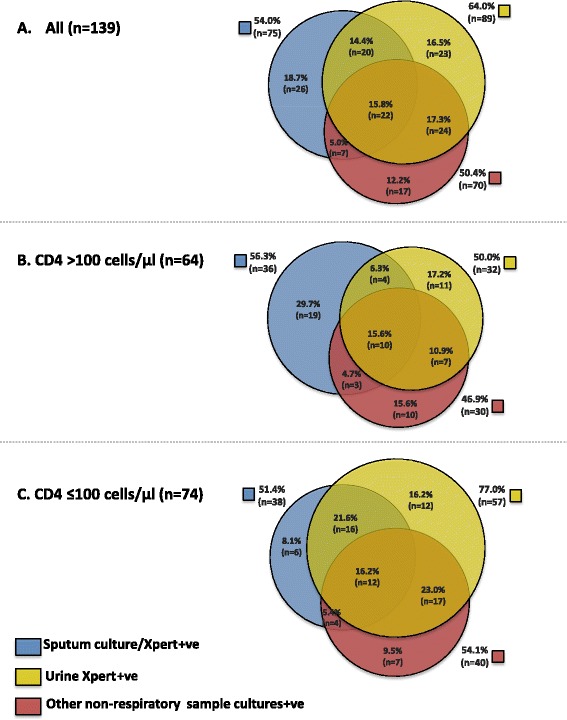
Yields of total tuberculosis (TB) diagnoses from all clinical samples collected at any time during hospital admission. Yields of TB diagnoses made by testing urine samples (using Xpert) collected on admission compared with the yield from all sputum samples (using either Xpert and/or culture) and all other non-respiratory samples (using culture). Venn diagrams show yields as proportions of (a) all TB diagnoses (n = 139), (b) TB diagnoses in patients with CD4 cell counts >100 cells/μL (n = 64) and (c) TB diagnoses in patients with CD4 cell counts ≤100 cells/μL (n = 74). Note: the CD4 cell count result was missing for one patient with TB
Of 75 total microbiologically confirmed pulmonary TB (PTB) diagnoses, more than one half (n = 42; 56.0 %) could alternatively be diagnosed by testing urine with Xpert. Similarly, of the 70 microbiologically confirmed extrapulmonary TB (EPTB) diagnoses made using culture of non-respiratory samples, two-thirds (n = 46; 65.7 %) could be made by testing urine with Xpert. This proportion varied by sample type (Table 5). For example, whereas 78.0 % (32 of 41) of those with positive blood cultures tested urine Xpert positive, only 37.5 % (3 of 8) of those with culture-confirmed TB meningitis tested urine Xpert positive.
Specificity of Xpert testing
We finally examined the possibility of false-positive sputum Xpert results in patients previously treated for TB disease who might potentially have had persistent shedding of non-viable organisms in sputum [21]. A positive Xpert test from one or more sputum samples was recorded in 57 patients with a TB diagnosis. Of these, 50 (88 %) had positive cultures from either sputum or a non-respiratory sample, thereby confirming a current diagnosis of active TB. Of the remaining seven patients, four had a history of previous TB treatment but only one of these had received treatment for TB within the preceding 3-year period.
Discussion
Using comprehensive clinical sampling, a microbiological diagnosis of TB was made in one in three unselected HIV-positive new medical admissions to this South African district hospital. Since TB prevalence was so high and since neither clinical symptoms nor patient risk factors could be used to reliably predict who did and who did not have TB, we suggest that a policy of routine microbiological investigation of all HIV-positive medical admissions may be justified in this and other high-burden settings. Urine samples were readily obtained from patients in the first 24 h of admission and testing these with Xpert was the single investigation that yielded the greatest number of TB diagnoses, representing nearly two-thirds of total TB diagnoses. Use of Xpert to screen sputum samples collected in the first 24 h provided a substantially lower yield, reflecting the well-recognized difficulty of obtaining sputum from sick in-patients, especially when they have not been pre-selected based on respiratory symptoms. Routine testing of urine samples with Xpert provides an effective means of rapid TB diagnosis in this patient population and one that could readily be implemented wherever the GeneXpert test platform is already being used. Consideration should be given to routine testing of urine as the initial diagnostic screen in such patients, and especially in those for whom sputum production is difficult.
