

Abstract
To analyze the characteristics and treatment of middle-super thoracic fractures associated with the sternum fracture, twenty six patients with middle-super thoracic fractures associated with the sternum fracture were retrospectively reviewed. The intimate information of patients including age, gender, cause of injury, site of the sternal fracture, level and type of thoracic vertebral fracture, spinal cord injury and associated injuries were included in the analysis. There were 12 compressed fractures, 11 fracture-dislocations, two burst fracture and one burst-dislocation in this study. Six patients had a complete lesion of the spinal cord, nine sustained a neurologically incomplete injury and 11 were neurologically intact. Nine patients were treated non-operatively and 17 were underwent surgery. All patients were followed up for 8~99 months. Our results showed that road traffic accidents (RTA) and fall were the dominated in the causes. All six patients with a complete paralytic lesion were not recovered with any significant function. Four out of eleven neurologically intact patients had local pain although ten of them remained normal function and one patient turn up tardive paralysis. One of nine patients with incomplete paraplegia returned to normal and four recovered with some function. These study suggested that the sternum is one of the important parts in constructing thoracic cage and plays an important role in maintain the stabilization of the thoracic vertebra. Because of the unique anatomy and biomechanics of the thoracic cage, the classification commonly applied to thoracic vertebra fractures is not suitable for middle-super thoracic fractures associated with the sternum fracture. Middle-super thoracic fractures associated with the sternum fracture was marked by violent force, severe fractures of spine, severe injuries of spinal cord and high incidence of associated injuries. These cases confirm the existence and clinical relevance of the fourth column of the thoracic spine and its role for spinal stability in the patient with middle-super thoracic fracture.
Keywords: Thoracic vertebral fractures, sternal fractures, thoracic cage
Introduction
Thoracic vertebra is different from cervical vertebra, thoracolumbar vertebra and lumbar vertebra, due to the particularity of its own physiological structure. Thoracic vertebra has 12 centrums to bear the compression load: the vertebral arch is the major parts to bear the tension load while the vertebral plate is short but wide, which can prevent the hyperextension activity of the thoracic vertebra. The articular surface of the zygapophyseal joint is coronary, which allows the thoracic vertebra to take a certain range of axial rotation and has a strong resistance to the onward dislocation. The vertebra, intervertebral disc and ligament jointly maintain the stability of the thoracic vertebra. The stability of the thoracic vertebra is obviously higher than that of thoracolumbar vertebra and other spine areas, which shall mainly be credited to the existence of thoracic cage. In the front, the sternocostal joint was composed of costal cartilage and sternum; in the back, the joint was composed of rid head and the corresponding centrum, intervertebral disc and transverse process.
The middle-super thoracic fractures associated with the sternum fracture are often found in severe trauma. In recent years, as the clinical report and research on biomechanical function of thoracic ring go deeper, the knowledge on the middle-super thoracic fractures associated with the sternum fracture in the aspects of anatomy, injury mechanism and clinical treatment has been deepened. From May 1996 to November 2007, our hospital have totally received and cured 26 patients of the middle-super thoracic fractures associated with the sternum fracture. Now the medical information is retrospectively analyzed as follows.
Material and methods
General information
Our department have totally received and cured 26 patients, who suffered from the middle-super thoracic fractures associated with the sternum fracture from May 1996 to November 2007. Nineteen of them were male and seven of them were female; with an average age of 36.3, they were at the age of 17~71; the time from being injured to being treated was 30 min~24 d.
Causes of injury
18 cases were caused by traffic accident, 6 cases were caused by falling accident and 2 cases were caused by other accidents. This group of data is excluded the cases of pathological fracture (including osteoporosis fracture).
Distribution of fractures
The T1 fracture characteristics were similar to that of cervical spinal fracture while T11 and T12 fractures shall be classified into the injury scope of thoracolumbar vertebra; therefore, they were excluded in the statistics. To be specific, there were 2 cases of T2 fracture, 3 cases of T3 fracture, 3 cases of T4 fracture, 5 cases of T5 fracture, 6 cases of T6 fracture, 7 cases of T7 fracture, 4 cases of T8 fracture, 3 cases of T9 fracture and 2 cases of T10 fracture (according to the statistics by the vertebral involvement, among the 26 cases, there were 35 vertebras in total). Furthermore, there were 2 cases with more than 3 vertebras involved, 5 cases with 2 vertebras involved and 19 cases with one vertebra involved. Moreover, there were 2 cases of jumping fracture, 2 cases associated with lumbar fracture and 1 case of sacrum fracture. In addition, there were 17 cases with sternum fracture taking place on mesosternum, 5 cases with sternum fracture taking place on manubrium, 2 cases of manubrium separation and 2 cases with sternum fracture taking place on xiphoid process.
