

Abstract
Background: To explore the correlation between FTO (fat mass and obesity associated) gene, which is associated with 3 single nucleotide polymorphisms (SNP) of fat mass and obesity, type 2 diabetes and body mass index (BMI) in the Uygur population in northwest China. Methods: A total of 849 Uygur patients with type 2 diabetes mellitus were selected from the hospitalized patients in the First Affiliated Hospital of Xinjiang Medical University, the First People’s Hospital of Kashi and the hospitals in the Turpan areas. At the same time, 873 cases of healthy persons who conducted a medical checkup in the physical examination centre of the above hospitals were enrolled as controls. The present investigation used the case-control research method, and physical examination and biochemical index determination were carried out. The Sequenom MassARRAY technology was employed in the detection of 3 SNP loci of the FTO gene. The representative population of each SNP in the control group was analyzed by Hardy-Weinberg law. The differences of each clinical parameter in the two groups were analyzed by t-test analysis. The differences of genotype and allele of each SNP in the two groups were analyzed by χ2 test. Results: BMI, waistline (WL), systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting blood glucose (FBG), total cholesterol (TC), aspartate aminotransferase (AST) and alanine aminotransferase (ALT) in the type 2 diabetes group were higher than those in the control group, while the high density lipoprotein (HDL) and low density lipoprotein (LDL) were lower than those of the control group; 2. The allele frequency of A of rs8050136 and rs9939609 in the type 2 diabetes mellitus group was higher than that of the control group. The BMI of the whole population and type 2 diabetes group with genotype C/A+A/A of rs8050136 was higher than that in C/C group, and the BMI with genotype T/A+A/A of rs9939609 was higher than that in group T/T. Stratification was conducted on BMI according to the normal, overweight and obesity criteria. There were significant differences in the distribution of genotype frequency of rs9939609 in the type 2 diabetes group and the control group of the normal BMI group. Conclusion: Single nucleotide mutation of rs7195539 in FTO gene may be a protective factor against the Uygur type 2 diabetes. Single nucleotide mutations of rs8050136 and rs9939609 may be associated with the Uygur type 2 diabetes and obesity, with A as a potential risk allele. The gene polymorphism of rs8050136 may correlate with type 2 diabetes mellitus through the function of BMI, while the correlation between rs9939609 gene polymorphism and type 2 diabetes is not depending from BMI.
Keywords: FTO, gene polymorphism, type 2 diabetes, Uygur
Introduction
Type 2 diabetes is considered as a complex disease caused by a combination of genetic and environmental factors, of which the genetic factors play a vital role in the pathogenesis of type 2 diabetes. There are a total of 92.4 million adult diabetic people in China [1]. Obesity is a major risk factor for type 2 diabetes mellitus, and the genetic variation influencing obesity may also affect the onset of type 2 diabetes. In 2007, Frayling et al. discovered in the genome-wide association study (GWAS) on the susceptibility genes of type 2 diabetes mellitus, that there was a strong correlation between the sequence variation of the FTO gene located on chromosome 16 on the one hand and BMI, obesity and type 2 diabetes in European Caucasians on the other [2]. Subsequently, several research groups demonstrated that the common variation of FTO gene was correlated with type 2 diabetes independently of BMI in various populations [3-7]. Many SNPs of FTO gene were correlated with type 2 diabetes mellitus, but the results were different in different populations studied [2-4,7-13]. The daily lifestyle and food habits of the Uygur people are different from those of the Han population. Furthermore, the contents of protein and fat in the diet of Uygur people are high, and the population shows a large number of overweight and obese people. Since abdominal obesity is largely diffused in the Uygur type 2 diabetic patients, the objective of the present study was to investigate the distribution characteristics of 3 SNPs of the FTO gene in the Uygur people of Xinjiang to investigate the correlation between the FTO gene polymorphism, Uygur type 2 diabetes and obesity, providing scientific basis for a future prevention and treatment of Uygur patients with type 2 diabetes mellitus.