Patients were investigated very thoroughly for TB with an average of 5.6 tests done on samples obtained from a median of three anatomic compartments in each patient. Thus, this is likely to have provided a very reliable estimate of TB prevalence in these unselected patients. Positive non-respiratory samples indicated extrapulmonary involvement in a large majority (83 %) of TB cases. Indeed, disease was frequently disseminated as shown by positive blood cultures in 30 % of TB patients and the observation that samples from more than one anatomic site tested positive for TB in approximately half of all TB cases (Fig. 3).
The prevalence of TB varied by risk categories but in none of the stratified groups was the prevalence less than 10 % (Table 3). Admission symptoms were very poorly predictive of undiagnosed TB and were not significantly associated with TB in multivariable analysis. Thus, we propose that in such clinical populations, patients should be investigated for TB regardless of their symptoms. While multiple studies of unselected out-patients screened prior to starting ART in South Africa have reported TB prevalence rates of approximately 20–25 % [18, 22–24], comparable studies of unselected hospital in-patients are lacking. In Lusaka, Zambia, the prevalence of sputum culture-positive TB was 27 % among HIV-positive medical in-patients, but these patients were selected on the basis of ability to produce sputum [25]. In the absence of a microbiological diagnosis, some patients might have received empirical TB treatment. However, since presentation was so very non-specific, such a strategy would inevitably miss many cases and TB treatment would be unlikely to be started within the first 24 h of admission.
Only approximately one third of all patients could produce a sputum sample within 24 h of admission despite assistance from a dedicated study respiratory nurse and availability of sputum induction [26]. Just over one half could produce sputum at any time during admission and this was strongly related to the presence or absence of respiratory symptoms at the time of admission. Thus, the low yield from sputum was directly related to the fact that patients were investigated for TB without pre-selection according to respiratory symptomatology. However, in a previous study of unselected HIV-positive ambulatory out-patients in this setting, the same research nurse using the same protocol obtained sputum from 90 % of patients at a single clinic visit [18, 26]. This also illustrates the well-recognized difficulties in obtaining sputum from hospital in-patients who are often too sick, weak or unable to cooperate. Thus, the very high comparative yield of urine-based TB diagnostics in this study was in large part a direct result of the ease with which urine could readily be obtained.
Prior centrifugation of between 30 ml and 40 ml of urine substantially increased the yield of cases and this observation is explained by the fact that Xpert detects the DNA associated with whole M. tuberculosis bacilli, which sediment with centrifugation, rather than detecting free DNA [27, 28]. The detection of M. tuberculosis bacilli in urine is strongly suggestive of renal involvement with TB, most likely arising as a result of haematogenous disease dissemination. The yield from urine was substantially greater among those with lower CD4 cell counts (Fig. 2b,c), likely reflecting higher mycobacterial load and greater risk of disease dissemination and renal involvement. Our findings are entirely consistent with a study from the USA early in the HIV epidemic, which reported a very high yield (77 %) of diagnoses from culture of urine samples from HIV-infected patients with advanced immunodeficiency and extrapulmonary TB [29]. However, compared to culture, which may take several weeks, Xpert testing takes just 2 h. The Determine TB-LAM urine lateral-flow assay for lipoarabinomannan is an alternative urine-based rapid TB diagnostic that has shown promise [30]. Although the diagnostic yield is lower than that of urine Xpert [16], its potential use at the point-of-care and the lack of need for instrumentation or electricity supply and its low cost are all very considerable advantages [30].