Classification of thoracic fractures
According to the classification of Hanley-Eskay, there were 12 cases of compression fracture, 11 cases of fracture dislocation, 2 cases of burst fracture and 1 case of burst dislocation.
Degree of spinal cord injury
There were 6 cases of complete nerve damage, 9 cases of incomplete nerve damage and 11 cases without nerve damage. According to the Frankel standards, there were 6 cases of Grade A, 3 cases of Grade B, 2 cases of Grade C, 4 cases of Grade D and 11 cases of Grade E. All the 26 cases were associated with different degrees of kyphosis angulation and deformity: the angle was 6°~42° and the average kyphotic angle was 21°.
Associated injury
All the 26 cases were associated with different degrees of rib fracture. Specifically, there were 8 cases associated with pulmonary contusion, 12 cases associated with hemopneumothorax, 1 case associated with mediastinum injury, 2 cases associated with abdominal visceral injury, 3 cases associated with clavicle fracture and 1 case associated with comminuted fracture of the left ulna olecranon.
Therapeutic methods
The main reference basis for us to select the therapeutic methods included thoracic fracture compression dislocation, spinal nerve trauma, thoracic kyphotic deformity, sternum fracture dislocation and associated injury.
Treatment of associated injury
Among the 12 cases associated with hemopneumothorax, 10 cases accepted the thoracic close drainage and 1 case accepted the ventilator support treatment. The 8 cases associated with pulmonary contusion accepted the treatments of enhancement for resistance to infection, aerosol inhalation, dieresis, a moderate amount of transfusion of whole blood or plasma, oxygen uptake, sputum suction, etc.; meanwhile, 1 case accepted the treatment of tracheal incision to place the tracheal tube. The 1 case associated with abdominal visceral injury accepted the exploratory laparotomy. All the cases associated with clavicle fracture accepted the non-surgical treatment. Moreover, the 1 case associated with comminuted fracture of the left ulna olecranon accepted the surgery of open reduction and internal fixation.
Non-surgical treatment (9 cases)
The cases of thoracic injury were minor so that with the reduction by the sternum fracture dislocation technique applied, the front of the sternum was padded with “cross-shaped” wide tape for fixation and the spine shall be hyper-extended appropriately; the patient then shall rest in bed for a short time to take breathing and functional exercises; with the symptomatic treatment supplemented, 1~2 weeks later, the patient can take a sit under the protection of the support or get around in a wheelchair. The 2 cases of associated injury were too serious to carry out the surgical treatment so that the life-threatening associated injury was treated first and the time in bed was extended with the bedside care strengthened. In addition, due to the economic reason, 1 case refused the surgical treatment.
Surgical treatment
Among the 17 cases, 12 cases accepted the posterior surgery. Both before and in the surgery, all the patients accepted the C arm machine positioning. Under the endotracheal intubation anesthesia and in the prone position, the patients accepted the surgery through the posterior median approach. According to different types of fracture and spinal cord injury, the lamina resection or spinal canal ring/secondary ring decompression was applied and then the bone graft fusion and internal fixation by instrument were applied to the lamina intertransverse process or vertebral body. 1 patient of T5 vertebral compression fractures associated with sternum fracture, for whom the non-surgical treatment was applied, accepted the surgery of anterior decompression intervertebral bone graft and internal fixation four months after the injury due to the late-onset neural dysfunction. Among the 12 cases of posterior surgery, 5 cases accepted the surgery of open reduction and internal fixation for the sternum fracture: specifically, there were 3 cases for the mesosternum, 1 case for the manubrium fracture and 1 case for the mesosternum separation. In addition, 4 cases of thoracic stable fracture only accepted the surgery of surgery of open reduction and internal fixation for the sternum fracture while the associated thoracic fractures adopted the non-surgical treatment. Moreover, among the 9 cases of surgical treatment for the sternum fracture, 7 cases adopted steel plate for internal fixation, 1 case adopted steel wire for fixation and 1 case adopted kirschner pin for fixation (Figure 1).
Figure 1.