Materials and methods
Patients
A total number of 849 Uygur patients with type 2 diabetes mellitus, 530 male and 319 female with mean age of 51.30 ± 9.84, were selected from the First Affiliated Hospital of Xinjiang Medical University, the First People’s Hospital of Kashi and the hospitals in the Turpan areas, during the period between March 2012 and September 2013. In addition, a total number of 873 healthy Uygur people, 557 male and 316 female with mean age of 50.44 ± 9.94, without any kinship and diabetes, who conducted medical checkup in the above mentioned hospitals during the same period of time, were employed as controls. There was no significant difference of age and gender in the diabetic group and in the control group. All the recruited subjects filled informed consents before participating in this study, and the research program has been approved by the ethics committee of the First Affiliated Hospital of Xinjiang Medical University.
The diagnosis criteria of diabetes used in the present investigation were consistent with the criteria applied by the World Health Organization (WHO) in 1999 and in previous years, to diagnose type 2 diabetes [14]. The recruited subjects were divided into 3 groups according to the Guidelines for the prevention and control of the Chinese adult overweight and obesity: normal group: BMI < 24 kg/m2; overweight group: 24 kg/m2 ≤ BMI < 28 kg/m2; obesity group: BMI ≥ 28 kg/m2 [15].
Research methods
Physical examinations such as height, weight, waist circumference, systolic and diastolic blood pressure, were carried out on all the subjects. Family and current disease history were asked and reported in details. All the research subjects were fasted for 8 hours. Four mL fasting venous blood was collected for anticoagulation and non-anticoagulation analysis. Blood serum was separated in 2 hours at 3500 rpm, and biochemical indexes such as Scr, UA, FPG, TG, TC, HDL, LDL, AST and ALT were measured. The above indexes were examined and analyzed by the Hitachi 7600 automatic biochemical analyzer in the First Affiliated Hospital of Xinjiang Medical University laboratory, and quality control was qualified. Anticoagulant venous blood was divided into EP tubes and stored in the -80°C refrigerator for further DNA extraction, avoiding a frequent freeze-thaw procedure.
The DNA of the peripheral blood was extracted by the automatic extraction instrument of the Beijing hundred Taike Biotechnology Co. Ltd., and the specific operation steps were consistent with the nucleic acid automatic extraction instrument method. The extracted DNA of the whole blood genome was analyzed by 1% agarose gel electrophoresis, and the concentration and DNA degradation degree were subsequently estimated. The DNA A260/A280 ratio (OD) obtained by Quality inspection was in the range of 1.8-2.0, with a DNA concentration of more than 50 ng/uL and good quality gel electrophoresis bands. This DNA was thus perfect to be subsequently used. The samples were then transferred to 96-well plates and stored at -20°C for further analysis.
All the 3 SNPs of the FTO gene were investigated by the analysis of the hotspot in SNP, function candidate SNP and labeled SNP including rs7195539, rs7203521, rs8050136, rs9939609. The detection of SNPs was carried out by the Beijing CapitalBio Corporation by using Sequenom MassARRAY RSNP technology. The success rate and accuracy rate of genotyping in this study was more than 98%.
Statistical analyses
SPSS 21.0 statistical software was used in the current research. The Hardy-Weinberg equilibrium in the control group was used to evaluate whether statistical sampling are representative of the population. Data were expressed as mean ± standard deviation. After normalizing the values, t-test was used for two groups’ comparison and one-way ANOVA was used for multiple groups’ comparison. χ2 test was used for the comparison of the enumerated data, the genotype and allele frequency of each SNP in two groups and genotype and allele frequencies between groups. P < 0.05 was considered statistically significant.
Results
Various clinical indexes in the type 2 diabetes group and in the control group
There was no significant difference in gender and age between the type 2 diabetes group and the control group (P = 0.554, 0.072). There was no significant difference in Scr and UA between the two groups (P = 0.269, 0.093). BMI, WL, SBP, DBP, FPG, TC, AST and ALT in type 2 diabetes group were higher than those of the control group, although HDL and LDL were lower than those of the control group (P < 0.05) (Table 1).