Xpert testing of urine could be used as a rapid screening investigation for TB among HIV-infected adults admitted to medical wards in high-burden settings. The optimum diagnostic algorithm for a given setting will depend on the disease burden and the financial resources and infrastructure available. In South Africa, a single Xpert cartridge is allocated per patient under national implementation. The greatest overall diagnostic yield in this clinical population would be obtained from testing concentrated urine samples and, if used to routinely screen all HIV-infected patients, approximately one in five tests would be positive. To gain the increased yield derived from sample centrifugation, testing would have to be laboratory-based and with appropriate biosafety facilities. Use of urine as the initial diagnostic sample might reduce the need to obtain respiratory and other non-respiratory samples. The advantages of this approach would include reducing the generation of infectious bio-aerosols in the ward environment, decreasing the need for biohazardous sputum induction or the need for invasive procedures to sample extra-pulmonary disease sites and reducing requirements for culture. Importantly, urine-based TB diagnosis identifies patients with the highest mortality risk [15, 16, 31, 32]; expediting TB diagnosis and treatment in this group may potentially improve survival. The impact of this screening strategy on survival and clinical outcomes is being evaluated in a large randomized controlled trial in South Africa and Malawi (Rapid urine-based Screening for Tuberculosis to reduce AIDS-related Mortality in hospitalized Patients in Africa (STAMP) trial; ISRCTN71603869).
Strengths of the present study include the investigation of an unselected sample of HIV-infected patients regardless of respiratory symptoms or clinical suspicion of TB or ability to produce a sputum sample. Microbiological investigation for TB was extremely thorough, testing a very large number of samples using quality-assured laboratories. Xpert has been demonstrated to have very high specificity when testing both respiratory and non-respiratory samples [12–14]. However, we carefully assessed the possibility of false-positive Xpert tests occurring among patients previously treated for TB and shedding non-viable organisms in sputum as being very low in this patient population. We also used single-use sterile receptacles for urine collection to reduce any risk of cross-contamination of urine samples with either live or dead M. tuberculosis bacilli.
Weaknesses include the fact that the study was conducted at a single site and the extent to which these findings can be generalized to other settings remains to be assessed. However, the remarkable uniformity in the findings of autopsy studies of HIV-infected in-patients conducted in West, East and southern Africa [2–7] and in India [33] suggest that these findings are likely to be broadly relevant across high-burden settings. The results should not be generalized to HIV-infected medical out-patients in whom the diagnostic yield is known to be lower [15].
Conclusion
In conclusion, this study has defined a means of rapid microbiological diagnosis of HIV-associated TB through systematic screening in newly admitted HIV-positive medical in-patients in high TB burden settings. This urine-based approach overcomes the frequent difficulties in obtaining sputum samples from such patients. In addition to sputum testing, routine testing of urine samples with Xpert should be considered and further evaluated either as a first-line screening investigation to enhance the yield and speed of TB diagnosis in this clinical population or as an adjunctive investigation in patients who are sputum-scarce.
Acknowledgements
The investigators are grateful to staff of the GF Jooste Hospital and also to the Provincial Government of the Western Cape for granting permission for this study. The study was funded by the Wellcome Trust, London, UK (grant number 088590). SDL and GM were funded by the Wellcome Trust, London, UK (grant numbers 088590 (SDL), 098316 and 085251 (GM)). SDL is also supported by a Global Clinical Trials Grant from the Medical Research Council (MRC), Department for International Development (DFID) and Wellcome Trust (STAMP trial; grant number MR/M007375/1). GM was also supported in part by the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation (NRF) of South Africa (grant number 64787). Any opinion, finding and conclusion or recommendation expressed in this material is that of the authors and the NRF does not accept any liability in this regard.