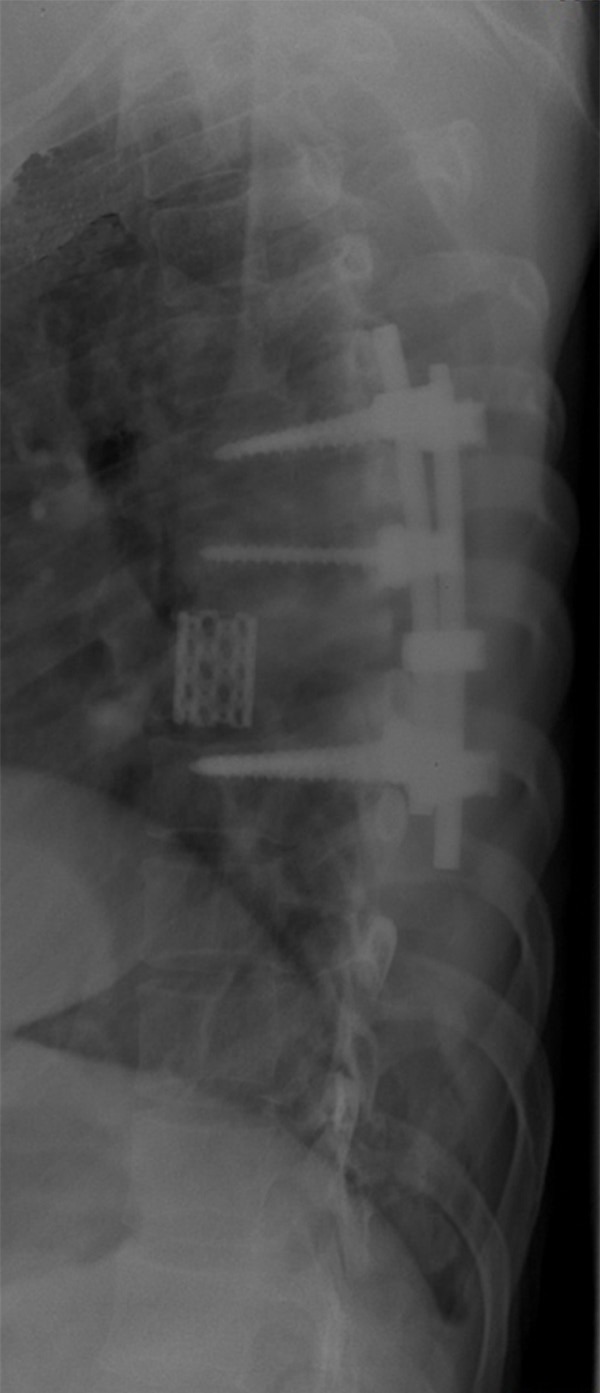
The typical case after surgical treatment with adopted kirschner pin for fixation.
Results
This group of patients was hospitalized for an average of 18.4 d (5~26 d): 2 patients suffered from mild wound infection during the hospitalization and 1 patient suffered from associated pulmonary infection upon the pulmonary contusion, who, after the anti-inflammatory support and symptomatic treatment, was healed. Before and after the surgery, all the 12 patients accepting the thoracic posterior surgery took the routine X-ray film and CT scanning and 10 of then took the MRI examination: it was found that the fracture dislocation reduction was satisfactory; the anterior height of the injured vertebra was restored from the average 56% before the surgery to 82% after the surgery; the spinal kyphotic deformity was averagely 11° corrected. The 26 patients were followed up for 8~99 months with an average follow-up of 35.8 months (including 1 patient, who died of rectal cancer 3 years after the follow-up visit). Among the 6 patients suffering from complete nerve damage, no one got better while among the 9 patients suffering from incomplete nerve damage, 1 patient returned to normal, 4 patients got better and the rest four patients remained unchanged. Among the 11 patients without nerve damage, 1 patient suffered from the late-onset neural dysfunction and the rest did not suffered from the disease progression; however, 4 patients still suffered from localized chest and back pain. There were different degrees of loss for the anterior height of the injured vertebra: the loss in the cases accepting the non-surgical treatment was most obvious, which was averagely 27%; the average loss in the cases of the pure sternum surgery was 12%; the average loss in the cases of the pure thoracic surgery was 8%; the average loss in the cases of the combined surgery for thoracic vertebra and sternum was less than 3%. There were different degrees of aggravation for the spinal kyphotic deformity: specifically, the aggravation on the cases accepting the non-surgical treatment was most obvious, which was averagely most obvious; the average aggravation on the cases accepting the pure sternum surgery was 9°; the average aggravation on the cases accepting the pure thoracic surgery was 5°; the average aggravation on the cases accepting the combined surgery for thoracic vertebra and sternum was 2°.