Table 1.
Comparison of various clinical indexes in the type 2 diabetes group and in the control group
| Variable | Control | Case | P |
|---|---|---|---|
| Sex (M/F) | 557/316 | 530/319 | 0.554 |
| Age | 50.44 ± 9.94 | 51.30 ± 9.84 | 0.072 |
| BMI (kg/m2) | 27.04 ± 3.93 | 28.34 ± 4.70 | < 0.001 |
| WL (cm) | 95.70 ± 10.15 | 99.46 ± 11.11 | < 0.001 |
| SBP (mmHg) | 123.10 ± 18.31 | 126.69 ± 18.97 | 0.001 |
| DBP (mmHg) | 77.38 ± 12.58 | 78.81 ± 11.72 | 0.037 |
| Scr (umol/L) | 70.82 ± 18.55 | 68.79 ± 49.71 | 0.269 |
| UA (umol/L) | 282.12 ± 69.17 | 273.34 ± 134.87 | 0.093 |
| FPG (mmol/L) | 4.95 ± 0.82 | 9.25 ± 3.67 | < 0.001 |
| TG (mmol/L) | 2.46 ± 1.98 | 2.40 ± 2.07 | 0.596 |
| TC (mmol/L) | 4.31 ± 1.70 | 4.63 ± 1.36 | < 0.001 |
| HDL (mmol/L) | 1.25 ± 0.33 | 0.94 ± 0.32 | < 0.001 |
| LDL (mmol/L) | 2.99 ± 0.81 | 2.81 ± 0.90 | < 0.001 |
| AST (U/L) | 21.94 ± 18.18 | 24.82 ± 29.87 | 0.019 |
| ALT (U/L) | 29.30 ± 34.33 | 35.20 ± 52.66 | 0.011 |
Genotype and allele frequency distribution of each SNP in the type 2 diabetes mellitus group and in the control group
The genotype distribution of each SNP in the control group was in accordance with Hardy-Weinberg balance (P > 0.05). The genotype and allele frequency distributions of each SNP in the two groups are illustrated in Figure 1 and Table 2. Significant differences in genotype distribution of rs7195539 and rs9939609 in the two groups (P = 0.015, 0.025) were found. The A allele frequency of rs8050136 and rs9939609 in the type 2 diabetes mellitus group was higher than that in the control group (P = 0.027, 0.006).
Figure 1.
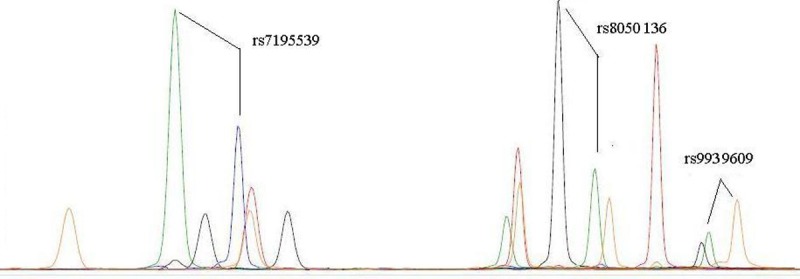
rs9939609, rs8050136, rs7195539 genotype in the type 2 diabetes mellitus group. Note: (ddGTP = blue peak; ddATP = green peak; ddTTP = red peak; ddCTP = black peak).
Table 2.