Role of the funding source
The study was funded by the Wellcome Trust. The funders had no role in the study design, data collection, data analysis, data interpretation, or writing of this report. The opinions, findings and conclusions expressed in this manuscript reflect those of the authors alone. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Abbreviations
- ART
Antiretroviral therapy
- CI
Confidence interval
- EPTB
Extrapulmonary tuberculosis
- IPT
Isoniazid preventive therapy
- MGIT
Mycobacterial growth indicator tube
- NHLS
National Health Laboratory Service
- NNS
Number needed to screen
- PTB
Pulmonary tuberculosis
- TB
Tuberculosis
- WHO
World Health Organization
- Xpert
Xpert MTB/RIF
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SDL designed the study with input from RB, GM and MN. PP, RB, GvW, CS and GM were responsible for patient recruitment. MV and ADK were responsible for the database. SDL and ADK designed the analyses and ADK did the analyses. MN was responsible for the mycobacteriology. SDL wrote the first draft of the paper and GM, ADK and MN gave input to further drafts. All authors commented on drafts and approved the final version of the article. SDL takes responsibility for the integrity of this study and decision to publish these data.
Contributor Information
Stephen D. Lawn, Phone: +44 (0)20 7927 2546, Email: stephen.lawn@lshtm.ac.uk
Andrew D. Kerkhoff, Email: andrewkerkhoff@gmail.com
Rosie Burton, Email: rosie@polka.co.za.
Charlotte Schutz, Email: charlottelouw@discoverymail.co.za.
Gavin van Wyk, Email: gvw001@gmail.com.
Monica Vogt, Email: monica.vogt@hiv-research.org.za.
Pearl Pahlana, Email: pearlpahlana@yahoo.com.
Mark P. Nicol, Email: mark.nicol@uct.ac.za
Graeme Meintjes, Email: graemein@mweb.co.za.
References
- 1.World Health Organization (WHO). Global tuberculosis report 2014. Geneva: WHO; 2014. Available at: http://apps.who.int/iris/bitstream/10665/137094/1/9789241564809_eng.pdf?ua=1. Accessed 31 July 2015.
- 2.Gupta RK, Lucas SB, Fielding KL, Lawn SD. Prevalence of tuberculosis in post-mortem studies of HIV-infected adults and children in resource-limited settings: a systematic review and meta-analysis. AIDS 2015; in press. [DOI] [PMC free article] [PubMed]
- 3.Lucas SB, Hounnou A, Peacock C, Beaumel A, Djomand G, N'Gbichi JM, et al. The mortality and pathology of HIV infection in a west African city. AIDS. 1993;7:1569–79. doi: 10.1097/00002030-199312000-00005. [DOI] [PubMed] [Google Scholar]
- 4.Rana FS, Hawken MP, Mwachari C, Bhatt SM, Abdullah F, Ng'ang'a LW, et al. Autopsy study of HIV-1-positive and HIV-1-negative adult medical patients in Nairobi, Kenya. J Acquir Immune Defic Syndr. 2000;24:23–9. doi: 10.1097/00126334-200005010-00004. [DOI] [PubMed] [Google Scholar]
- 5.Cohen T, Murray M, Wallengren K, Alvarez GG, Samuel EY, Wilson D. The prevalence and drug sensitivity of tuberculosis among patients dying in hospital in KwaZulu-Natal, South Africa: a postmortem study. PLoS Med. 2010;7 doi: 10.1371/journal.pmed.1000296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cox JA, Lukande RL, Nelson AM, Mayanja-Kizza H, Colebunders R, Van Marck E, et al. An autopsy study describing causes of death and comparing clinico-pathological findings among hospitalized patients in Kampala, Uganda. PLoS One. 2012;7 doi: 10.1371/journal.pone.0033685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wong EB, Omar T, Setlhako GJ, Osih R, Feldman C, Murdoch DM, et al. Causes of death on antiretroviral therapy: a post-mortem study from South Africa. PLoS One. 2012;7 doi: 10.1371/journal.pone.0047542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.World Health Organization (WHO). WHO tuberculosis programme framework for effective tuberculosis control. Geneva: WHO; 1994. WHO/TB/94.179. Available at: http://whqlibdoc.who.int/hq/1994/WHO_TB_94.179.pdf. Accessed 31 July 2015.