Discussion
In 1983, Denis put forward the classification system for the spinal three-column theory, who believed that the injury involved more than 2 columns would lead to the potential instability of the spine. In 1993, based on the review for two cases, Berg [1] put forward the concept for the first time to take the thoracic cage composed of sternum, rib and sternocostal joint as the fourth column of the thoracic vertebra so as to strengthen the special function of the thoracic cage to stabilize the thoracic vertebra. Afterwards, some scholars in succession carried out demonstrations [2-5] on this concept.
Meanwhile, the case report, retrospective analysis and biomechanical study associated with the concept that the thoracic cage would stabilize the thoracic vertebra could also be found in the literature [6-13]. These studies provided mechanical basis for the fourth column theory of the thoracic vertebra.
Due to the existence of the thoracic cage, the stability of the thoracic vertebra is higher than that of the thoracolumbar vertebra and lumbar vertebra, whose incidence of fracture is, hence, relatively low. However, once the fracture occurs, the violence resulting into injury will tend to be more powerful so that the fracture will also be more serious, which sometimes will involve multiple segments and often will be accompanied by the injury to other visceral organs and the fracture to other parts. Based on our study, it can be seen that traffic injury and fall injury dominated in the cause while compression fracture and fracture dislocation dominated in the caused injury; different from lumbar fracture or thoracolumbar fracture, the latter is featured by burst fracture. The thoracic vertebra canal is relatively narrow so that when the bone structure is damaged, the incidence of the spinal cord injury will also be relatively high.
Clinically, the sternum fracture is relatively rare, which can be caused by direct violence or indirect force. The rib can transfer the violence from the spine to the sternum. On the contrary, when the lumbar vertebra and thoracolumbar spine suffer from the extreme flexion, the mesosternum will sustain the upward and onward pressure from the low-level ribs. The thoracic fractures associated with sternum fracture are the result of huge violent actions, including flexion, axial pressure, rotating external force and onward shear force. These acting forces can occur at the same time and in succession. The victims of the traffic injury generally will be in the driving position or wear the seat belt so that the violence, on the one hand, will be imposed on the sternum directly through the steering wheel or seat belt, and, on the other hand, will be imposed on the head and neck or upper back so that the upper spine will suffer from over-flexion compression: through the first & second ribs and clavicle (probably including the mentum), the violence will be conveyed to the sternum to force the manubrium to generate the downward and backward movements, which will result into the fracture or dislocation of the spine and sternum. For the victims of the fall injury, after falling, their hip usually will strike the ground first so that the violence will be imposed on the lower spine and make it buckled, and then the posterior abdominal wall will go against the thoracic cage while the lower ribs will generate upward impact, which thus will result into the sternum fracture [4].
The incidence of the thoracic fractures associated with sternum fracture is low: the relevant reports in the literature are significantly different, ranging from “1.4%~18.5%” [14-17]; meanwhile, most of them are found in the severe trauma; usually, they will be associated with rib fracture, hemopneumothorax, pulmonary contusion, mediastinum injury, cardiac contusion, etc [17]. In our study, this group of cases is majorly associated with rib fracture, hemopneumothorax and pulmonary contusion. The injured thoracic cage is poor in stability and the proportion for the formation of flail chest is high so that the patient might suffer from the paradoxical respiration, which will lead to the respiratory and circulatory collapse within a short time. If the thoracoabdominal organ injury is associated, the condition will become more complex and dangerous. Therefore, once the sternum fracture occurs, the condition generally will be serious so that the patient shall be diagnosed in a timely manner and fixed appropriately so as to treat the life-threatening thoracoabdominal organ injury.