Genotype and allele frequency distribution of each SNP in the type 2 diabetes mellitus group and in the control group
| SNP | Group | Genotype n (%) | HWE P | P value | Allele n (%) | P value | OR (95% CI) | |||
|---|---|---|---|---|---|---|---|---|---|---|
| rs7195539 | A/A | A/G | G/G | A | G | |||||
| Control | 787 (90.1) | 85 (9.7) | 1 (0.1) | 0.404 | 0.015 | 1659 (95.0) | 87 (5.0) | 0.226 | 1.220 (0.884-1.683) | |
| Case | 785 (92.5) | 58 (6.8) | 6 (0.7) | 1628 (95.9) | 70 (4.1) | |||||
| rs8050136 | C/C | C/A | A/A | C | A | |||||
| Control | 460 (52.7) | 348 (39.9) | 65 (7.4) | 0.942 | 0.084 | 1268 (72.6) | 478 (27.4) | 0.027 | 1.181 (1.019-1.368) | |
| Case | 409 (48.2) | 357 (42.0) | 83 (9.8) | 1175 (69.2) | 523 (30.8) | |||||
| rs9939609 | T/T | T/A | A/A | T | A | |||||
| Control | 443 (50.7) | 350 (40.2) | 80 (9.2) | 0.367 | 0.025 | 1236 (70.8) | 510 (29.2) | 0.006 | 1.225 (1.060-1.415) | |
| Case | 382 (45.0) | 364 (42.9) | 103 (12.1) | 1128 (66.4) | 570 (33.6) | |||||
HWE: Hardy-Weinberg equilibrium; OR: odd ratio; CI: confidence interval; HWE: Hardy-Weinberg equilibrium; OR: odd ratio; CI: confidence interval.
Genotype distribution of each SNP in two groups with different BMI levels, and comparison of BMI (kg/m2) of each SNP with different genotypes
After stratification of BMI according to normal, overweight and obesity, significant differences were found in the distribution frequency of rs9939609 genotype in the type 2 diabetes subgroup and in the control subgroup both belonging to the normal BMI group (P = 0.044) (Table 3). The BMI of the group with C/A+A/A genotype of rs8050136 in the whole population and type 2 diabetes group was bigger than that of C/C group (P < 0.05), and the BMI of the group with T/A+A/A genotype of rs9939609 was higher than that of T/T group (P < 0.05) (Table 4).
Table 3.
Genotype distribution of each SNP in the type 2 diabetes mellitus group and in the control group with different BMI levels
| SNP | Group | Control n (%) | Case n (%) | P value | ||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| A/A | A/a | a/a | A/A | A/a | a/a | |||
| rs7195539 | Normal | 136 (92.5) | 11 (7.5) | 0 | 112 (92.6) | 9 (7.4) | 0 | 0.989 |
| Overweight | 280 (90.9) | 27 (8.8) | 1 (0.3) | 239 (91.2) | 22 (8.4) | 1 (0.4) | 0.982 | |
| Obesity | 252 (92.3) | 21 (7.7) | 0 | 390 (94.0) | 21 (5.1) | 4 (1.0) | 0.052 | |
| rs8050136 | Normal | 80 (54.4) | 58 (39.5) | 9 (6.1) | 70 (57.9) | 36 (29.8) | 15 (12.4) | 0.089 |
| Overweight | 167 (54.2) | 118 (38.3) | 23 (7.5) | 121 (46.2) | 116 (44.3) | 25 (9.5) | 0.153 | |
| Obesity | 142 (52.0) | 103 (37.7) | 28 (10.3) | 195 (47.0) | 180 (43.4) | 40 (9.6) | 0.335 | |
| rs9939609 | Normal | 75 (51.0) | 60 (40.8) | 12 (8.2) | 65 (53.7) | 36 (29.8) | 20 (16.5) | 0.044 |
| Overweight | 159 (51.6) | 119 (38.6) | 30 (9.7) | 113 (43.1) | 118 (45.0) | 31 (11.8) | 0.128 | |
| Obesity | 140 (51.3) | 105 (38.5) | 28 (10.3) | 185 (44.6) | 186 (44.8) | 44 (10.6) | 0.206 | |
Normal: BMI < 24 kg/m2, Overweight: 24 kg/m2 ≤ BMI < 28 kg/m2. Obesity: BMI ≥ 28 kg/m2. AA: wild type homozygote; Aa: heterozygote; aa: homozygous mutant.