- 9.Reid MJ, Shah NS. Approaches to tuberculosis screening and diagnosis in people with HIV in resource-limited settings. Lancet Infect Dis. 2009;9:173–84. doi: 10.1016/S1473-3099(09)70043-X. [DOI] [PubMed] [Google Scholar]
- 10.Lawn SD, Wood R. Tuberculosis in antiretroviral treatment services in resource-limited settings: addressing the challenges of screening and diagnosis. J Infect Dis. 2011;204:S1159–67. doi: 10.1093/infdis/jir411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.World Health Organization (WHO). Tuberculosis diagnostics automated DNA test. WHO endorsement and recommendations. Geneva: WHO; 2010. Available at: http://www.who.int/tb/features_archive/xpert_factsheet.pdf. Accessed 31 July 2015.
- 12.World Health Organization (WHO). Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children: policy update. WHO/HTM/TB/2013.16. Geneva: WHO; 2013. Accessible at: http://apps.who.int/iris/bitstream/10665/112472/1/9789241506335_eng.pdf?ua=1. Accessed 31 July 2015.
- 13.Denkinger CM, Schumacher SG, Boehme CC, Dendukuri N, Pai M, Steingart KR. Xpert MTB/RIF assay for the diagnosis of extrapulmonary tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2014;44:435–46. doi: 10.1183/09031936.00007814. [DOI] [PubMed] [Google Scholar]
- 14.Maynard-Smith L, Larke N, Peters JA, Lawn SD. Diagnostic accuracy of the Xpert MTB/RIF assay for extrapulmonary and pulmonary tuberculosis when testing non-respiratory samples: a systematic review. BMC Infect Dis. 2014;14:709. doi: 10.1186/s12879-014-0709-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lawn SD, Kerkhoff AD, Vogt M, Wood R. High diagnostic yield of tuberculosis from screening urine samples from HIV-infected patients with advanced immunodeficiency using the Xpert MTB/RIF assay. J Acquir Immune Defic Syndr. 2012;60:289–94. doi: 10.1097/QAI.0b013e318258c6af. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Peter JG, Theron G, Muchinga TE, Govender U, Dheda K. The diagnostic accuracy of urine-based Xpert MTB/RIF in HIV-infected hospitalized patients who are smear-negative or sputum scarce. PLoS One. 2012;7 doi: 10.1371/journal.pone.0039966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Getahun H, Kittikraisak W, Heilig CM, Corbett EL, Ayles H, Cain KP, et al. Development of a standardized screening rule for tuberculosis in people living with HIV in resource-constrained settings: individual participant data meta-analysis of observational studies. PLoS Med. 2011;8 doi: 10.1371/journal.pmed.1000391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lawn SD, Kerkhoff AD, Vogt M, Wood R. Diagnostic accuracy of a low-cost, urine antigen, point-of-care screening assay for HIV-associated pulmonary tuberculosis before antiretroviral therapy: a descriptive study. Lancet Infect Dis. 2012;12:201–9. doi: 10.1016/S1473-3099(11)70251-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lawn SD, Brooks SV, Kranzer K, Nicol MP, Whitelaw A, Vogt M, et al. Screening for HIV-associated tuberculosis and rifampicin resistance before antiretroviral therapy using the Xpert MTB/RIF assay: a prospective study. PLoS Med. 2011;8 doi: 10.1371/journal.pmed.1001067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.World Health Organization (WHO). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. WHO/NMH/NHD/MNM/11.1. Geneva: WHO; 2011. Accessible at: http://www.who.int/vmnis/indicators/haemoglobin.pdf. Accessed 31 July 2015.