Most of the studies suggested that it was still necessary to fix and stabilize the spine in order to create conditions for the recovery of the spinal cord functions although it was impossible to restore the spinal cord functions. They believed that the stabilized spine could facilitate nursing care and rehabilitation, as well as could reduce the series of complications brought about by bed rest, which was conducive to the rapid recovery of the limb functions. Furthermore, the recovery of the postoperative thoracic physiological kyphosis would be helpful to relieve local pain. In our study, 6 cases with complete nerve damage in this group, no patient got recovered after the surgery; however, through the decompression surgery, some cases with incomplete nerve damage got different degrees of recovery. Moreover, the hospitalized time of the patients accepting the thoracic surgery was shortened so that the incidence of bedsore and other complications was reduced and the postoperative life quality was improved. These results indicated that for the unstable thoracic fractures associated with incomplete nerve damage, it is necessary to take the aggressive surgery of decompression, fixation and fusion. It will be helpful to restore the normal sequence and stability of the spine. Furthermore, it can create conditions for the recovery of the spinal cord functions. With regard to the unstable thoracic fractures associated with complete nerve damage, the author thinks that, at least, it is necessary to take the surgery of fusion and fixation for the spine. These results are consistant with other studies by Cooper [18], Lund [5] and Klaase [19].
In our study, all of the 26 cases were involved with the spinal kyphotic deformity (with an average kyphotic angle of 21°): although after the thoracic surgery, the kyphotic deformity was corrected to some extent, whether the surgery was applied or not, the spinal kyphotic deformity was aggravated by different degrees in the long-term follow-up visits. It was worth noting that the aggravation degree of the thoracic kyphotic deformity of the patients suffering from the sternum fracture and accepting the fixation treatment was lesser (see above). Therefore, for this special type of injury, it is necessary to take full considerations to the fracture type and stability, to check whether the spinal cord injury is associated or not (if it is, what is the degree) and to check whether there are other associated injuries (if there are, what is the degree); in addition, it is necessary to take thoracic cage and thoracic vertebra as an organic whole and include it into the consideration scope of treatment.
In this study, 4 of the 6 cases with complete spinal cord injury in this group, 4 patients accepted the spinal canal ring decompression and 2 patients accepted the pure spinal fusion & fixation: in the long-term postoperative follow-up visit, no one was found with the recovery of the nerve functions. However, after the surgery, the local pain was relieved and the bed rest time was shortened so that the quality of life was improved. It is suggested that the decompression surgery shall not be carried out at the same time, especially for the anterior decompression surgery, so as to avoid unnecessary trauma. With regard to the treatment of sternum fracture, the steel wire binding or Kirschner pin or Steinmann pin usually would be adopted for fixation in the past. In this study, 9 cases of the surgical treatment for sternum fracture, 7 patients adopted steel plate for internal fixation, 1 patient adopted steel wire for fixation and 1 patient adopted Kirschner pin for fixation. What we have learnt is that taking steel plate for fix at ion will be optimal for the patient with manubrium/meso sternum fracture or serious manubrium separation & dislocation. The steel plate is featured by strong tension stress and firm fixation so that there is no need for external fixation after the surgery, which is helpful for the early recovery of the respiratory function.
The middle-super thoracic fractures associated with the sternum fracture are caused by high-energy injury, as well as might easily be developed into severe deformity and nerve dysfunction. However, the existence of the complete fourth column is of great clinical significance for these cases. The deepening of the theoretical understanding on the fourth column of the thoracic vertebra can help us to improve the treatment level for the external injury, as well as can help us to cope with the thoracic deformity correction, phyma excision, spinal infection, congenital deformity and may other clinical problems.
Disclosure of conflict of interest
None.