Table 4.
Comparison of BMI (kg/m2) of each SNP with different genotypes in the whole population, in the type 2 diabetes group and in the control group
| SNP | Whole | Control | Case | |||
|---|---|---|---|---|---|---|
|
|
|
|
||||
| A/A | A/a + a/a | A/A | A/a + a/a | A/A | A/a + a/a | |
| rs7195539 | 27.77 ± 4.39 | 27.16 ± 4.52 | 27.08 ± 3.97 | 26.54 ± 3.46 | 28.38 ± 4.65 | 27.82 ± 5.37 |
| rs8050136 | 27.31 ± 4.21 | 28.15 ± 4.55* | 26.86 ± 3.86 | 27.24 ± 4.00 | 27.76 ± 4.49 | 28.89 ± 4.84* |
| rs9939609 | 27.38 ± 4.20 | 28.04 ± 4.55* | 26.94 ± 3.86 | 27.14 ± 4.01 | 27.82 ± 4.49 | 28.78 ± 4.84* |
AA: wild type homozygote; Aa: heterozygote; aa: homozygous mutant.
P < 0.05.
Discussion
FTO gene is a gene related to fat mass and obesity discovered in white race by Frayling et al. [2] in 2007. This gene is located on chromosome 16q12.2, possesses a total length of about 430 kb and contains 9 exons and 8 introns. The encoded product of the FTO gene is a member of the non-heme dioxygenase superfamily [16], which is highly similar to Escherichia coli ALKB enzyme and human ABH family. Mouse FTO protein also possesses similar double stranded β-folding structure, which contains 4 conserved residues that can interact with Fe2+ and 2-oxoglutarate [17], both important for the function of the FTO protein. 2-ketoglutaric acid oxygenase is involved in many reactions such as DNA repair, fatty acid metabolism and post translational modification. Fe2+ uses oxygen as a cofactor. Rat recombinant FTO protein can catalyze demethylation of 3-methylthymidine in the single stranded DNA under conditions of Fe2+ and 2-oxoglutarate [18]. Fawcett et al. reported that the demethylation of FTO might regulate the expression of genes related to some metabolic processes, and their dysregulation may be related to type 2 diabetes, although the specific molecular mechanism is still not clear [19]. Moreover, the mutation of FTO gene leads to a lack of control of the appetite and consequent morbid hunger, increased ingestion reflex, inhibition of metabolism and reduced energy consumption efficiency, all symptoms that may lead to obesity. Gerken et al. found a high expression of FTO mRNA in the brain tissues of wild mice, especially in the hypothalamic area where it reaches the highest concentration [18]. The hypothalamic area plays critical roles in the control of energy balance, thus indicating that the FTO gene may regulate the pathogenesis and development of obesity mainly through its effect on hypothalamic energy centre.
The present study shows that the levels of BMI, WL, SBP, DBP, FPG, TC, AST and ALT in the type 2 diabetes group were higher than those in the control group (P < 0.05), suggesting that type 2 diabetes was associated with abdominal obesity, hypertension, dyslipidemia, non-alcoholic fatty liver and other abnormal metabolism dysfunctions, which may be considered to be related to insulin resistance (IR). The HDL and LDL levels in Type 2 diabetes mellitus group were lower than those in the control group (P < 0.05), with no significant difference of TG between the two groups. These effects may be both associated with lipid regulating agents’ treatment because of the combined dyslipidemia and atherosclerosis.
In the current research, the BMI of the genotype C/A+A/A of rs8050136 group in the whole population and the type 2 diabetes group was bigger than that of C/C group, and the level of BMI of the genotype T/A+A/A of rs9939609 group was higher than that of the T/T group (P < 0.05), indicating that the rs8050136 and rs9939609 gene polymorphism was correlated with the obesity of Uygur people, as it was confirmed in many studies [8,3,10,20-22].