- 21.Friedrich SO, Rachow A, Saathoff E, Singh K, Mangu CD, Dawson R, et al. Assessment of the sensitivity and specificity of Xpert MTB/RIF assay as an early sputum biomarker of response to tuberculosis treatment. Lancet Respir Med. 2013;1:462–70. doi: 10.1016/S2213-2600(13)70119-X. [DOI] [PubMed] [Google Scholar]
- 22.Lawn SD, Kranzer K, Edwards DJ, McNally M, Bekker LG, Wood R. Tuberculosis during the first year of antiretroviral therapy in a South African cohort using an intensive pretreatment screening strategy. AIDS. 2010;24:1323–8. doi: 10.1097/QAD.0b013e3283390dd1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bassett IV, Wang B, Chetty S, Giddy J, Losina E, Mazibuko M, et al. Intensive tuberculosis screening for HIV-infected patients starting antiretroviral therapy in Durban, South Africa. Clin Infect Dis. 2010;51:823–9. doi: 10.1086/656282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Houlihan CF, Mutevedzi PC, Lessells RJ, Cooke GS, Tanser FC, Newell ML. The tuberculosis challenge in a rural South African HIV programme. BMC Infect Dis. 2010;10:23. doi: 10.1186/1471-2334-10-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bates M, O'Grady J, Mwaba P, Chilukutu L, Mzyece J, Cheelo B, et al. Evaluation of the burden of unsuspected pulmonary tuberculosis and co-morbidity with non-communicable diseases in sputum producing adult inpatients. PLoS One. 2012;7 doi: 10.1371/journal.pone.0040774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lawn SD, Kerkhoff AD, Pahlana P, Vogt M, Wood R. Diagnostic yield of tuberculosis using sputum induction in HIV-positive patients before antiretroviral therapy. Int J Tuberc Lung Dis. 2012;16:1354–7. doi: 10.5588/ijtld.12.0174. [DOI] [PubMed] [Google Scholar]
- 27.Lawn SD, Nicol MP. Xpert(R) MTB/RIF assay: development, evaluation and implementation of a new rapid molecular diagnostic for tuberculosis and rifampicin resistance. Future Microbiol. 2011;6:1067–82. doi: 10.2217/fmb.11.84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Blakemore R, Story E, Helb D, Kop J, Banada P, Owens MR, et al. Evaluation of the analytical performance of the Xpert MTB/RIF assay. J Clin Microbiol. 2010;48:2495–501. doi: 10.1128/JCM.00128-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Shafer RW, Kim DS, Weiss JP, Quale JM. Extrapulmonary tuberculosis in patients with human immunodeficiency virus infection. Medicine (Baltimore) 1991;70:384–97. doi: 10.1097/00005792-199111000-00004. [DOI] [PubMed] [Google Scholar]
- 30.Lawn SD. Point-of-care detection of lipoarabinomannan (LAM) in urine for diagnosis of HIV-associated tuberculosis: a state of the art review. BMC Infect Dis. 2012;12:103. doi: 10.1186/1471-2334-12-103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lawn SD, Kerkhoff AD, Vogt M, Wood R. Clinical significance of lipoarabinomannan detection in urine using a low-cost point-of-care diagnostic assay for HIV-associated tuberculosis. AIDS. 2012;26:1635–43. doi: 10.1097/QAD.0b013e3283553685. [DOI] [PubMed] [Google Scholar]
- 32.Talbot E, Munseri P, Teixeira P, Matee M, Bakari M, Lahey T, et al. Test characteristics of urinary lipoarabinomannan and predictors of mortality among hospitalized HIV-infected tuberculosis suspects in Tanzania. PLoS One. 2012;7 doi: 10.1371/journal.pone.0032876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lanjewar DN. The spectrum of clinical and pathological manifestations of AIDS in a consecutive series of 236 autopsied cases in Mumbai, India. Patholog Res Int. 2011;2011:547618. doi: 10.4061/2011/547618. [DOI] [PMC free article] [PubMed] [Google Scholar]