References
- 1.Berg EE. The sternal-rib complex. A possible fourth column in thoracic spine fractures. Spine (Phila Pa 1976) 1993;18:1916–1919. [PubMed] [Google Scholar]
- 2.Vioreanu MH, Quinlan JF, Robertson I, O’Byrne JM. Vertebral fractures and concomitant fractures of the sternum. Int Orthop. 2005;29:339–342. doi: 10.1007/s00264-005-0001-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shen FH, Samartzis D. Successful nonoperative treatment of a three-column thoracic fracture in a patient with ankylosing spondylitis: existence and clinical significance of the fourth column of the spine. Spine (Phila Pa 1976) 2007;32:E423–427. doi: 10.1097/BRS.0b013e318074d59f. [DOI] [PubMed] [Google Scholar]
- 4.Huang ZY, Yi BL, Liu HY. Sternal insufficiency fractures of post-menopausal women: retrospective analysis of 17 cases. Chin Med Sci J. 2012;27:101–105. [PubMed] [Google Scholar]
- 5.Lund JM, Chojnowski A, Crawford R. Multiple thoracic spine wedge fractures with associated sternal fracture; an unstable combination. Injury. 2001;32:254–255. doi: 10.1016/s0020-1383(00)00235-7. [DOI] [PubMed] [Google Scholar]
- 6.Andriacchi T, Schultz A, Belytschko T, Galante J. A model for studies of mechanical interactions between the human spine and rib cage. J Biomech. 1974;7:497–507. doi: 10.1016/0021-9290(74)90084-0. [DOI] [PubMed] [Google Scholar]
- 7.Oda I, Abumi K, Lu D, Shono Y, Kaneda K. Biomechanical role of the posterior elements, costovertebral joints, and rib cage in the stability of the thoracic spine. Spine (Phila Pa 1976) 1996;21:1423–1429. doi: 10.1097/00007632-199606150-00005. [DOI] [PubMed] [Google Scholar]
- 8.Takeuchi T, Abumi K, Shono Y, Oda I, Kaneda K. Biomechanical role of the intervertebral disc and costovertebral joint in stability of the thoracic spine. A canine model study. Spine (Phila Pa 1976) 1999;24:1414–1420. doi: 10.1097/00007632-199907150-00005. [DOI] [PubMed] [Google Scholar]
- 9.Oda I, Abumi K, Cunningham BW, Kaneda K, McAfee PC. An in vitro human cadaveric study investigating the biomechanical properties of the thoracic spine. Spine (Phila Pa 1976) 2002;27:E64–70. doi: 10.1097/00007632-200202010-00007. [DOI] [PubMed] [Google Scholar]
- 10.Watkins RT, Watkins R 3rd, Williams L, Ahlbrand S, Garcia R, Karamanian A, Sharp L, Vo C, Hedman T. Stability provided by the sternum and rib cage in the thoracic spine. Spine (Phila Pa 1976) 2005;30:1283–1286. doi: 10.1097/01.brs.0000164257.69354.bb. [DOI] [PubMed] [Google Scholar]
- 11.Korovessis P, Sdougos G, Dimas T. Spontaneous fracture of the sternum in a child being treated in a Boston brace for kyphoscoliosis. A case report and review of the literature. Eur Spine J. 1994;3:112–114. doi: 10.1007/BF02221450. [DOI] [PubMed] [Google Scholar]
- 12.Muldoon K, Chu P, Pathria M, Resnick D. Association of posterior rib fractures with exaggerated kyphosis and sternal collapse. Clin Imaging. 1999;23:311–313. doi: 10.1016/s0899-7071(99)00153-9. [DOI] [PubMed] [Google Scholar]
- 13.Stahlman GC, Wyrsch RB, McNamara MJ. Late-onset sternomanubrial dislocation with progressive kyphotic deformity after a thoracic burst fracture. J Orthop Trauma. 1995;9:350–353. doi: 10.1097/00005131-199509040-00014. [DOI] [PubMed] [Google Scholar]
- 14.Hills MW, Delprado AM, Deane SA. Sternal fractures: associated injuries and management. J Trauma. 1993;35:55–60. doi: 10.1097/00005373-199307000-00009. [DOI] [PubMed] [Google Scholar]
- 15.Brookes JG, Dunn RJ, Rogers IR. Sternal fractures: a retrospective analysis of 272 cases. J Trauma. 1993;35:46–54. doi: 10.1097/00005373-199307000-00008. [DOI] [PubMed] [Google Scholar]
- 16.Jones HK, McBride GG, Mumby RC. Sternal fractures associated with spinal injury. J Trauma. 1989;29:360–364. doi: 10.1097/00005373-198903000-00014. [DOI] [PubMed] [Google Scholar]
- 17.Gopalakrishnan KC, el Masri WS. Fractures of the sternum associated with spinal injury. J Bone Joint Surg Br. 1986;68:178–181. doi: 10.1302/0301-620X.68B2.3957997. [DOI] [PubMed] [Google Scholar]
- 18.Cooper KL. Insufficiency fractures of the sternum: a consequence of thoracic kyphosis? Radiology. 1988;167:471–472. doi: 10.1148/radiology.167.2.3357957. [DOI] [PubMed] [Google Scholar]
- 19.Klaase JM, Zimmerman KW, Veldhuis EF. Increased kyphosis by a combination of fractures of the sternum and thoracic spine. Eur Spine J. 1998;7:69–71. doi: 10.1007/s005860050031. [DOI] [PMC free article] [PubMed] [Google Scholar]