In the present study, the frequency of the A allele of rs8050136 was 29.1%, and the frequencies of the A allele of the Chinese and the Europeans in the HapMap database were 13.9% and 46% respectively. The frequency of the allele A of rs9939609 was 31.4%, and the frequencies of the Chinese and the Europeans in the HapMap database were 15% and 46%, suggesting that the rs8050136 and rs9939609 allele frequency risk in the Uygur people was between that of the Han population of China and the European population. Moreover, the genotype frequency distribution of rs8050136 and rs9939609 of FTO displayed racial and regional differences. The differences of gene frequency between the races may partly explain the different results obtained in the study of different races Furthermore, the interaction of gene-environment may be one of the causes of the distribution difference.
In summary, the single nucleotide mutation of rs7195539 in FTO gene may be a protective factor of Uygur type 2 diabetes. The single nucleotide mutations of rs8050136 and rs9939609 may be associated with the Uygur type 2 diabetes and obesity, with A as the risk allele. The correlation of the rs8050136gene polymorphism with type 2 diabetes mellitus may be mediated by BMI, while the association between rs9939609 gene polymorphism and type 2 diabetes is not depending from BMI.
Acknowledgements
This work was supported by grant 2012CB722403 from the national 973 science and technology project.
Disclosure of conflict of interest
None.
References
- 1.Yang W, Ji Q, Zhu D, Weng J, Jia W, Ji L, Xiao J, Shan Z, Liu J, Tian H, Ge J, Lin L, Chen L, Guo X, Zhao Z, Li Q, Zhou Z, Shan G, He J China National Diabetes and Metabolic Disorders Study Group. Prevalence of diabetes among men and women in China. N Engl J Med. 2010;362:1090–1101. doi: 10.1056/NEJMoa0908292. [DOI] [PubMed] [Google Scholar]
- 2.Frayling TM, Timpson NJ, Weedon MN, Zeggini E, Freathy RM, Lindgren CM, Perry JR, Elliott KS, Lango H, Rayner NW, Shields B, Harries LW, Barrett JC, Ellard S, Groves CJ, Knight B, Patch AM, Ness AR, Ebrahim S, Lawlor DA, Ring SM, Ben-Shlomo Y, Jarvelin MR, Sovio U, Bennett AJ, Melzer D, Ferrucci L, Loos RJ, Barroso I, Wareham NJ, Karpe F, Owen KR, Cardon LR, Walker M, Hitman GA, Palmer CN, Doney AS, Morris AD, Smith GD, Hattersley AT, McCarthy MI. A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Science. 2007;316:889–894. doi: 10.1126/science.1141634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Scott LJ, Mohlke KL, Bonnycastle LL, Willer CJ, Li Y, Duren WL, Erdos MR, Stringham HM, Chines PS, Jackson AU, Prokunina-Olsson L, Ding CJ, Swift AJ, Narisu N, Hu T, Pruim R, Xiao R, Li XY, Conneely KN, Riebow NL, Sprau AG, Tong M, White PP, Hetrick KN, Barnhart MW, Bark CW, Goldstein JL, Watkins L, Xiang F, Saramies J, Buchanan TA, Watanabe RM, Valle TT, Kinnunen L, Abecasis GR, Pugh EW, Doheny KF, Bergman RN, Tuomilehto J, Collins FS, Boehnke M. A genome-wide association study of type 2 diabetes in Finns detects multiple susceptibility variants. Science. 2007;316:1341–1345. doi: 10.1126/science.1142382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Yajnik CS, Janipalli CS, Bhaskar S, Kulkarni SR, Freathy RM, Prakash S, Mani KR, Weedon MN, Kale SD, Deshpande J, Krishnaveni GV, Veena SR, Fall CH, McCarthy MI, Frayling TM, Hattersley AT, Chandak GR. FTO gene variants are strongly associated with type 2 diabetes in South Asian Indians. Diabetologia. 2009;52:247–252. doi: 10.1007/s00125-008-1186-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hertel JK, Johansson S, Sonestedt E, Jonsson A, Lie RT, Platou CG, Nilsson PM, Rukh G, Midthjell K, Hveem K, Melander O, Groop L, Lyssenko V, Molven A, Orho-Melander M, Njølstad PR. FTO, type 2 diabetes, and weight gain throughout adult life: a meta-analysis of 41,504 subjects from the Scandinavian HUNT, MDC, and MPP studies. Diabetes. 2011;60:1637–1644. doi: 10.2337/db10-1340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Horikoshi M, Hara K, Ito C, Shojima N, Nagai R, Ueki K, Froguel P, Kadowaki T. Variations in the HHEX gene are associated with increased risk of type 2 diabetes in the Japanese population. Diabetologia. 2007;50:2461–2466. doi: 10.1007/s00125-007-0827-5. [DOI] [PubMed] [Google Scholar]
- 7.Qian Y, Liu S, Lu F, Li H, Dong M, Lin Y, Du J, Lin Y, Gong J, Jin G, Dai J, Hu Z, Shen H. Genetic variant in fat mass and obesity-associated gene associated with type 2 diabetes risk in Han Chinese. BMC Genet. 2013;14:86. doi: 10.1186/1471-2156-14-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Frayling TM, Timpson NJ, Weedon MN, Zeggini E, Freathy RM, Lindgren CM, Perry JR, Elliott KS, Lango H, Rayner NW, Shields B, Harries LW, Barrett JC, Ellard S, Groves CJ, Knight B, Patch AM, Ness AR, Ebrahim S, Lawlor DA, Ring SM, Ben-Shlomo Y, Jarvelin MR, Sovio U, Bennett AJ, Melzer D, Ferrucci L, Loos RJ, Barroso I, Wareham NJ, Karpe F, Owen KR, Cardon LR, Walker M, Hitman GA, Palmer CN, Doney AS, Morris AD, Smith GD, Hattersley AT, McCarthy MI. A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Science. 2007;316:889–894. doi: 10.1126/science.1141634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zeggini E, Weedon MN, Lindgren CM, Frayling TM, Elliott KS, Lango H, Timpson NJ, Perry JR, Rayner NW, Freathy RM, Barrett JC, Shields B, Morris AP, Ellard S, Groves CJ, Harries LW, Marchini JL, Owen KR, Knight B, Cardon LR, Walker M, Hitman GA, Morris AD, Doney AS Wellcome Trust Case Control Consortium (WTCCC) McCarthy MI, Hattersley AT. Replication of genome-wide association signals in UK samples reveals risk loci for type 2 diabetes. Science. 2007;316:1336–1341. doi: 10.1126/science.1142364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Scuteri A, Sanna S, Chen WM, Uda M, Albai G, Strait J, Najjar S, Nagaraja R, Orrú M, Usala G, Dei M, Lai S, Maschio A, Busonero F, Mulas A, Ehret GB, Fink AA, Weder AB, Cooper RS, Galan P, Chakravarti A, Schlessinger D, Cao A, Lakatta E, Abecasis GR. Genome-wide association scan shows genetic variants in the FTO gene are associated with obesity-related traits. PLoS Genet. 2007;3:e115. doi: 10.1371/journal.pgen.0030115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Puavilai G, Chanprasertyotin S, Sriphrapradaeng A. Diagnostic criteria for diabetes mellitus and other categories of glucose intolerance: 1997 criteria by the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (ADA), 1998 WHO consultation criteria, and 1985 WHO criteria. World Health Organization. Diabetes Res Clin Pract. 1999;44:21–26. doi: 10.1016/s0168-8227(99)00008-x. [DOI] [PubMed] [Google Scholar]
- 12.Chen C, Lu FC Department of Disease Control Ministry of Health, PR China. Guidelines for Prevention and Control of Overweight and Obesity in Chinese Adults. Biomed Environ Sci. 2004;17(Suppl):1–36. [PubMed] [Google Scholar]
- 13.Sanchez-Pulido L, Andrade-Navarro MA. The FTO (fat mass and obesity associated) gene codes for a novel member of the non-heme dioxygenase superfamily. BMC Biochem. 2007;8:23. doi: 10.1186/1471-2091-8-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Clifton IJ, Mcdonough MA, Ehrismann D, Kershaw NJ, Granatino N, Schofield CJ. Structural studies on 2-oxoglutarate oxygenases and related double-stranded beta-helix fold proteins. J Inorg Biochem. 2006;100:644–669. doi: 10.1016/j.jinorgbio.2006.01.024. [DOI] [PubMed] [Google Scholar]
- 15.Gerken T, Girard CA, Tung YC, Webby CJ, Saudek V, Hewitson KS, Yeo GS, McDonough MA, Cunliffe S, McNeill LA, Galvanovskis J, Rorsman P, Robins P, Prieur X, Coll AP, Ma M, Jovanovic Z, Farooqi IS, Sedgwick B, Barroso I, Lindahl T, Ponting CP, Ashcroft FM, O’Rahilly S, Schofield CJ. The obesity-associated FTO gene encodes a 2-oxoglutarate-dependent nucleic acid demethylase. Science. 2007;318:1469–1472. doi: 10.1126/science.1151710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fawcett KA, Barroso I. The genetics of obesity: FTO leads the way. Trends Genet. 2010;26:266–274. doi: 10.1016/j.tig.2010.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gerken T, Girard CA, Tung YC, Webby CJ, Saudek V, Hewitson KS, Yeo GS, McDonough MA, Cunliffe S, McNeill LA, Galvanovskis J, Rorsman P, Robins P, Prieur X, Coll AP, Ma M, Jovanovic Z, Farooqi IS, Sedgwick B, Barroso I, Lindahl T, Ponting CP, Ashcroft FM, O’Rahilly S, Schofield CJ. The obesity-associated FTO gene encodes a 2-oxoglutarate-dependent nucleic acid demethylase. Science. 2007;318:1469–1472. doi: 10.1126/science.1151710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Scuteri A, Sanna S, Chen WM, Uda M, Albai G, Strait J, Najjar S, Nagaraja R, Orrú M, Usala G, Dei M, Lai S, Maschio A, Busonero F, Mulas A, Ehret GB, Fink AA, Weder AB, Cooper RS, Galan P, Chakravarti A, Schlessinger D, Cao A, Lakatta E, Abecasis GR. Genome-wide association scan shows genetic variants in the FTO gene are associated with obesity-related traits. PLoS Genet. 2007;3:e115. doi: 10.1371/journal.pgen.0030115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chang YC, Liu PH, Lee WJ, Chang TJ, Jiang YD, Li HY, Kuo SS, Lee KC, Chuang LM. Common variation in the fat mass and obesity-associated (FTO) gene confers risk of obesity and modulates BMI in the Chinese population. Diabetes. 2008;57:2245–2252. doi: 10.2337/db08-0377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Legry V, Cottel D, Ferrieres J, Arveiler D, Andrieux N, Bingham A, Wagner A, Ruidavets JB, Ducimetière P, Amouyel P, Meirhaeghe A. Effect of an FTO polymorphism on fat mass, obesity, and type 2 diabetes mellitus in the French MONICA Study. Metabolism. 2009;58:971–975. doi: 10.1016/j.metabol.2009.02.019. [DOI] [PubMed] [Google Scholar]
- 21.Price RA, Li WD, Zhao H. FTO gene SNPs associated with extreme obesity in cases, controls and extremely discordant sister pairs. BMC Med Genet. 2008;9:4. doi: 10.1186/1471-2350-9-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hunt SC, Stone S, Xin Y, Scherer CA, Magness CL, Iadonato SP, Hopkins PN, Adams TD. Association of the FTO gene with BMI. Obesity (Silver Spring) 2008;16:902–904. doi: 10.1038/oby.2007.126. [DOI] [PMC free article] [PubMed] [Google Scholar]